Article Text

Abstract
Introduction Donor transition for HIV/AIDS programmes remains sensitive, marking a significant shift away from the traditional investment model of large-scale, vertical investments to control the epidemic and achieve rapid scaling-up of services. In late 2015, the United States President’s Emergency Plan for AIDS Relief (PEPFAR) headquarters instructed their country missions to implement ‘geographic prioritisation’ (GP), whereby PEPFAR investments would target geographic areas with high HIV burden and reduce or cease support in areas with low burden.
Methods Using Gaventa’s power cube framework, we compare how power is distributed and manifested using qualitative data collected in an evaluation of the GP’s impact in Kenya and Uganda.
Results We found that the GP was designed with little space for national and local actors to shape either the policy or its implementation. While decision-making processes limited the scope for national-level government actors to shape the GP, the national government in Kenya claimed such a space, proactively pressuring PEPFAR to change particular aspects of its GP plan. Subnational level actors were typically recipients of top-down decision-making with apparently limited scope to resist or change GP. While civil society had the potential to hold both PEPFAR and government actors accountable, the closed-door nature of policy-making and the lack of transparency about decisions made this difficult.
Conclusion Donor agencies should exercise power responsibly, especially to ensure that transition processes meaningfully engage governments and others with a mandate for service delivery. Furthermore, subnational actors and civil society are often better positioned to understand the implications and changes arising from transition. Greater transparency and accountability would increase the success of global health programme transitions, especially in the context of greater decentralisation, requiring donors and country counterparts to be more aware and flexible of working within political systems that have implications for programmatic success.
- public health
- health systems evaluation
- health policy
- qualitative study
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ABOUT THIS TOPIC
Funding agencies hold significant power in the decisions on whether to transition their programmes and when, and power asymmetries exist also within decentralised donor agencies stimulating a disconnect between global decision-makers and national governments.
WHAT THIS STUDY ADDS
Our analysis revealed missed opportunities in creating spaces for consultation and coordination, especially with regard to subnational actors in decentralised settings.
We also identify the potential held by the United States President’s Emergency Plan for AIDS Relief (PEPFAR) implementing partners and local civil society to create spaces that engage and create bridges across the development partner and national government divide.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Transition policies, such as PEPFAR’s geographic prioritisation, should be designed more collaboratively, with greater transparency and more flexibility for country governments, especially at the subnational and local levels.
Introduction
As countries advance from low-income to middle-income status, they are likely to observe a transition in funding and technical assistance provided by multilateral and bilateral aid agencies. Triggered by a combination of advances in economic development, the achievement of health programme goals, and, sometimes, a shift in donor priorities, transitions involve the conclusion of one or more types of financial, programmatic or technical support to various health programmes.1 While some multilateral agencies, such as the Global Fund to Fight HIV/AIDS, Tuberculosis and Malaria (GFATM) and Gavi—The Vaccine Alliance, describe the triggers and preparation for transition,2 3 not all initiatives do so. The cessation of donor support is inevitably a political process,4 involving negotiations, some open, others closed, and tension between donor and country priorities.
The financing of many HIV/AIDS programmes remained donor-dependent, making their transitions particularly sensitive. Donor support for HIV/AIDS epidemic control often forms the foundation for programmes for key populations, for whose care there may be limited domestic and local political commitment4 as well as millions that need lifelong medical care. Because of the politics of HIV/AIDS and the many actors involved in implementing HIV/AIDS programmes, transition can trigger tensions around mandate and responsibilities across multiple levels of governance—involving both national partners and international ones. Evaluations that aim to establish the effects and implications of donor transitions exist,5–11 although rarely explicitly focused on power and politics. Using data from an evaluation of the impact of the United States President’s Emergency Plan for AIDS Relief’s (PEPFAR) geographic prioritisation (GP) in Kenya and Uganda, we use power analysis to better understand the political actors and processes at play.
PEPFAR has been a significant funder of HIV/AIDS programmes across the world, particularly in Eastern and Southern Africa since the early 2000s.12 In 2015, PEPFAR launched a transition policy aimed to create more sustainable HIV control ‘by pivoting to a data-driven approach that strategically targets geographic areas and populations’ as opposed to generalised national responses.13 In late 2015, PEPFAR instructed country missions to geographically prioritise their programmes, whereby PEPFAR investments were targeted at geographic areas with high HIV burden with the goal of accelerating achievement of the United Nations Programme on HIV/AIDS (UNAIDS) 90-90-90 targets.1 Three categories of support for subnational units (SNUs) were identified: scale-up (highest burden areas that receive additional support to accelerate progress towards at least 80% antiretroviral (ARV) treatment coverage); maintenance (areas with little to no change in the amount of support, would be scaled-up aggressively eventually) and central support (CS) (areas with lowest burden, would be transitioned to government or other support). Within these classifications, the SNUs refer to districts or counties, and sites refer to health facilities, which were also transitioned in some cases. The guidance PEPFAR issued to country missions suggested that transition and other changes in SNU support would take place within the same fiscal year, although no guidance was provided for implementing this process.14
In this paper, we compare how power is distributed and manifested in the context of the initial implementation of PEPFAR’s GP in Kenya and Uganda, between 2015 and 2018, drawing on Gaventa’s power cube framework. This is important because much writing about donor transition reflects an implicit understanding of asymmetries of power between countries and funding agencies, which are typically viewed to be relatively powerful in terms of deciding when and how to transition.15 16 However, a simple dichotomous understanding of the role of power in shaping transition is problematic for several reasons. First, both the development literature and global statements proposed that effective development practice should enable national government leadership and the alignment of development partners with country needs. We wished, in part, to understand the extent to which this is really the case in transition. Second, domestic and international actors involved in transition are far from being homogenous groupings. For example, international actors could be positioned within global headquarters (HQ), country offices of a development partner or within firms involved in implementation, each of which may have different types of power and authority. Finally, and reflecting the second point, the nature of transition decision-making is likely a reflection of networks of power and how different actors collaborate or communicate to influence transition decisions.17 Understanding the nature of these networks, and how communication flows between them during transition may offer insight into how more collaborative transition processes can be achieved.
Methods
Research design
This analysis relies on data collected as part of a United States Agency for International Development (USAID) -supported mixed-methods evaluation of the impact of PEPFAR’s GP on CS SNUs and health facilities in Kenya and Uganda. The evaluation was carried out between 2016 and 2018 by faculty from Johns Hopkins University School of Public Health in collaboration with colleagues from Makerere University School of Public Health (MakSPH) and IPSOS-Kenya through USAID’s Project SOAR - Supporting Operational AIDS Research. The evaluation sought to understand how the transition from PEPFAR support to central government support affected the delivery and coverage of HIV and priority non-HIV services. Results from the evaluation and more detailed accounts of the data that were collected and analysed as part of this evaluation are documented elsewhere.8 18–24
This article re-analyses qualitative data to document the process and impacts of implementing the PEPFAR’s GP strategy with a particular lens on the power dynamics involved in the process. Data include two rounds of national-level interviews describing the nature of the GP strategy and plans for its implementation, and longitudinal case studies of purposefully selected facilities that included multiple respondents at each facility. This analysis was not part of the original scope of the evaluation, but sufficient power-related themes emerged from our initial analysis that they warranted additional exploration.
Country transition context
Table 1 provides an overview of the HIV/AIDS context in Kenya and Uganda, as well as a summary of the SNUs’ geographic prioritisation classification. In Kenya, the seven CS counties were primarily located in Northeastern Kenya plus one coastal county. In Uganda, CS districts were identified by an algorithm that primarily considered HIV prevalence (ie, HIV prevalence <0.6%) and were largely in the east of the country. In many Ugandan CS districts, USAID and PEPFAR planned to retain regional-level mechanisms for supporting districts.14
HIV/AIDS context and geographic prioritisation summary in Kenya and Uganda, at the time of the evaluation in 2018
Data collection
National-level semi-structured interviews in each country were conducted in May and November 2017 by researchers from the Johns Hopkins University School of Public Health (JHSPH) in collaboration with colleagues from Makerere University School of Public Heealth (MakSPH) and IPSOS-Kenya. Some interviews were conducted in teams, involving researchers from JHSPH as well as from the country partner teams. Informants were purposively selected from US government (USG) agencies (primarily USAID), PEPFAR implementing partners (IP)—that is, international or local non-governmental organisations (NGOs) contracted by PEPFAR to implement PEPFAR-funded projects, relevant units of the national government, civil society organisations (CSOs) and selected other donor agencies—based on their perceived knowledge of and role in the GP process or based on whether they were providing financial support to HIV services. No non-US donor agencies were included in the interviews in Kenya. Other donor agencies were operating in the area affected by GP, but they were not supporting HIV services. In Uganda, some non-US donor agencies were included in our first round of interviews if they were financing HIV services or if they were potentially operating in the areas affected by the GP. However, our interviews found minimal involvement or financing, and as such, this type of respondent does not feature prominently nor were they included in round 2 interviews. The analysis presented in this article is based on interviews with 23 national-level stakeholders in Kenya, and 40 in Uganda. In both countries, we had repeat respondents between rounds 1 and 2 of data collection.
In addition, longitudinal case studies were conducted in six to seven CS facilities in each country to capture the local experience of GP, including perspectives from subnational government officials, facility managers, IPs and patients. In Uganda, MakSPH conducted a total of 62 semi-structured interviews (34 in round 1 and 28 in round 2, with overlap). In Kenya, IPSOS-Kenya conducted a total of 36 semi-structured interviews (16 in round 1 and 20 in round 2, with overlap). Among the case study interviews, we draw only on analysed the interviews with district/county health managers, facility staff and IPs. Patient perspectives are explored in-depth as part of other publications.23 24 Table 2 summarises the number of interviews and types of respondents in each country, per round. All of the interviews used in this article were conducted in English, per the preference of the respondent.
Summary of respondents, by type, country and data collection round
Our project teams presented findings from the analysis as part of half-day workshops with USG, CSOs, IP stakeholders in early 2018, separately in Kenya and Uganda. The purpose of this workshop was to present and validate overall findings from the evaluation with concerned stakeholders. The power cube analysis was not discussed at that time, however, this consultation touched on and confirmed some of the issues that we draw on in the current paper.
Data analysis
We draw on Gaventa’s power cube framework to conceptualise the various forms of power at play in the context of the GP. The power cube arose from Gaventa’s efforts to ‘make the implicit power perspective more explicit’.25 It suggests three dimensions of power previously elaborated by Lukes,25 26 in relation to spaces, levels and forms (see box 1).25 Analysis entails an examination of the continuum of spaces of participation, how they are created, based on what interests and through what forms of engagement,25 to facilitate understanding each dimension individually, as well as in context of the other two dimensions. Because donor transition involves a unique set of actors, we first conduct a mapping of stakeholders, vis-à-vis the power cube levels. We then examine all the power cube dimensions through the data that we have available from Uganda and Kenya and reflect on cross-country learnings about power manifestations in the context of donor transitions.
Power cube dimensions
Dimension 1: decision-making spaces:
Closed: stakeholders making decisions ‘behind closed doors’, without any attempts to enhance participation.
Invited: stakeholders—usually officials or authorities—take deliberate measures to enhance participation, particularly of users or beneficiaries.
Claimed/Created: less powerful actors create or take over decision-making spaces, often organically and outside of ‘institutionalised arenas’.25
Dimension 2: places and levels where various forms of power (social, economic, political) exist:
The arenas that form in response to bureaucratic arrangements.
Reflecting on the spheres and arenas that form at local, national and global levels, recognising that they are inter-related and their inter-relationships can be messy in light of political processes, such as decentralisation.25
Forms and visibility of power, across both places and spaces:
Visible power: observable decision-making, governed by ‘formal rules, structures, authorities, institutions and procedures of decision-making’.25
Hidden power refers to the influence that powerful stakeholders or institutions maintain, which can be exercised by controlling how priorities are set on an agenda, as well as by limiting participation in available decision-spaces.25
Invisible power shapes ‘the psychological and ideological boundaries of participation’, using its power to shape how individuals conceptualise their place and entitlements in the world, including the acceptance of the status quo and perpetuation of exclusion and/or inequality.25
Within and across every power cube dimension, Gaventa emphasises that spaces, places and forms of power do not exist on their own, but are in a constantly changing relationship with one another; therefore, decision-making spaces are not fixed, but may constantly be shifting, opening or closing through broader system transformation.25
For this article, transcripts from both rounds of national-level and case study interviews were re-analysed guided by the power cube framework and using a framework analysis (familiarisation, identifying a thematic framework, indexing, charting, mapping and interpretation).27 Atlas.ti 8 and Excel were used to assist with the analysis. LP and DCR developed a data extraction matrix in the familiarisation stage, based around the dimensions of the power cube framework. The dimensions of the power cube framework were slightly adapted and mapped on the X-axis of an excel sheet, while the summaries for Uganda and Kenya were plotted vertically, to allow for cross-country findings and reflections to be summarised and compared as appropriate. To better understand actor dynamics around GP, we undertook a broad stakeholder mapping to contextualise the various arenas in which actors exert (or not) their power. While LP and DCR led this analysis, all other coauthor partners reviewed and provided inputs into the results and contributed to the review and refinement of the ‘Discussion’ section, to ensure accurate contextual interpretation.
Any references and quotations provided below are tagged by country and interview number.
In the analysis presented in this article, we strove to maintain the same respect to ethical principles as for the larger study, with a particular focus on protecting the confidentiality of respondents, with care as to not disclosing any information that could unveil the identity of our respondents or raise any professional or personal risks to them.
As our partnership involves an international partnership, an author reflexivity statement was developed using guidance on promoting equitable authorship in publications28 29 and can be found in the online supplemental appendix.
Supplemental material
Results
Our results begin by setting the stage around the actors within which power rests in order to provide the context for the subsequent description of Gaventa’s power dimensions (ie, levels at which power is exerted, decision-making spaces and forms of power).
Actors
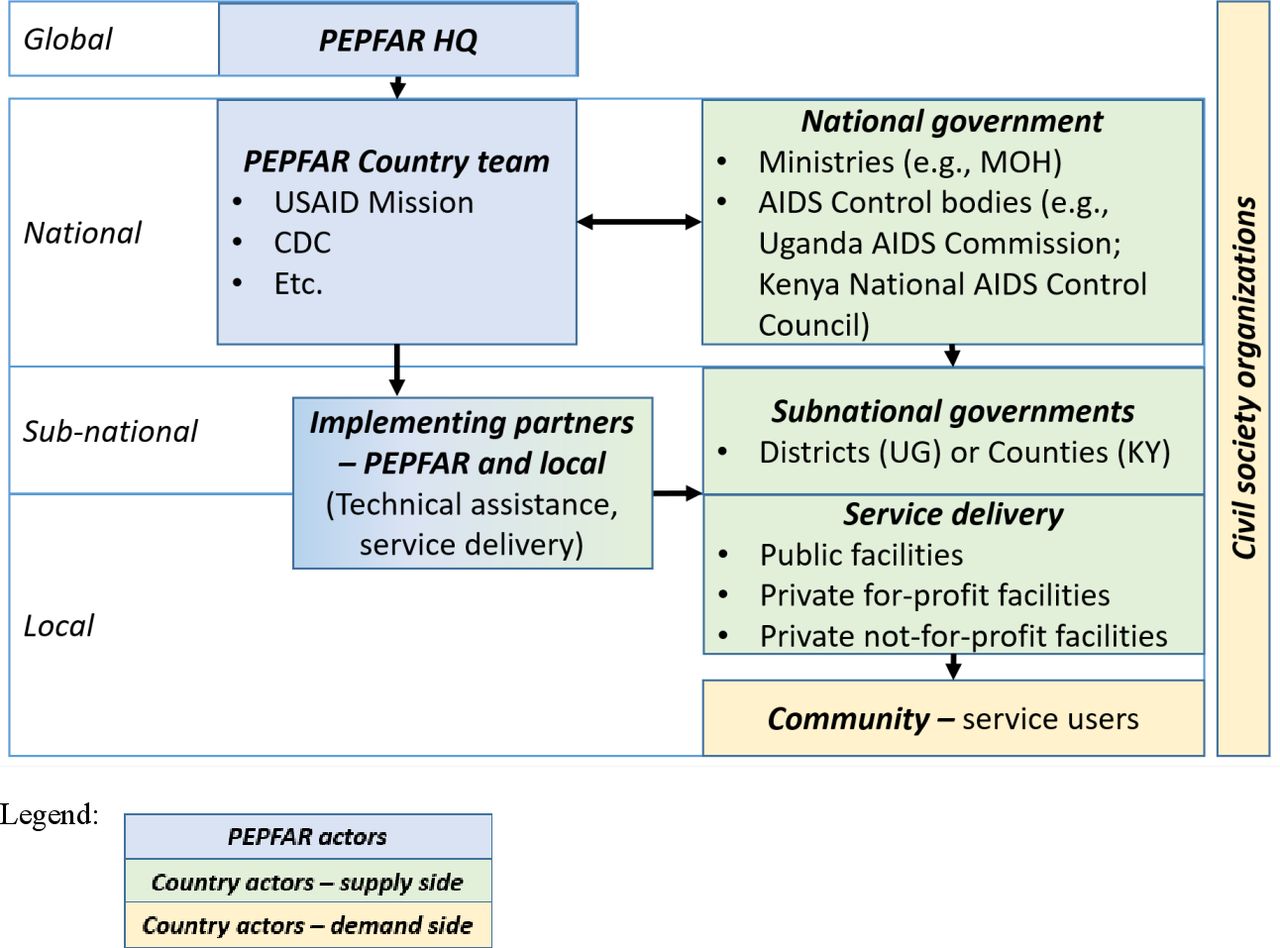
Power rests with two main sets of actors—those within PEPFAR and those within the national bureaucracy. Figure 1 summarises the key actors with their location in the global to local hierarchy. Some actors, such as IPs, interface with country actors across levels, both formally and informally.
{kind=link}
Stakeholders relevant to PEPFAR’s geographic prioritisation in UG and KY, across levels of governance. CDC, Centers for Disease Control and Prevention; HQ, headquarters; KY, Kenya; MOH, Ministry of Health; PEPFAR, United States President’s Emergency Plan for AIDS Relief; UG, Uganda.
At the global level, key stakeholders are PEPFAR HQ leaders, who spearhead global policies and strategies, such as GP. Although they may be influenced by other global health initiatives, HQ leaders often issue global policies without engaging in collaborative decision-making with country-based counterparts, whether national government or cross-agency PEPFAR country teams. PEPFAR IPs, which are largely national and international service delivery NGOs, operate at subnational level offering technical assistance to local governments and health facilities. While IPs are under PEPFAR contracts, they might simultaneously work with government or other stakeholders, straddling the space between PEPFAR and country stakeholders. PEPFAR country teams liaise between PEPFAR HQ and national government agencies as well as IPs, while IPs liaise between country teams and subnational actors. PEPFAR does not have actors representing it at the local level, although it often funds local CSOs who can mobilise community members—mostly for service delivery other than policy consultations.
Country actors operate from the national level and below. For the GP, national-level actors included national government agencies, such as the Ministry of Health (MOH) as well as dedicated HIV agencies such as the Kenya National AIDS and STI Control Programme (NASCOP) and AIDS cross-sectoral coordination bodies (eg, Uganda AIDS Commission, Kenya National AIDS Control Council (NACC)). National government actors both oversee and provide strategic direction to subnational governments (eg, district and county governments), who in turn manage and provide oversight to service delivery across public, private not-for-profit and private for-profit health sector organisations. The local actors map to the service providers, citizens, communities, service users illustrated by Gaventa.25 In addition, especially in the HIV/AIDS realm, CSOs are present at all levels of the system from communities to the national level.
Levels of power
Global
The stimulus for the Kenya’s and Uganda’s GP came directly from the global level, as the Office of the Global AIDS Coordinator and Health Diplomacy (OGAC) issued a directive via its 2015 Country Operational Planning (COP) guidance for all PEPFAR country teams to identify ways in which PEPFAR investments could be more efficient and sustainable, in light of flatlined financial resources since Financial Year 2014.14 30 OGAC developed thresholds for SNU transition, primarily focusing on low testing volume, and used data to construct the GP narrative at the global and national levels.
Country counterparts were not included in any of the global-level policy discussions (U-D12, K-D10, K-D4), and one Kenyan respondent went so far as to suggest that OGAC did not check internally with its own country teams before issuing policy changes (K-D26). Individuals within the USAID Kenya office disagreed with the GP policy when it was announced (K-D4, K-D26).
There was a fair bit of dissidence across the whole US government in doing this [GP]… because at the same time you had a big push on the PMTCT [prevention of mother to child transmission of HIV/AIDS] side for virtual elimination [of] pediatric infections […] it felt like whiplash to a lot of people, to come into all of these communities, to express the intent as to what we were doing […] and to step back…[…] I think it is probably fair to say that we were not as clear in our directions to the IPs as we could have been as people weren’t really on board with the approach. (K-D4 USG)
A couple of USAID Uganda respondents described how the PEPFAR country team negotiated with OGAC to Uganda to allow for significantly longer timelines and IP’s ability to provide regional support (ie, ‘above-site support’), including to CS districts identified for transition (U-D15, U-D21). One of them noted specifically:
[…] from the side of the headquarters […] you don’t give instructions to a country to do a 360 turnover in a defined period of time. So the good thing is that we went firm with our negotiations, and we went firm with our adaptation and I think that’s a positive thing that OGAC accepted our adapting of the strict guidelines to actually accommodate our clustering approach and I think Uganda was […] the first country to modify the instructions. (U-D21 USG)
While we did not have an opportunity to triangulate these findings at the global level, they highlight that in certain instances PEPFAR country teams challenged global policy-making, although this decision-making space was closed to other local actors.
National
At the national and subnational levels, communication provides an important link to how power can manifest. Gaventa illustrates that ‘those who are powerful are not those who “hold” power but those who are able to enrol, convince and enlist others into associations on terms which allow these initial actors to “represent” all the others’.17 Patterns in communication and actors associations, therefore, provide insight into how legitimacy forms across different levels of engagement and into the nature of transition decision-making.26
In Uganda, how the GP was communicated between national PEPFAR actors, such as USAID, and their Government of Uganda (GoU) counterparts was unclear. Our respondents described meetings held during COP consultations and GoU being informed of the GP policy (U-D21, U-D23). However, GoU respondents had very little awareness of the GP (U-D3, U-D8, U-D12, U-D14) and those that were aware acknowledged the GP as a new PEPFAR policy but were unaware of its implementation (U-D12). A Transition Technical Group—including both government and PEPFAR actors was initially proposed, but not operationalised due to the belief that the GP would not have a significant impact on health facilities (U-D12).
Initially we thought we were going to [play a direct role in the GP implementation] because when it was first presented—before the matter was finalized—we felt that this was going to be a major seismic shift and our plan was to come up with a task team that would go out, plan with the district, plan within the ministry on how to respond to the transitions. But it was realized that the impact was unlikely to be that big anyway. So we didn’t have such an active involvement or active role. (U-D12 GoU)
Our evaluation could not confirm the specifics around the data used for this decision and who was involved from GoU or PEPFAR, partly because our respondents reported low awareness of GP decision-making.
By contrast, in Kenya there was widespread awareness of GP. Respondents from USAID, CSOs and Government of Kenya (GoK) indicated that PEPFAR informed key government counterparts, such as NACC and NASCOP, directly and experienced rapid pushback from the GoK about the plan (K-D9, K-D35, K-D3, K-D5, K-D4, K-D32). Concerns about the specifics and timeline of the GP led to protracted negotiations, including two high-level visits from the PEPFAR Ambassador, before an agreement was reached.
IPs and the CSOs were informed directly by PEPFAR via their usual engagement with USAID administrators, informational workshops and monthly and ad hoc meetings (U-D10, U-D18, K-D6, K-D8). CSOs were also informed via existing consultation mechanisms like the Global Fund’s Country Coordinating Mechanism, technical working groups and COP consultations (U-D5, K-D2, K-D3, K-D5). Even within these existing fora, actors received top-down communications rather than being involved in GP decision-making.
According to national-level respondents in both countries, national burden of HIV data was used by PEPFAR to justify the GPs, both as a PEPFAR policy as well as the allocations of SNUs and facilities by burden of HIV cases. In Kenya, this was seen through PEPFAR Kenya’s framing of alignment with GoK’s roadmap. Kenya respondents noted the irony that by dropping a considerable part of their portfolio across countries, PEPFAR would have a harder time meeting its ambitious targets, which resulted in a push from OGAC to ensure that country teams continue collecting and reporting data from CS SNUs and facilities even though support to them had stopped (K-D4, K-D28, K-D29).
The one surprise I’d say is [OGAC] changing their tune a bit [about support to CS], but…if I’d thought about it harder, it’s not that surprising because at the end of the day they want to reach their global numbers, right? And when they realize, if you stop reporting on those counties across all the countries, well there’s going to be an impact on the number of people we’re seeing or supporting. So, it may be a bit cynical … (K-D28 Kenya USG)
In Uganda, respondents justified GP based on data showing that facilities transitioned had not gotten much support and had not seen many patients (U-D12, U-D48), yet there were large discrepancies among the data sets used and inconsistent application of the facility volume rules—meaning that some high-volume facilities also ended up being transitioned to CS. Making funding decisions based on static data estimates also risked missing potential hot spots where HIV incidence was changing (U-D5). Furthermore, throughout the GP in Uganda, and more broadly, data quality across several domains is low and data on how much support is received from PEPFAR by the various districts and facilities are not always declared, suggesting that PEPFAR’s country programmes have the power to limit access to data, and its use for health planning at the country level (U-D3).
Subnational and local
Although decision-making was typically top-down, the flow of information from the top to lower levels of the system was rarely smooth. Respondents across categories and countries reported strong and consistent information flows about GP between subnational actors (ie, government officials and health facilities) and IPs, but almost no communication between the MOH and its district/county counterparts (U-D9, U-D12, U-D14, U-D31, U-D26, U-D37, U-D48, K-D6, K-D8, K-D32). In Kenya, the negotiations between PEPFAR and GoK were given as a reason for delayed notifications to counties, who were eventually informed by the IPs. County-level respondents also complained about the fact that negotiations between PEPFAR and GoK did not result in better coordination or identification of replacement support (K-D11, K-D7).
Several government respondents mentioned that unreliable communication patterns led to inconsistent preparations for executing policy change (U-D68, K-D35, K-D65, K-D67, K-D62, K-D7), with facilities feeling that GP was ‘happening to them, not something they are a part of’ (K-D7).
There was confusion because PEPFAR and National government knew that the only partner on the ground who was supporting HIV was [PEPFAR IP]. This, we never anticipated as a County, that they would be exiting so early…We were not informed prior. We got the information, within six months, that [PEPFAR IP] was transiting and the service should be taken over by the Ministry. So, it was kind of a shock because they left a gap. (K-D67 county government)
In Uganda, we did not have information from local respondents about GP decision-making, however national-level respondents suggested that communication to lower levels had not been consistent. Partly this was the case due to gaps in taking responsibility for such an action—PEPFAR believed communications would come through the Ministry, but in practice this gap was filled in by IPs. However, in Kenya data suggest that while county officials were aware of GP in advance, health facilities were inconsistently informed, and patients were not informed at all.
Given the recent devolution in Kenya that subnational actors were not actively engaged in negotiating GP is noteworthy. Some respondents indicated that counties were not yet ‘fully operational’ at that time and there was a common perception among county stakeholders that HIV was a national programme (ie, not devolved) (K-D8, K-D35). However, not engaging counties meant excluding their perspective (K-D6), and one county official was clear that county political leaders should have been engaged since local governments would be responsible for covering any gaps in service delivery (K-D94).
Decision-making spaces where power is exerted
Closed
The spaces in which actors decided on the GP policy were not open to country actors. One of the Ugandan IP respondents reflected that the process of planning for the GP was more exclusionary than other processes, such as rolling out new MOH guidelines, which are subject to a series of broad consultations (U-D9).
In Kenya, the space where it was decided to move forward with GP was completely internal to PEPFAR and closed to country stakeholders (K-D4, K-D1). Although the space did broaden to include national GoK officials during negotiations on the details of GP, it remained closed to subnational and non-government stakeholders (K-D9, K-D35, K-D10, K-D4, K-D6). As one government respondent stated, bilateral discussions are not open to all and citizens ‘get to know about it later’ (K-D9 GoK). Meanwhile, GP implementation was left entirely in the hands of the IPs.
I would say when the geographical prioritization was brought on, it was more actually a donor driven agenda. It was not widely shared with the National and County Government. […] it would have been nice if the County Government, national government had been […] even at an inception stage and planning to rationalize the resources around geographical prioritization. (K-D36 IP)
The exclusion of the subnational government in Kenya also reflected a perception among national stakeholders that GP would not result in many tangible changes at county and facility level (K-D1, K-D4) so the need to involve subnational actors was minimal.
Excessive complexity in a policy agenda is another way to exclude people from the policy space—policy spaces close if the policy agenda is so complex that it cannot be understood by all. In Uganda, GP took place during a time of rapid change on both the government and donor side, with multiple and overlapping policy changes making it difficult to follow the development of discreet policies, and who was driving which changes. For example, the MOH was rolling out test-and-treat policies in addition to six to seven additional guidelines changes. In addition to the GP, PEPFAR was also implementing ‘rationalisation’ (ie, streamlining of projects and IPs to facilitate local coordination), as well as a push for integrated programming. Each of these policies had overlapping purposes and stakeholders. Further IPs often had more than one source of funding and multiple programmatic priorities. Overall, this complexity would have made for civil society groups or others concerned by the GP to engage in the policy dialogue (U-D37, U-D64, U-D21, U-D10, U-D17, U-D18).
Policies keep changing, guidelines keep changing and new ones come on board…So now if such a thing happens we are left out. When they say the guidelines have changed, the HIV treatment guidelines have changed, the partners are supporting the district to roll out the new ones, we are not supported you see…there were trainings in the districts and then in the health facilities within the districts. We did not benefit. The ministry did not come in as a ministry to give us support but also the implementing partner […] they were not supporting us […] we kept on losing. (U-D64 District)
Invited
As part of its yearly COP preparation and review, PEPFAR conducts invited stakeholder consultations including with CSOs. Several respondents in both countries, including NGOs and CSOs, confirmed that COP review meetings provided the principal means for PEPFAR to inform stakeholders about the GP and gain buy-in (U-D4, U-D7, U-D12, U-D14, U-D21, K-D5, K-D10, K-D26, K-D32). COP review meetings intend to provide a platform for joint planning and discussions between PEPFAR, including their IPs, country governments and civil society. Our respondents confirmed that some of them were involved in the COP process, as well as some prior discussions with CSOs and presentations of OGAC’s strategic directions. However, our data overall indicate that, in the context of PEPFAR’s GP, these invited spaces were used by PEPFAR for information sharing to country governments, CSOs and IPs, rather than for decision-making or negotiations, as noted below.
I took part in some of the consultations […] initially it involved a presentation of the strategic direction that would finally lead to that and these were coming from I think OGAC and then the PEPFAR team would go and sit and work out the data and then present some of their findings. I would be involved in some of the meetings where these findings are presented. We would discuss them. Occasionally they share this in writing […] But as part of the PEPFAR COP process they always consult us. (U-D12 GoU)
Through the preparation for that COP 2015 yes, USAID did inform us of the strategic direction that they were undertaking in terms of how to support interventions in Uganda as a country and therefore they said yes there are districts that we are going to transition, there are districts that we are going to maintain and these that we are going to scale up according to the disease burden…We were taken though a workshop whereby all the implementing partners were informed by it and later on the individual [IP] level where this information was passed onto us. (U-D14 IP)
I think there are two levels of consultations. One the one is where the civil society they had the prior discussions and I think it’s believe the practice prior discussions, having received the communication of PEPFAR: this is where we want to go. Then there been some prior discussions on [the GP]on where, what, where such should be communicated to PEPFAR […] PEPFAR will meet the civil society, presenting their vision and then discussing their vision. And the…where do we want to go as a country and that’s happened its COP2016…2015 then COP2016. (U-D4 CSO)
At the central level the PEPFAR team that we’re working with on this had consultations with the MOH. We informed the MOH, showed them the criteria. We had a couple of meetings with them where we took them through the criteria justification and all and then that was approved […]. Then when we had the review and approval of all this by August [2016] during the in-country [COP] review process and it was approved, our methodology as well as our new approach, additional approach of clustering. We then, once that was approved we then came and informed partners and that was then cascaded down to district. Each district was informed and a plan was made about how to cut this one out. [Districts were] informed by the partner because as you know we have one 112 districts. (U-21 USG)
There wasn’t a strategy document, [GP planning] was kicked off with a cable from OGAC in Washington [in October 2015] that led us to do a quick analyses to look at what we were doing in those counties… just putting together spreadsheets and presentations and those presentations were the ones that were used to initiate the dialogue with the government but there was never a strategy document … because it was started as more of an edict that we shall be out by December 31, that was sort of the marching orders. (K-D4 Kenya USG)
Once the decisions were made and the COP was approved, we came back and the government had to be informed. There are various levels of information. There was a top level government organs which were informed by our front office that there were those changes…On the technical level we were involved. We had various meetings with our colleagues in government at various levels. (K-D32 Kenya USG)
To be honest with you the PEPFAR reprogramming [GP] was such a difficult time and even some people never used to speak to each other because the manner in which it happened found the country not prepared to take up the changes because what we wanted was to make sure that services were not interrupted. So from the Boardroom discussion that we were having we never knew that one day we’ll just wake up and we are told, ‘okay pup, here we go’. No more support to this and, this county and that. And remember even initially the HIV commodity support was going to be affected so it was only Kenya pushing back and saying, ‘as partners in the HIV response we are going to put all the money in one basket to make sure that at least a commodity support is not affected’…of course as government, as NASCOP and NACC I think we have more difficult questions to answer when we go to North Eastern counties like Wajir and Mandera. Why the support that we used to be there is no longer there and people are still in denial that probably it will come back. (K-D35 GoK)
Over time, the transparency of this process has improved, as was noted by several respondents (U-D4, K-D3). One even noted that the GP process may have prompted better engagement strategies:
Whether you can attribute it to the geographical prioritization strategy or not, I think that the elevated conversations that we’ve had and the way we have changed how we work with civil society and woken up to ‘perhaps we need to have a better communications strategy with all of our partners’ has helped that conversation and brought people together. (K-D4 Kenya USG)
In parallel to COP planning, the Ugandan MOH and districts consult with one another about the development of national strategic health plans, and their associated mid-term reviews (U-D37). However, no joint planning about the implementation of the GP was reported within the government hierarchy, nor across PEPFAR and Ugandan counterparts at the national level. In our interviews, CSOs in Kenya questioned GP as an equity issue and argued the process should be gradual because the counties designated for CS had been historically underinvested, face considerable HIV stigma and communities were hard to reach (K-D3, K-D4, K-D5, K-D6, K-D8, K-D35). The equity concerns were discussed in Uganda as well, although not through the interviews, only as part of the stakeholder consultation held to share findings to stakeholders. At the consultation meeting, various stakeholders talked about GP as a taboo topic due to the inequality argument—similar to Kenya, transitioned or CS districts were those which had experienced historical underinvestment, such as the Karamoja region.
Claimed/Created
Our Uganda respondents did not identify specific examples of claimed or created spaces, relative to the GP policy negotiations, except perhaps negotiations mentioned in the section above on the global level of power. These negotiations were led by the PEPFAR country team with OGAC to allow for significantly longer timelines and IP’s ability to provide regional support (ie, ‘above-site support’), including to CS districts identified for transition (U-D15, U-D21).
GoK’s pushback and demands resulting in changes to GP particulars is a form of claimed space in the rollout of GP. GoK garnered concessions around four key areas—extended timeline for GP, shift from facility-based to county-based GP allocations, retention of services for orphans and vulnerable children for a longer period and package of above-site support for counties—after difficult negotiations (K-D35), which seem unlikely that PEPFAR would have agreed to without pressure (K-D4).
In addition, Kenyan respondents described claimed spaces within country networks that influenced how GP was implemented. CSOs in Kenya view part of their role as to ensure accountability from the MOH around HIV, including ensuring continuity of services and assured availability of ARVs. As one CSO respondent indicated, the MOH tries to ensure availability of ARVs but not necessarily the accompanying package of services (K-D24). During GP negotiations, GoK worked to ensure the reliability of commodity supplies (K-D35) but other ancillary services were lost, as reported elsewhere.18 Likewise, over time, counties have evolved as powerful entities as devolution has been formalised resulting in demands for inclusion in what had historically been bilateral negotiations held at the national level, like applications for Global Fund support (K-D27), however at the time of the GP this remained in the realm of potential rather than an actual power. Respondents in Kenya, also raised the value of written documentation to formalise agreements or plans between stakeholders. Government and CSO respondents raised this point in different ways. CSOs noted that written agreements, such as the earlier PEPFAR Partnership Frameworks or even Global Fund’s Co-Financing policy, provide a foundation for civil society to demand accountability from governments for promised support (K-D5, K-D24). In contrast, a government respondent noted that PEPFAR’s announcement of GP via meetings was not actionable. Rather, a formal written announcement could have facilitated an earlier GoK response: ‘Treasury does not act on meeting notes’ (K-D14).
Forms of power
Visible
From the country governments’ perspective, PEPFAR exercised visible power throughout the GP process. For example, although the criteria for selecting SNUs and sites for transition from PEPFAR funding were transparent, they were also developed at the global level without specific regard to local suspected HIV/AIDS hot spots, changing migration patterns or new infrastructure projects and beneficiaries of current support (U-D5, U-D8, K-D32).
An emergent form of visible power during this period was USG’s publicly announced suspension of support to the Kenyan MOH in May 2017, due to corruption concerns.31 In practice, this meant that USG funds could not be used to support national-level entities, such as NASCOP, but support to counties or patient services could continue. This loss of support 8 months after GP affected NASCOP’s ability to provide technical assistance and capacity building to counties (K-D35) and resulted in a “period of instability of how we all work together” (K-D10 CSO).
Hidden
Our data suggest that dynamics within the country hierarchy play out as forms of hidden power. For example, Uganda respondents suggested that the MOH, among other government agencies, might have some leverage through their inaction—that is, not shifting their priorities in response to donor policies, such as the GP, without first monitoring how other donors react and contribute resources (U-D5, U-D10, U-D18).
I think the Ministry just quietly doesn’t do it because they know they can’t…And PEPFAR says ‘you have to take the lead, it’s your time to step up’ and the Ministry just quietly does nothing, they can’t…So their attitude is ‘this is your programme’ quietly, they don’t say it bluntly, so they just kind of passively don’t do anything. Just for self-protection really. (U-D18 IP)
In Kenya, one civil society respondent highlighted the national government’s tendency to invoke devolution when there were problems but exclude counties when convenient (eg, negotiating financing with donors), thus using GoK’s hidden power to retain negotiating primacy.
The challenge is for the National Government because when there are problems they come up to say health is a devolved function and it should be followed-up by county Government…But when they get resources like from PEPFAR and Global Fund or when they have money in treasury for health management equipment scheme or when they have loans, they manage it without reference to the county government…partners like USAID…their concern for risk and corruption…they don’t deal directly with the counties because I think some of it is also from intimidation from the national level. I think the national level is strong and want you to be dealing with them directly. That is the same arrangement with Global Fund, blame county but as long as it is signed at a national level the resources are at national treasury, there is no mechanism of ensuring that everybody gets its fair share. (K-D24 CSO)
In both countries, respondents raised concerns about how prioritising efforts geographically resulted in de-emphasising SNUs that were already underinvested, including rural areas, leading to further exclusion, while simultaneously ramping up efforts in areas that are overwhelmed by development partner presence (D8, D-33, D64, K-D5, K-D6, K-D10, K-D24).
When they [PEPFAR] chose to go where they chose to go, we also discovered there are many other partners…concentrated in the same area and other parts of the country were allowed to suffer. (K-D10 CSO)
Specific to GP implementation, we identified a couple of examples where PEPFAR’s dominant rules and procedures, in the absence of spaces to challenge them, resulted in PEPFAR exercising hidden power when it came to the promised above-site support. First, PEPFAR HQ provided guidance to country teams on what types of support SNUs could receive at any given time, but the existence of this guidance effectively created barriers for country teams to provide input on the support that was actually needed. Second, hidden power was exercised by PEPFAR country teams pressuring IPs to meet targets in non-CS areas thus re-orienting attention and resources away from CS (K-D8, K-D28, K-D32).
Invisible
Although challenging to identify, we believe that the GP case illustrates two incidences of the exercise of invisible power. First, in Kenya a CSO respondent described how GoK was reluctant to acknowledge the role of donor funding and support. Instead, the government sought to establish beliefs within the population that health services come primarily from government. This proves problematic when donors exit because communities’ and local stakeholders’ understanding of the situation creates confusion and means that local actors do not know who to hold accountable for the changes they are experiencing. Perversely, the government is exercising a form of invisible power that may damage its own reputation.
Government is reluctant to share openly with their counties that partners are leaving because…whether it is USAID [funding], whether it is Global Fund, the Government and Ministry of Health constantly communicates that they are providing services free of charge…So when a partner is getting out of for example county or a facility, the Government does not want to come back and say that ‘you see the USAID was supporting this and now they are getting out’, simply because in the initial communication they did not say USAID or PEPFAR, they say ‘we [MOH] are providing this’. So when the partner is now withdrawing then they find it difficult to come and expose themselves and say ‘the partner who was supporting us here now is leaving’. (K-D24 CSO)
Second, returning to initial decision-making around the GP, it is notable that while the GoK sought to challenge PEFPAR’s decision-making process, the GoU did not seek to do so. While this may be explained in part by the perception of some GoU respondents that the GP would have limited impact on the Ugandan districts and sites where services were withdrawn, it might also speak to the invisible power of PEPFAR in making such a decision without engaging local counterparts in a meaningful way.
Discussion
While this is not the first study to shed light on the political and sometimes difficult nature of donor transitions, ours is the first formal application of Gaventa’s power cube framework to analyse this topic. Our application of the power cube framework illuminates the different levels, spaces and forms through which political influence came into play for PEPFAR’s GP in Kenya and Uganda. We found that the GP was designed with little space for local actors to shape either the policy or its implementation, despite its significant implications for governments and subnational actors. At the time of our study, invited spaces, such as COP-related meetings, did not serve as platforms for joint decision-making and negotiations related specifically to the GP policy. While decision-making processes limited the scope for national-level government actors to shape the GP, the GoK claimed such a space, proactively pressuring PEPFAR to change particular aspects of its policy. Subnational-level actors by contrast were typically recipients of top-down decision-making with apparently limited scope to resist or change things. While CSOs, in principle, had an opportunity to hold both PEPFAR and government actors to account, in practice the closed-door nature of policy-making and the lack of transparency about decisions made it difficult for them to effect this role. Seeking accountability is complicated by the power funding agencies like PEPFAR have on the CSOs.
To some extent, our analysis confirmed that funding agencies hold significant power in the decisions on whether to transition their programmes and when. However, important power asymmetries existed also within PEPFAR, as displayed in the interactions between HQ, country PEPFAR teams and PEPFAR IPs. The attention to different levels of action aided by the power cube framework helped to tease out the nuances of these interactions in Uganda—where our data recorded less formal pushback to the GP policy—and in Kenya—where our data recorded important and public discord around the GP policy. These changes happened with the backdrop of a history of unbalanced power dynamics, which span well beyond the GP.
They also occur in the context of changes in the relationship between national, subnational and local government units, which in both Kenya and Uganda had formalised power sharing through devolution and decentralisation, respectively. Subnational or local government actors can and should play a role in transition decision-making, but they are often excluded from communications about transition policy by national-level actors. In both countries, the presence of distinct donor and national stakeholders, operating at times in parallel, underscore the potential disconnect between global decision-makers and national governments, and between donor programmes and local counterparts across levels. IPs contracted by PEPFAR straddle these two spheres and played an important role in the implementation of the GP.
The power cube spaces revealed insights into how the network of diverse actors interacted with one another in each country context. Our analysis highlighted missed opportunities in creating spaces for meaningful consultation and coordination—such as the decision to drop the Transition Technical Working Group discussed in Uganda. Our respondents’ reflection that COP planning is a PEPFAR space, not a government one, is important and raises questions about funders’ responsibilities to create more inclusive planning processes that may require yielding some of their power. Our analysis also shed light on the potential held by IPs and local CSOs to create spaces in which to engage. In both countries, our analysis highlighted ‘spaces avoided’ for policy discussion—at the time of our data collection, it did not seem like Technical Working Groups, Health Policy Advisory Committees, Country Coordination Mechanisms, etc were leveraged for GP or COP-related decision-making.
Finally, our analysis of forms of power highlights how large donor initiatives, such as PEPFAR, often create incentives to prioritise internal accountability structures for the donor rather than external accountability to local stakeholders. This can have severe repercussions, as seen from the pushback in Kenya. HIV service data were important in these relationships and negotiations, although the power cube does not directly reflect on the role of data, which has relevance across power cube levels, spaces and forms. In the push for evidence-informed decision-making, the neutrality of data and evidence are often implied but analyses like ours show how data can be deployed in support of predetermined policy decisions.
Overall, we found that the GP was designed with little flexibility for local actors despite its significant implications for national and subnational actors, and revealed how policies and data can be used to reinforce power imbalances. Our power analysis highlights several factors regarding power dynamics between development partners and country counterparts as well as for within-country governance beyond donor transition.
We also contribute to the growing literature arguing for best practices in donor transitions around (i) ensuring better alignment of policies and their implementation with the local country context, (ii) promoting power sharing during transition planning between donors and national actors (across all government levels) around how to best ensure continuity of service delivery post-transition and (iii) understanding the effects on policy and programmes of policy shifts, such as reversing transition policies.7 11 15 23 32–34 The GP experience highlights the importance of putting local actors in the primary decision-making role for transition planning and implementation and ensuring a fairer balance of power between donors and national governments.
As the power analysis was not the main objective of our data collection, our analysis has several limitations. Due to the nature of the parent study, our team was not able to conduct further interviews to follow-up on issues of power or to probe more deeply into some of the power cube dimensions that were not full represented in our data, such as invisible forms of power. As policy processes and deliberations are complex and multifaceted, it is possible that our data might have missed out on additional hidden spaces for decision-making. We did not have access to budgetary information to determine trends in PEPFAR investments by SNU type, over time. Among available interviews, only a few were conducted with CSOs, leading to an over-representation of IP views. Furthermore, only USAID-supported sites were included in our sample, missing perspectives from other PEPFAR agencies. Given the heterogeneity within PEPFAR, the power dynamics might be different when the GP was implemented through other agencies. However, the sites affected by GP were majority-supported by USAID. Second, the parent study was not timed to observe medium-term or long-term power dynamics. Greater efforts to monitor transition in real-time and to continue medium-term to long-term monitoring would be helpful to support learning from this process. Such analyses could observe whether, when and how GP-like policies may be reversed, whether and how invited spaces become more inclusive and trends in overall investments in HIV programmes from country governments, PEPFAR and other non-USG donors who work in this space.
More broadly, the PEPFAR’s GP policy is unlike Gavi and GFATM transition or graduation policies. Rather than a pre-established policy with clear metrics for transition and a long runway for preparation and implementation, it came about as part of a broader shift within PEPFAR from emergency response towards country ownership and greater sustainability,11 as well as warnings that a too rapid transition to country ownership would be risky.35 The initial premise of the GP policy was to better target PEPFAR resources to regions which needed the investment most while areas where investments were no longer justified according to PEPFAR’s metrics would permanently lose funding thus transitioning from PEPFAR support. In 2013, PEPFAR acknowledged that not all partner countries would be ready to assume greater funding commitments to their national HIV/AIDS programmes.36 After the initial wave of GP implementation, which our project evaluated, PEPFAR continued to refine its prioritisation policies, how they are framed and how they are implemented. Based on the available data, we examined the initial implementation of the GP, roughly between 2015 and 2018. A longitudinal analysis of how GP policies have evolved over time is not within the scope of this paper, but we hope that future research will document it in the future. Nevertheless, our analysis demonstrates the value of conducting a power analysis in the context of donor transition, as well as of adding new dimensions to the original power analysis cube—such as an elaboration of stakeholder hierarchies in the various spaces.
Despite a growing interest in the nature and expression of power in global health, and health policy and systems research in particular,37–39 there have been relatively few applications of the Gaventa power cube to global health issues. Notable exceptions include Baker and Demaio on food systems40 41 ; and McCollum et al on devolution in Kenya. While our original data collection did not aim to conduct a power analysis, we found that the notion of levels of power and spaces in which power was exercised were highly pertinent to our data. It was more challenging to discern the forms of power, perhaps because, by definition, hidden power and invisible power are difficult to interrogate, especially post facto. In addition to the three dimensions that Gaventa identifies, we also found it valuable to explore instruments of power, meaning the different tools or approaches used to exercise power.
Future research and practice should prioritise better governance and accountability models that consider differences between national and subnational actors, incentives, capacities, etc. With increased decentralisation in many contexts, research on development partner practices, including transition, needs to interrogate how global-level entities create the spaces and incentives for national governments to engage more directly in decision-making and to communicate transparently with local governments and civil society. In terms of broader efforts for donor accountability, the role of CSOs in the context of donor/government negotiations should be better documented, considering their current position at the margins of most decision-making spaces, yet their strong potential to advocate for marginalised and vulnerable groups. Longitudinal research on donor transition policies, such as the GP, should be prioritised and focused on capturing how transition and reprioritisation are framed by different stakeholders and over time and how politics and power shape the discourse around transition, especially as long-term impacts are observed.
Conclusions
In the context of increasing awareness of how long-standing power imbalances, particularly between North and South have shaped global health,42 43 transition processes offer a highly relevant case study of how such power differentials persist and what may be done to address them. A better understanding of the power dynamics stemming from donor transition highlights the importance of research and transparency about power dynamics and the value of frameworks such as the power cube for such analyses. Our findings make the case for donors to exercise power responsibly, especially to ensure that the transition can facilitate the transfer of health service mandates to governments or other role bearers. This study clearly highlights the underinvolvement of subnational actors/structures in negotiations, decision-making, communications and planning for implementation. If engaged by national governments, subnational actors as well as CSOs could respond better to changes that arise from transition in negotiations with donors, in support of the country’s national agenda. Greater transparency and accountability would increase the success of global health programme transitions because they support the actors engaged in decision-making around transition—across all levels—to be more aware and flexible of working within political systems that have implications for programmatic success. More deliberate efforts to build local confidence and capacity, as well as sustainable health gains require donors to allow sufficient time for negotiations about transition, and adequate resources for the related change management and planned financial outlays from their national and subnational counterparts.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval for the original data collection was provided by the Johns Hopkins Institutional Review Board (IRB) (IRB #0007208), Amref Kenya IRB (Protocol #325/2017) and the Makerere University IRB (Protocol #481). Local ethical approval was provided by the Uganda National Council of Science and Technology’s Research Ethics Committee (SS 4263). Oral informed consent was obtained for case study respondents and Key Informant Interviews.
Acknowledgments
We would like to acknowledge and thank study participants, especially those individuals living with HIV, who gave generously of their time and experience without which this study would not have been possible. We also recognise the extraordinary effort of the in-country research teams who supported and participated in data collection and analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
LP and DCR are joint first authors.
Handling editor Stephanie M Topp
Contributors This analysis relies on data collected as part of a USAID-supported mixed-methods evaluation of the impact of PEPFAR’s geographic prioritisation (GP) on central support subnational units and health facilities in Kenya and Uganda. This article re-analyses qualitative data to document the process and impacts of implementing the PEPFAR's GP strategy with a particular lens on the power dynamics involved in the process. LP and DCR developed a data extraction matrix in the familiarisation stage, based around the dimensions of the power cube and used it to guide data analysis and synthesis. While LP and DCR led this analysis, all other coauthor partners reviewed and provided inputs into the results and contributed to the review and refinement of the 'Discussion' section, to ensure accurate contextual interpretation. LP and DCR share the responsibility as guarantors for the analyses conducted for this article.
Funding This study was funded by USAID via Project SOAR, managed by Population Council (agreement no. AID-OAA-A-14-00060). USAID and Population Council provided feedback on the design and results of this study but did not influence the research team‘s interpretation of the findings.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
↵By 2020, 90% of all people living with HIV will know their HIV status, 90% of all people with diagnosed HIV infection will receive sustained antiretroviral therapy and 90% of all people receiving antiretroviral therapy will have viral suppression.44