Article Text

Abstract
Introduction Governance is one of the most important aspects for strong primary healthcare (PHC) service delivery. To achieve the targets for the Sustainable Development Goals, good governance may play a prime role in low-income and middle-income countries (LMICs). This evidence gap map (EGM) explored the available evidence in LMICs to identify the knowledge gap concerning PHC policy and governance in these settings.
Methods We followed the standard 3ie EGM protocol, finalising the scope of the EGM through a stakeholder workshop. We searched a total of 32 bibliographic databases, systematic review databases, impact evaluation databases, and donor and bilateral agency databases using a comprehensive search strategy. Two reviewers screened retrieved studies, extracted data and performed quality assessment. We plotted the interventions and outcomes derived from the included studies in a dynamic platform to build the interactive EGM and conducted a stakeholder consultation with nominal group technique methods to prioritise the identified gaps.
Results The EGM included 24 systematic reviews and 7 impact evaluations focusing on PHC policy and governance in LMICs. Most of the sources emphasised workforce management and supervision. There were noticeable evidence gaps regarding accountability and social responsibility. The most highly prioritised themes were the role of accountability, the role of public–private partnerships and the role of user–provider communication in PHC governance.
Conclusions This EGM identified some important aspects of PHC policy and governance such as accountability, social responsibility, public–private partnership, user–provider communication through the methodological approaches of evidence synthesis and stakeholder consultation. Identified gaps will provide directions for an implementation research plan to improve the governance of PHC in LMICs.
- primary health care
- developing countries
- policy
- governance
- evidence gap map
- LMICs
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Governance arrangements and relevant policies are very crucial for sustainable and successful primary healthcare (PHC) system in low-income and middle-income countries (LMICs) and week governance may challenge PHC service delivery.
What are the new findings?
There are evidence gaps regarding PHC policy and governance in LMICs in terms of the roles of social accountability, public–private partnership and intersectoral collaboration.
There remains a large opportunity to implement interventions and strategies for better PHC governance in LMICs.
What do the new findings imply?
Findings from this evidence gap map provide the basis for planning implementation research with the aim of developing an accountable governance system in PHC.
Policy-makers and researchers will be able to plan and implement PHC governance strategies efficiently in the long run.
Introduction
The Alma-Ata declaration emphasised redefining and strengthening the role of governments in primary healthcare (PHC), mentioning intersectoral collaboration as a key catalyst for better health.1 Despite notable progress since the declaration, challenges remain in fulfilling health needs in many parts of the world, particularly for the vulnerable and the poor.2 PHC service delivery is often disrupted in many low-income and middle-income countries (LMICs) by emerging outbreaks, natural disasters, civil unrest or war,3 and the dual burden of disease (communicable and non-communicable).4 Governance of the PHC system can play a critical role in improving the performance, operation and resilience of the broader health system.5 Defining or conceptualising governance in health systems is always critical as it involves the interaction of the government with a diverse and broad range of actors6—including the community, private sector, non-government actors and non-health sectors—requiring collaborative policies and synergistic actions.
Governance refers to ensure the existence of policy and strategic frameworks in combination with oversight, regulation, coalition and accountability.7 In LMICs, the PHC governance has mostly been focused on delivering public sector services. However, private sector is also playing a vital role to address the components of PHC. The PHC governance should be consist of three interrelated components namely ‘integrated health service, multisectoral policy and action and empowered people and communities’ to oversee and guide both the public and private sector to protect public interest.7 8 Several authors have explored the role of governance in health systems, developing multiple frameworks. The Health Systems Governance Framework8 incorporated other existing frameworks that described the relationship of the state and market, the interrelationship between ministries and approaches such as people-centred services and focused on ten principles including participation, equity, accountability and transparency. Mikkelsen-Lopez et al published a governance model based on WHO’s building blocks of health systems incorporating additional elements such as long-term strategic vision, transparency, corruption, accountability and participation of different stakeholders.9 Others applied cultural theory to explore governance in health systems, describing hierarchical bureaucratic models and individualist approaches.10 Many bottom–up models have focused on non-government actors, especially service providers and users. The Accountability Mechanism Framework described the relationship between policy-makers and service providers in terms of bureaucratic accountability and described the responsiveness of citizens to the providers as external accountability.11 The multilevel framework of governance considered the challenges of providing PHC service delivery in LMICs. This framework described interactions between the government, communities and health markets, allowing each level to supplement the other in case of failure.6 The Primary Health Care Performance Initiative developed a global PHC framework with emphasis on people-centred care, functional mechanisms addressing both the supply and demand side, and effective service delivery involving community engagement, facility management and accessible comprehensive healthcare.4 Almost all of these models identified the implementing authority or policy-makers, service providers and users or community members as the most important stakeholders to play roles in the governance mechanisms of PHC.
PHC in LMICs differs from PHC in high-income countries in terms of resource mobilisation, coverage, access and governance. In the case of governance, high-income countries rely on available technologies such as health information technology or software for human resource management to ensure good governance, which are expensive and generally rare in LMICs.12 Instead, LMICs mainly focus on resources, access to care, attaining equity which are not main focus in high-income countries due to sufficient coverage of resources and services; LMICs focus less on governance than on the other building blocks of health systems.13 We aimed to construct an evidence gap map (EGM) to explore the available evidence in LMICs regarding PHC policy and governance. Exploring these gaps can provide the basis for future research and may identify potential areas where specific interventions are needed and appropriate. The objectives of this EGM are to identify the gaps around PHC policy and governance in LMICs based on available research and published evidence, prioritise the three most important thematic areas and plan implementation research to address the most important gaps.
Methods
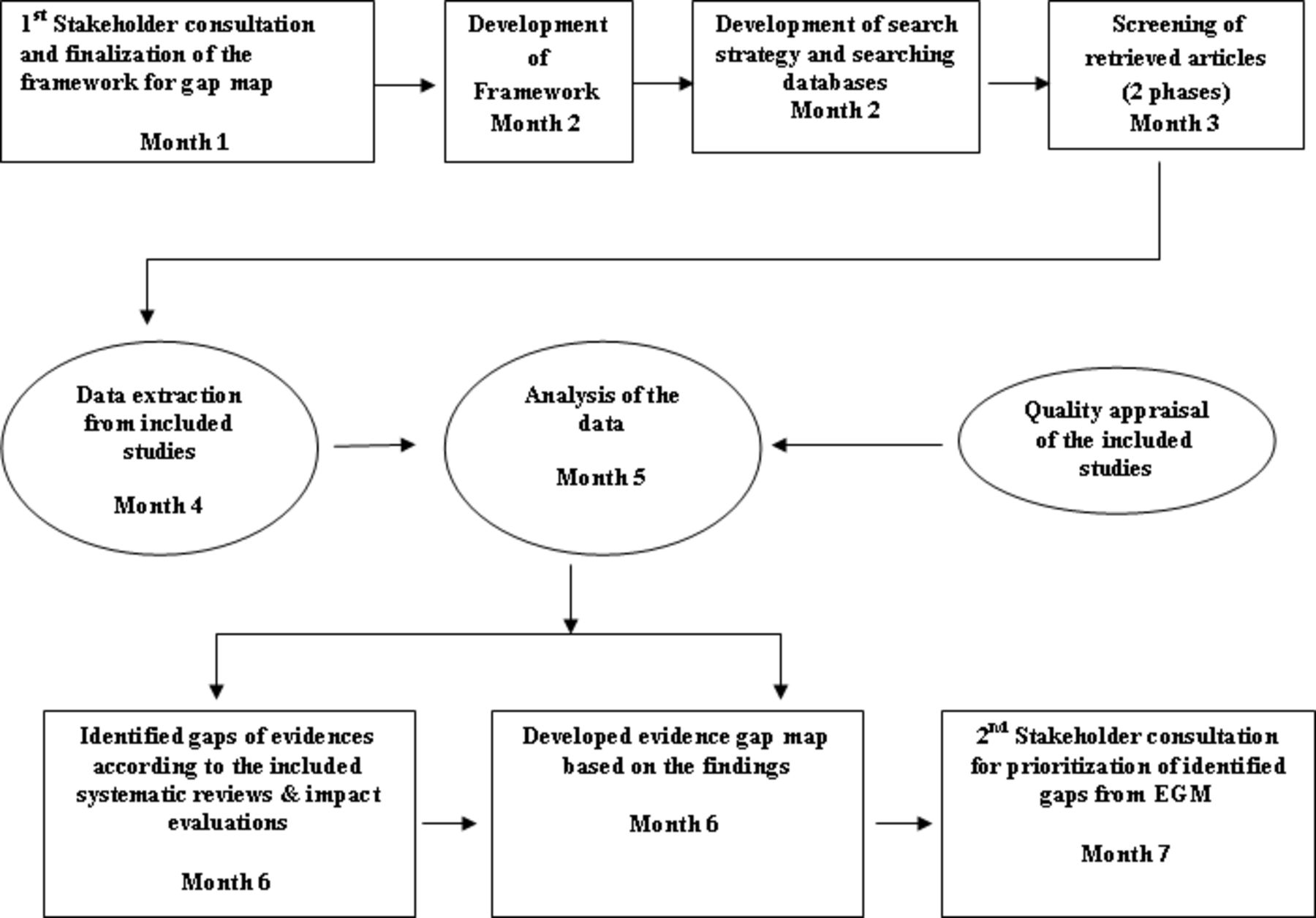
This EGM is consistent with the 3ie EGM Guidelines and Recommendations14 and has been reported according to the Reporting Standards for Systematic Evidence Syntheses guidelines.15 The scope of the EGM, conceptual framework and key search terms were finalised through a stakeholder consultative workshop. We organised the first stakeholder consultation in January 2018 to define the scope of the mapping. A total of 20 academics, researchers, and programme implementers attended the workshop. Through an extensive literature review and stakeholder consultation, we adapted the conceptual framework for improving PHC to the context of governance.16 The framework included a complete pathway from the broad health system to the impact on PHC and emphasises the interactions between providers, communities, and patients and the quality of services. The adapted framework demonstrated people—and community-centred care and supply-and-demand functions. The service delivery has been described based on effective workforce management and partnership among interplaying sectors. This framework focuses on key components that provide direction in achieving outcomes and, ultimately, broad impact.
To keep the scope appropriately narrow, we outlined some key categories to develop a comprehensive search strategy for inclusion of relevant literature. Because of the complexity of the term ‘governance,’ stakeholders also identified key terms which may play a direct or indirect role on governance, which we used for developing the search strategy and the framework of the EGM. We used a comprehensive strategy incorporating the key search terms such as ‘LMICs’,
‘Developing country’ ‘Health systems model’, ‘Governance model’, ‘Workforce management’, ‘Community engagement’, ‘Public private’, Policy, Governance, Accountability, ‘Social responsibility’, Compliance to search 32 electronic bibliographic databases, impact-evaluation databases, systematic-review databases, and databases of bilateral agencies, the United Nations and international non-governmental organisations (NGOs) and applied a prespecified set of criteria to select studies for inclusion.16 The major databases were MEDLINE through PubMed, Cumulative Index of Nursing and Allied Health Literature, Web of Science, Informit Humanities, Popline, Scopus, Social Sciences, 3ie Impact Evaluation Repository, Cochrane Database of Systematic Reviews, Evidence for Policy and Practice Information and coordinating Centre systematic reviews database, Joanna Briggs systematic reviews, PHC evidence, Campbell Collaboration database and 3ie database of systematic reviews. We included the studies performed in LMICs17 or systematic reviews that incorporated studies from high-income countries and LMICs. We searched for programme and interventions implemented by governments, NGOs, international organisations or funding agencies to manage PHC policies and governance. We organised outcomes by the study objectives and categorised them by broad themes, for example, facility management, quality of care, and compliance. We included both impact evaluations and systematic reviews of effects on PHC policy and governance. We excluded non-systematic literature reviews, ongoing trials and reviews, trial or review protocols, letters to the editor, editorial comments, conference papers, articles published before January 1980 and written in languages other than English.
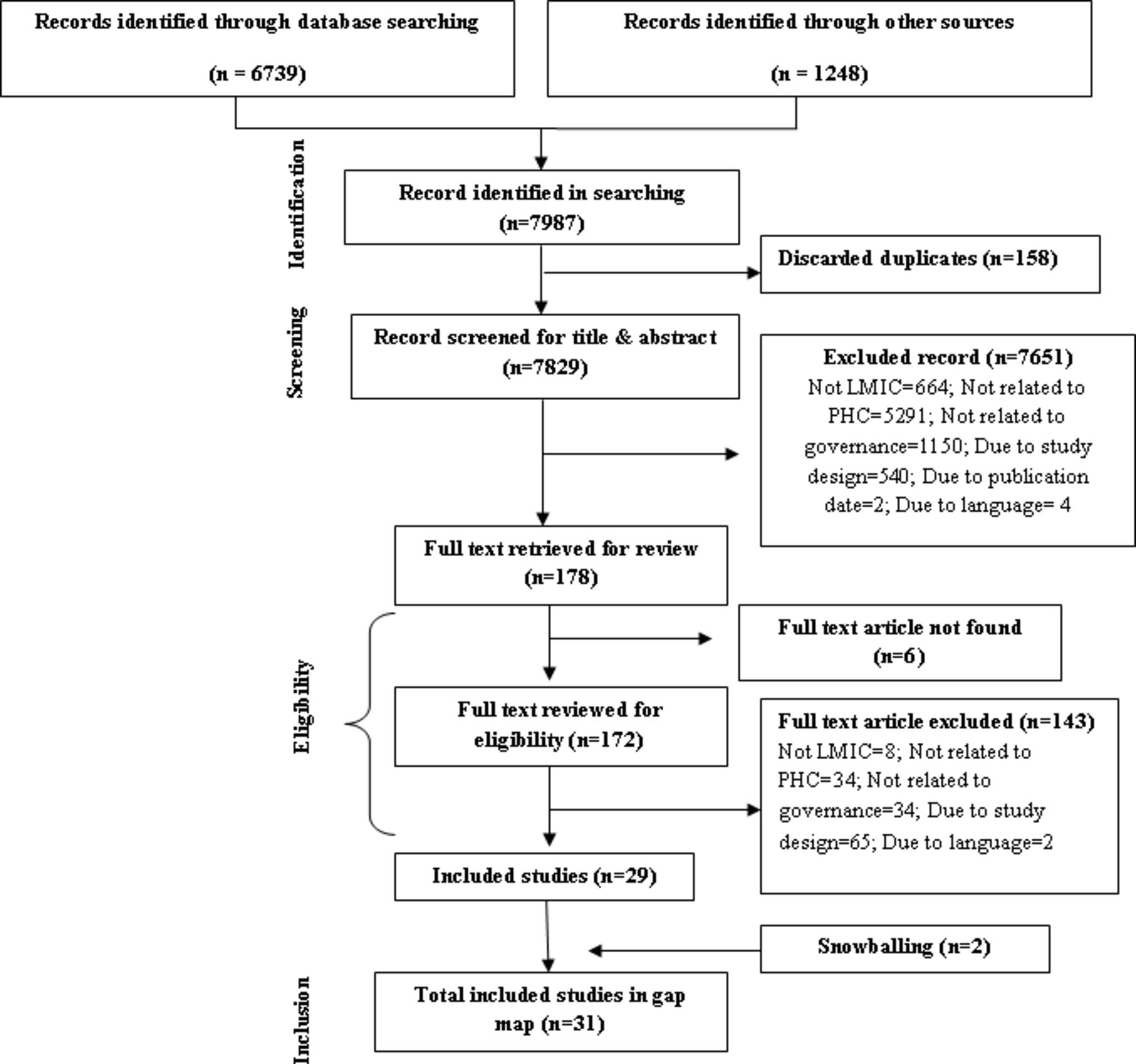
We screened articles in two phases (figure 2). Two independent reviewers first screened titles and abstracts of the articles to determine inclusion in the study based on the predefined inclusion and exclusion criteria. Second, two reviewers independently assessed initially included articles based on the full text to finalise the sample. The reviewers resolved any disagreements through discussion with a third reviewer. Two reviewers independently extracted information using a standardised form (online supplementary file 1). A third reviewer randomly checked the data extraction process and resolved any disagreements between the primary reviewers. Two reviewers independently assessed the quality of the included systematic reviews using modified version of ‘Supporting the Use of Research Evidence’ checklist.14 Reviewers rated each systematic review as having high-grade, medium-grade or low-grade evidence. A third reviewer checked and finalised the assessment. We did not assess the quality of included impact evaluations.
Supplemental material
We analysed the interventions and outcomes of the systematic reviews and impact evaluations in a descriptive synthesis. Additionally, we mapped the geographical distribution of included articles and calculated the frequency of interventions. We plotted identified interventions in rows and outcomes in columns in a dynamic platform to develop a gap map where each intervention (rows) and their outcomes (column) are plotted to visualise the gap. We plotted studies in multiple places in the visual gap map if those studies considered more than one outcome or intervention and colour coded the plot according to evidence quality. The detail methodology, including the scope of the EGM, conceptual framework and search strategy, has been described in the published protocol.16
Prioritisation of identified gaps through second stakeholder’s workshop
We organised the second stakeholder consultation workshop to identify the highest priority areas from the identified gaps in the EGM. Total 20 national experts of Bangladesh including persons leading the government PHC system, researchers both from government and autonomous bodies, academics from public and private universities, development partners working on PHC were engaged in the prioritisation process. We developed a ‘score card’ to prioritise the top three gaps using a nominal group technique. The score card consisted of contextual factors such as service coverage, human resource, stewardship, social, cultural, political context and communication perspective. These factors were proposed by the research group and agreed by the stakeholders. Each participant scored and ranked the identified gaps to prioritise them independently. Maximum point for each factor was 3 whereas minimum point was 1. Participants reached consensus on the final three high-priority themes through discussion. The score card has been provided in online supplementary file 2. Stakeholders prioritised the topics with an intention to plan implementation research in Bangladesh for the better governance of PHC and expected on the basis of their experience and expertise, that these will be applicable to other LMICs as well.
Supplemental material
Implementation research plan
The research team developed an implementation research plan based on their experience to address the prioritised gaps. We shared an initial draft of the research plan with policy-makers who attended the prioritisation workshop and finalised it with their input.
A flow diagram of the EGM methodology has been demonstrated in figure 1.
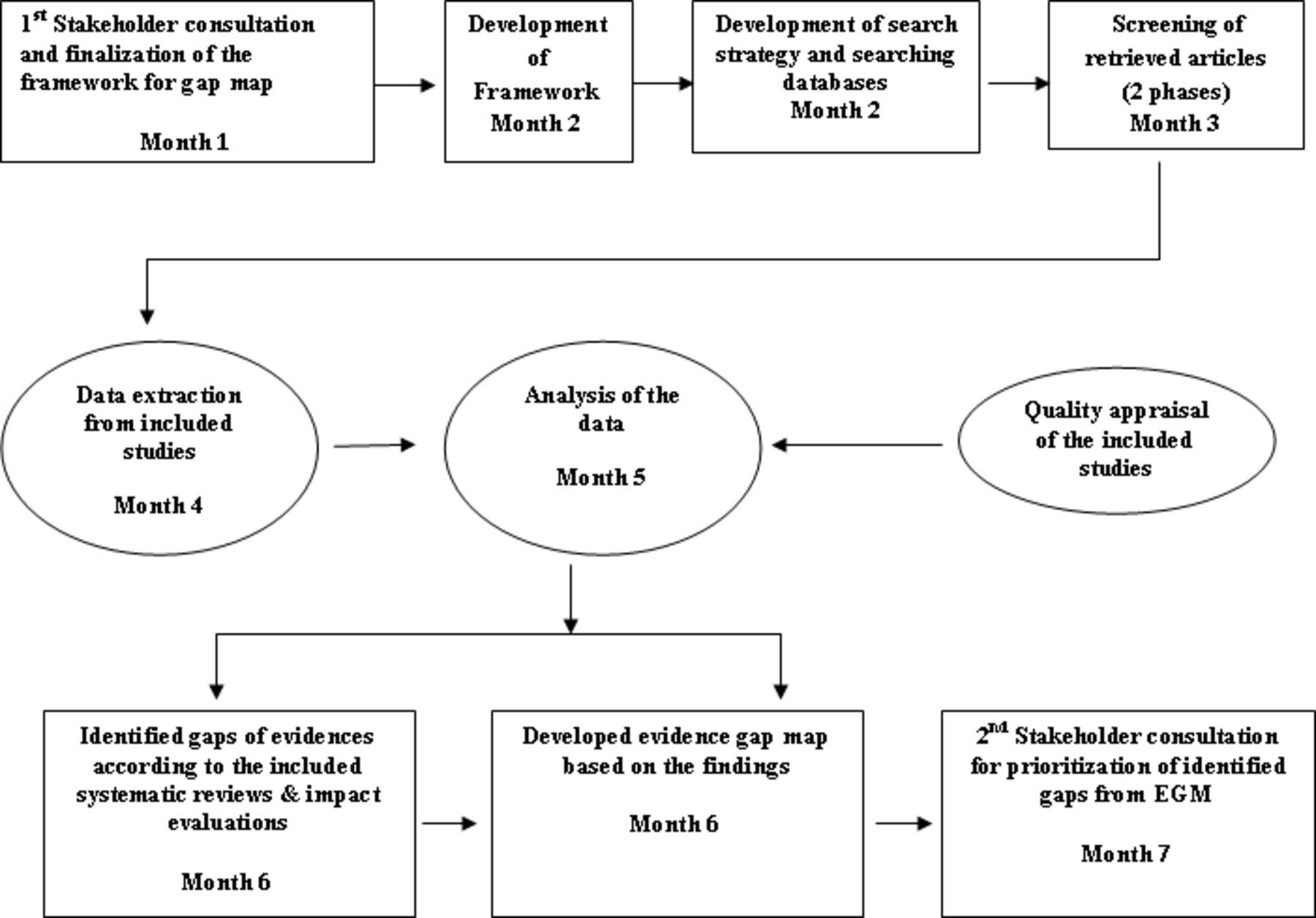
Flow diagram of EGM methodology and prioritisation of identified gaps. EGM, evidence gap map.
Patient and public involvement
This EGM is based on available published works, and there is no direct involvement of patients and public in the whole process of EGM. The findings of this EGM can be used for the overall betterment of PHC for public and patients.
Results
Our search strategy identified a total of 7987 citations from relevant databases. After removing duplicates, we screened 7829 citations based on titles and abstracts. Of those, we assessed 178 full-text articles for eligibility (figure 2). Thirty-one studies met the eligibility criteria and were included in the final analysis.
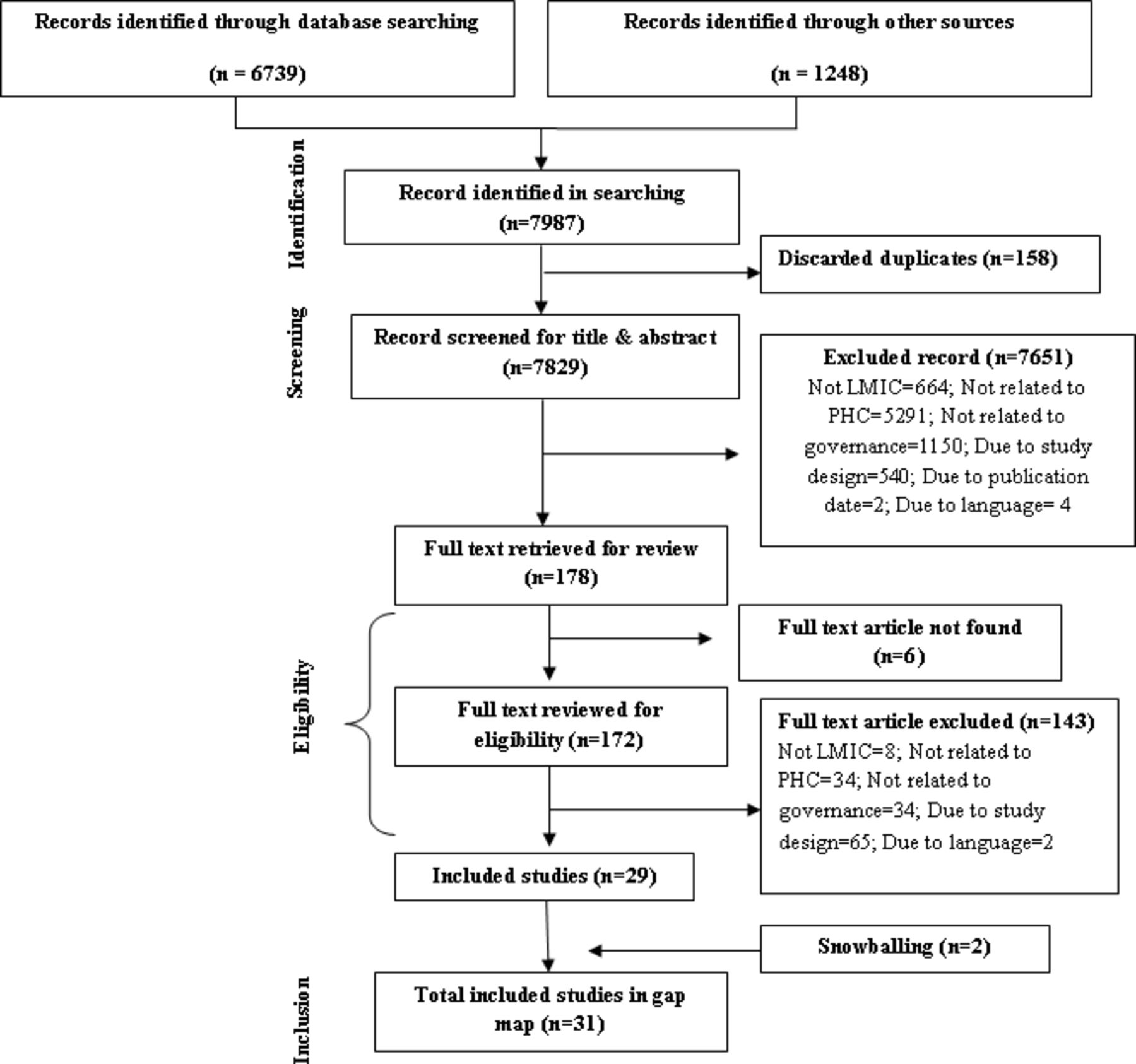
Flow diagram of included articles using ROSES. LMIC, low-income and middle-income country; PHC, primary healthcare; ROSES, Reporting Standards for Systematic Evidence Syntheses.
Characteristics of included studies
We included a total of 24 systematic reviews and 7 impact evaluations in the EGM (table 1). All studies but one was published between the years 2005 and 2017. All but one of the impact evaluations followed a quantitative study design; among those, most (n=3) were quasi-experimental, before-and-after studies. The remainder used baseline and follow-up surveys, pre–post interventions, time series designs or randomised controlled trials.
List of the included studies: systematic reviews
Quality assessment of the systematic reviews
Most of the included reviews had clear inclusion criteria (n=19), used partially comprehensive searches, and reported required outcomes (n=13). Nine studies did not use appropriate data analysis methods, and eight studies used partially appropriate methods. A majority of the reviews (n=15) mentioned bias, but only five of them assessed study bias appropriately (figure 3).
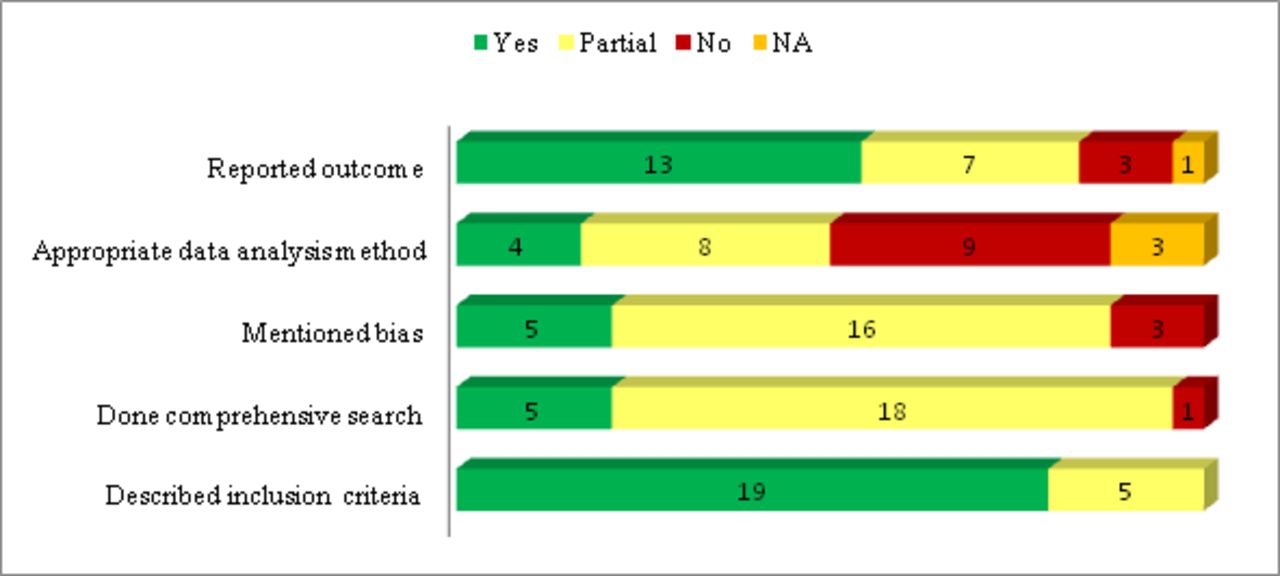
Distribution of systematic reviews by major quality-assessment criteria.
More than half of the systematic reviews (n=17) rated the included studies as having poor quality. The remaining systematic reviews rated the included studies as having moderate and good quality (n=5 and n=2, respectively).
Geographical location of the existing evidence
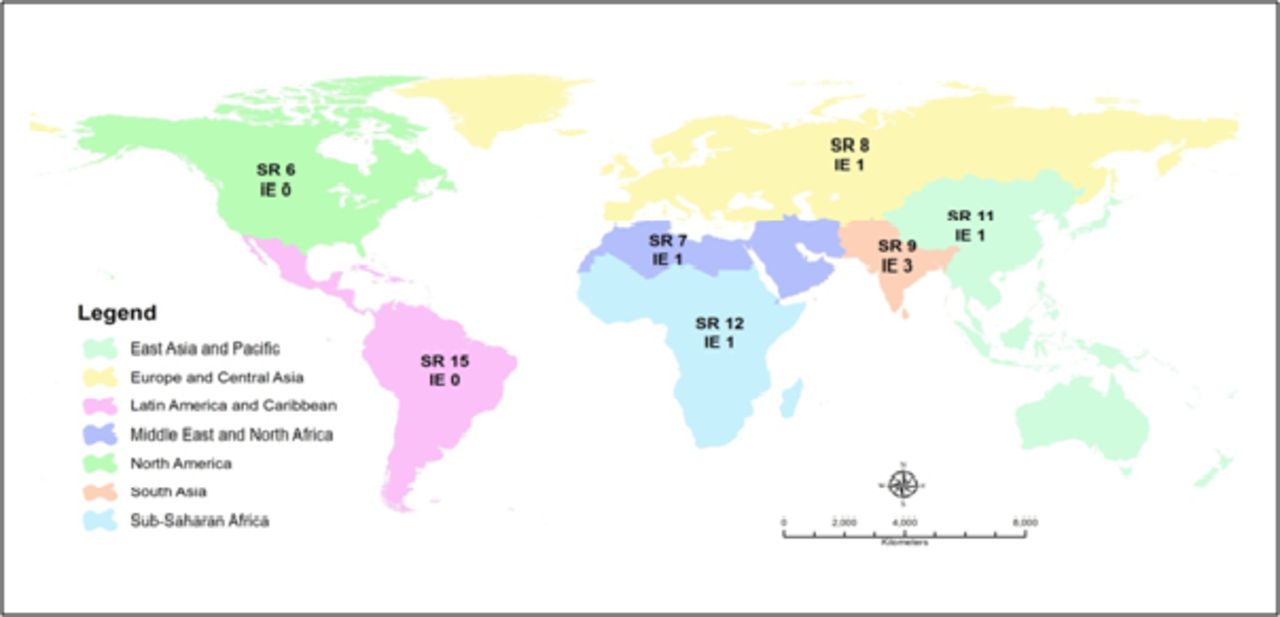
Among the included studies, most systematic reviews provided evidence from the Latin America and Caribbean region (n=15); whereas, no impact evaluations originated from that region. Three of the included impact evaluations originated in South Asia, but the remaining four impact evaluations came from four different regions. The remaining systematic reviews reported evidence from the Sub-Saharan Africa region (n=12) followed by the East Asia and Pacific region (n=11). Some systematic reviews included studies from both high-income countries and LMICs, which we also included in the geographical distribution (figure 4).

Geographical distribution of articles (IE: Impact Evaluations and SR: Systematic Reviews) by world bank region.
Interventions focused on PHC policy and governance
The most frequent thematic area of interventions was workforce management (n=13; SR=12, IE=1),18–30 including decentralisation of health workforce, provision of financial incentives and career promotions to physicians, doctor–nurse substitution, consideration of lay health workers as health workforce, provision of training to lay health workers, and establishment of new medical schools (table 1). Community engagement was the second most prioritised area of intervention (n=7; IE=3, SR=4)27 31–36 followed by health system model (n=7; IE=1, SR=6).20 31 34 37–40 Two impact evaluations and four systematic reviews addressed workforce supervision as a part of the performance assessment of health workforce.33 41–45 A few systematic reviews focused on infrastructure, including purchasing of new equipment, establishment of new PHC facilities and improvement of existing infrastructure such as size and availability of consulting rooms and availability of required equipment.24 26 27 Interventions related to user fees were rare33 46; one study reported on setting lower fees for receiving PHC compared with that of secondary healthcare, and another focused on standardisation of user fees for purchasing medicines. A small number of reviews considered referral,26 user–provider communication,26 public–private partnership33 and contracting out.47
Some systematic reviews lacked evidence demonstrating the broad impact of the interventions but focused instead on showing relevant outcomes in one or more specific areas.24 27 37 39 For example, a systematic review conducted in Brazil39 assessed the accessibility and quality of health service coverage in the PHC system. Another study reviewed the Iranian health system model, focusing on decentralisation.37 Another review focused on the relationship between health workforce performance and quality of care.19 Another study summarised an extensive review of PHC systems in South America27 focusing on decentralisation of administrative and fiscal issues and reformation of health systems.
Outcomes focused on PHC policy and governance
Examples of PHC service coverage, the most commonly measured outcome (n=18; 13 SR,22–25 27 33 38 39 41–43 46 47 5 IE30 35 44 45 48), included improved immunisation coverage, outcomes for selected infectious diseases, disease-screening coverage and healthcare coverage among the poor. Improved PHC service coverage ultimately resulted in improved health status. Seventeen studies (11 SR, 6 IE) highlighted quality of care as an outcome,19 21 26 28 31 32 34 35 38 39 41 43–45 47 48 focusing on reduction of child and neonatal mortality and morbidity, improvement in people-centred care and promotion of successful implementation of PHC. They also reported on PHC facilities with sufficient equipment, essential medicines and skilled health workforce, with improved health outcomes and with increased duration spent on direct patient care.
Evidence from nine systematic reviews19 20 26 27 31 32 38 40 47 and three impact evaluations30 35 48 showed that interventions focused on a suitable health system model, a contracting-out process, workforce management, infrastructure, intersectoral collaboration and community engagement could bring changes in access to healthcare. Eight systematic reviews18 20 22 24 26 28 29 41 and one impact evaluation34 assessed the availability of workforce as an outcome of specific interventions. Four studies identified health systems reform defined by decentralisation of workforce31 37 and infrastructure reform.20 40 Eight studies used compliance as an outcome,18 21–23 25 26 38 46 and two studies19 32 mentioned ‘accountability’ during the provision of healthcare.
GapMap
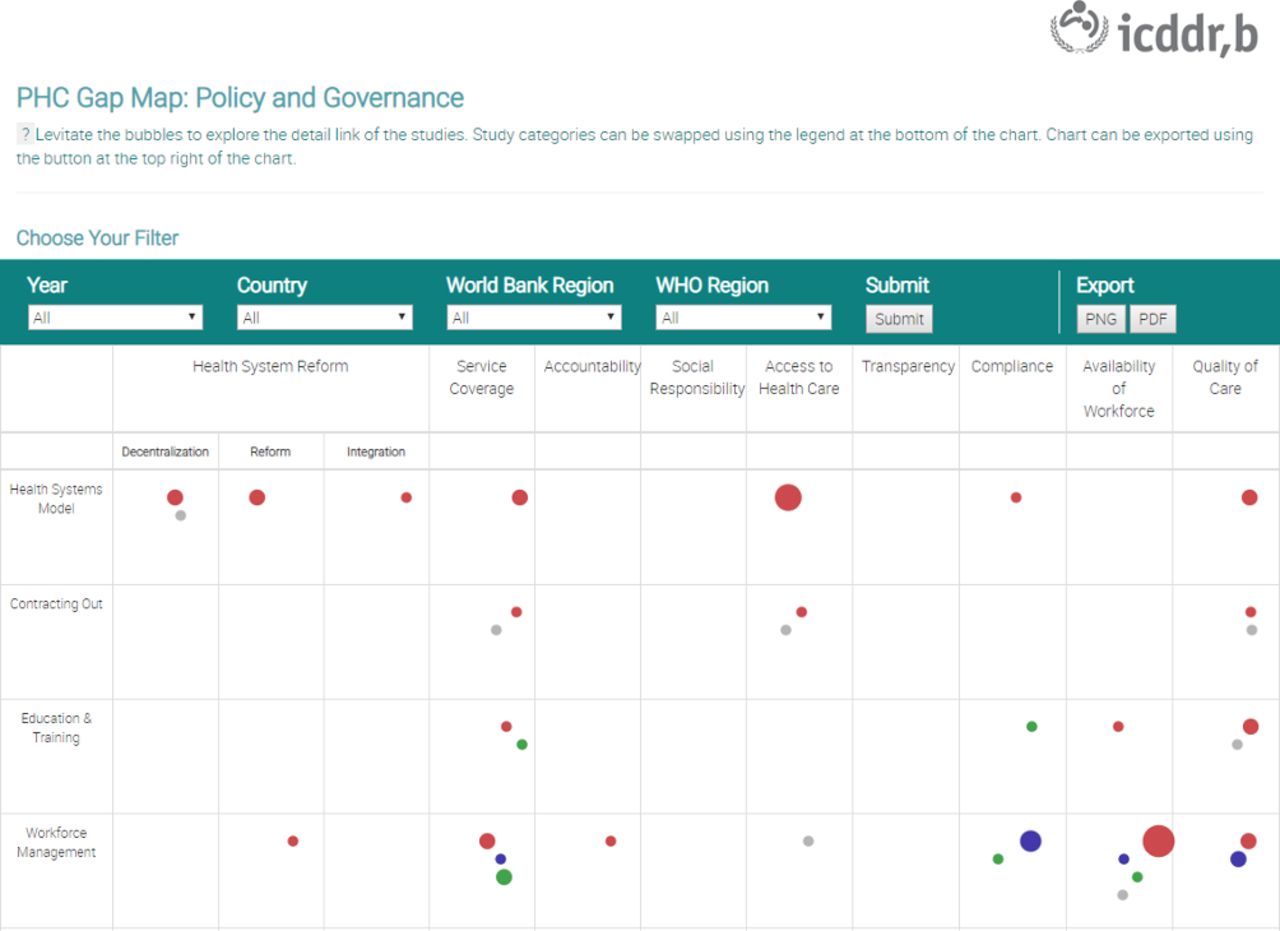
We developed an interactive web-based gap map (www.evidencesynthesisbd.com, figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
An illustration of the interactive evidence gap map on PHC policy and governance. PHC, primary healthcare.
Identified gaps and prioritised themes
The EGM analysis identified several gaps in PHC policy and governance:
Interventions to improve accountability for better governance in PHC.
Role of social responsibility in governance of PHC.
Interventions to ensure transparency in local-level decisions making and governance.
Role of contracting out to provide PHC service, and the governance of the contracting process.
Interventions on proper referral system to improve PHC and the governance of the referral system.
Role of external aid in PHC governance.
Role of public–private partnership in PHC governance to improve community leadership and mutual accountability.
Role of user–provider communication in PHC to increase awareness and demand from user end which ensure better service and governance.
Interventions on purchasing and payment models to improve PHC governance.
Interventions to improve intersectoral collaboration for better governance of PHC.
During the second consultative workshop, stakeholders determined the three highest priority areas for conducting implementation research for better PHC governance. Stakeholders considered the local context of Bangladesh during prioritisation and it was expected to be applicable in other LMICs based on their experience. The prioritised topics were (1) interventions to improve accountability for better governance in PHC (2) role of public–private partnership in PHC governance to improve community leadership and mutual accountability and (3) role of user–provider communication in PHC to increase awareness and demand from user end which ensure better service and governance.
Additionally, stakeholders strongly recommended that implementation research be conducted in the identified areas.
Next steps for implementation research
To address the highest priority thematic areas, we planned implementation research to improve accountability and governance through a public–private partnership initiated by a community support group (CSG), to enhance user–provider communication in providing PHC, and to establish a parafinancing mechanism to support additional needs through a CSG. We propose conducting 36 months of implementation research, employing a mixed-methods approach. Implementation research will facilitate health systems strengthening and support the scale-up and integration of interventions at the national level.
Discussion
This EGM mapped the available impact evaluations and systematic reviews on policy-related and governance-related PHC interventions in LMICs. Some studies did not mention specific interventions but instead highlighted focused areas responsible for the improvement of governance-related issues in PHC; other studies presented multiple interventions interacting to affect one type of outcome. We found impact evaluations most often evaluated the impact of community engagement interventions.34–36 Other impact evaluations considered contracting out PHC services,48 workforce management interventions30 and introducing a new health system model.34
Most of the evidence from systematic reviews focused on workforce-related interventions. Specifically, studies reviewed workforce management interventions more frequently than workforce supervision interventions. Workforce-related PHC interventions included decentralising the health workforce, providing education and training to healthcare workers, providing financial incentives or career promotion to healthcare workers, substituting nurses for doctors and establishing new medical schools. Most studies were methodologically poor considering the points for quality assessment checklist14 such as clear inclusion criteria, comprehensive search strategy, outcome reporting, data analysis methods and assessment of bias.
The second largest bodies of evidence focused on the health system model and on community engagement; though, the studies were also of poor methodological quality. Other categories of interventions such as infrastructure, intersectoral collaboration and user fees had limited evidence from systematic reviews. Some categories—public–private partnership33 and user–provider communication26—appeared in only one study each. Still, we believe these interventions have important roles to contribute in PHC. No systematic review provided evidence on purchasing or external aid interventions. No impact evaluation provided evidence on purchasing, intersectoral collaboration, public–private partnership, external aid, user–provider communications, user fees or referral interventions.
There are notable gaps in the evidence for several interventions and outcomes in impact evaluations and systematic reviews. Evidence concentrated around outcomes related to service coverage, availability of workforce and quality of care. Fewer studies measured outcomes related to health system reform, including decentralisation of health facilities and workforce and integration of new facilities. Most evidence from impact evaluations concentrated on outcomes related to quality of care; impact evaluations reported on very few other outcomes related to PHC and not at all on outcomes concerning reform of the health system and integration of new facilities, accountability, transparency and compliance. Additionally, few systematic reviews assessed impact on outcomes concerning accountability and integration of new healthcare facilities (two and one review, respectively). No systematic review addressed social responsibility as an outcome, and only one impact evaluation assessed this outcome. Virtually no studies reported on transparency.
Limitation of the EGM
This EGM includes only 7 impact evaluations and 24 systematic reviews as the research question and inclusion criteria set for the study limited the potential literature to be included. We included only English-language studies, and we did not include any unpublished work.
It was occasionally difficult for the study team to categorise interventions, especially when the ‘intervention’ was only a description of an existing health system or other circumstances of a country. In many cases, insufficient reporting of intervention characteristics increased the challenge. Therefore, we categorised interventions based on area of focus.
Conclusion
Applying rigorous synthesis methods, we identified issues related to policy and governance that are still understudied in LMICs. Interventions to improve accountability, social responsibility, public–private partnership, user–provider communication are the main identified gaps. To improve PHC governance and service delivery in LMICS, future implementation researches are recommended, specifically addressing gaps in the areas of accountability, public–private partnership, CSG formation to enhance user–provider communication and para-financing mechanisms.
Acknowledgments
We acknowledge Lisa Hirschhorn, Senior Advisor of Primary Health Care at Ariadne Labs and Dan Schwarz, Associate Director of Primary Health Care at Ariadne Labs with gratefulness for their support and guidance with this study. icddr,b is also grateful to the Governments of Bangladesh, Canada, Sweden and the UK for providing core/unrestricted support.
References
Footnotes
Handling editor Seye Abimbola
Contributors KMS-U-R: led the development of proposal, study design and research implementation. Conducted evidence synthesis, drafted initial paper and revised. RM: aided in the development of proposal, evidence synthesis and drafting the manuscript. IN: conducted evidence synthesis, contributed in narrative synthesis and drafting the manuscript. SH: guided the workshop, provided critical input all manuscript revisions. TR: conducted evidence synthesis, helped in drafting the manuscript. EK: contributed in workshops, helped in drafting the manuscript. AR: guided proposal development, involved in all manuscript revisions. ND: provided input to manuscript revisions KI: guided development of proposal, conducted workshop and revised manuscript. IA: guided development of proposal, conducted workshop and revised all versions of the manuscript.
Funding This publication is based on research funded by Ariadne Labs through Brigham and Women’s Hospital, who is the recipient of a Bill & Melinda Gates Foundation grant. The findings and conclusions contained within are those of the authors and do not necessarily reflect positions or policies of the Bill & Melinda Gates Foundation.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.