Article Text

Abstract
Since the first administration of COVID-19 vaccine in December 2020, countries have experienced a range of challenges at different phases of their COVID-19 vaccination programmes. Initially, with limited global COVID-19 vaccine supply, the WHO called for vaccine equity to ensure the most vulnerable people in every country globally had access to vaccine, and COVID-19 Vaccines Global Access was established to facilitate equitable access to COVID-19 vaccine. However, the aims of these initiatives were challenged as many countries secured earlier access to COVID-19 vaccine with direct agreements with manufacturers. During the early stages of COVID-19 vaccination programmes, the rate of vaccine uptake was determined by number of COVID-19 vaccines approved for use and the manufacturing capacity of the manufacturers of these vaccines. It is a very different situation in 2022, where COVID-19 vaccination coverage is no longer determined by access to supply and manufacturers are reducing or stopping production of vaccines completely. Uptake of COVID-19 vaccination in 2022 is dependent on complex issues like vaccine hesitancy. This paper focuses on the Central and West Asia region, where the authors have been supporting COVID-19 vaccination programmes across seven countries in this region. In this paper, we outline and describe the different phases of demand for COVID-19 vaccination as well as the risks and strategies to consider in each of these phases.
- Vaccines
- COVID-19
Data availability statement
Data are available in a public, open access repository.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
There have been three distinct demand phases for the COVID-19 vaccine since first administrations in December 2020.
The first phase was defined by high demand and low supply, the second phase as a period of high demand and high supply, and the third phase as a period of high supply and low demand.
Countries need to adopt different strategies across each of these demand phases to ensure effective use and minimal wastage of COVID-19 vaccines.
The extent to which vaccine hesitancy and vaccine nationalism feature in different regions is dependent on the demand phase being experienced.
Introduction
The COVID-19 pandemic is profoundly affecting life across all areas of the globe, including morbidity and mortality from the disease itself, but also through a range of mechanisms designed to restrict the spread of COVID-19. Measures to reduce the transmission of COVID-19 have had a significant impact on all elements of society. Social isolation, local trade and business restrictions, restrictions of conventional workplace practices, border constraints, and restricted access to non-emergency surgical and medical care have been of significant socioeconomic, cultural and mental health detriment throughout the global community.1–4
Before the pandemic, the shortest time to develop a vaccine was 4 years. However, the unprecedented global efforts to market a COVID-19 vaccine resulted in the first vaccine, Pfizer-BioNTech, being approved for emergency use in less than 9 months after the WHO declared COVID-19 a global pandemic on 11 March 2020.5 6 This extremely ambitious timeline was achieved through global coordination of advanced research, provision of sufficient multimodel funding, and remarkable innovations in clinical trial and vaccine manufacturing processes.
Despite the successes of the COVID-19 vaccination effort globally, resulting in 5.16 billion people (67.3% of the global population) receiving at least one dose of vaccine (as of 15 May 2022) in just over 2 years since the pandemic was declared, many challenges persist.7
A key challenge currently in the global vaccine effort is countries with low vaccination rates that have a vast stockpile of vaccines at high risk of wastage at all levels of the supply chain. This issue has been identified with the Serum Institute of India, the largest vaccine manufacturer globally and manufacturer of the Oxford-AstraZeneca vaccine, Covishield, which halted vaccine production in December 2021 on the basis that their vaccine stockpile had grown to 200 million doses, noting that the only 63% of the population in India are fully vaccinated.7 8
Further, many countries have reported being challenged with increased wastage attributable to a decline in ongoing vaccine uptake from what had been anticipated.
There have been three distinct demand phases for COVID-19 vaccination since the first vaccine was administered in December 2020. These are outlined as follows:
The first phase of demand was defined by the low supply of vaccines and high demand for COVID-19 vaccination. During this phase, countries focused on providing access to healthcare workers at high risk of exposure and vulnerable individuals, including older adults.
The second phase of demand was defined by higher supply in the presence of high demand for COVID-19 vaccination. During this phase, countries focused on expanding eligibility to the broader population as quickly as possible.
The third phase of demand is defined by high supply with low demand for COVID-19 vaccination. Many countries are now experiencing this phase, and it is presenting a range of challenges including increased wastage from expiries and cold chain breaches.
With different challenges at each demand phase, stewards of COVID-19 vaccination programmes will need to adopt a range of strategies at each phase to ensure rapid uptake of vaccine within the most appropriate cohorts, minimise the burden of COVID-19 as well as minimise wastage.
While vaccination rates vary between countries, 7-day rolling averages of administrations have decreased from the peak of more than 43 million doses per day to less than 6 million doses per day, and therefore many countries will be approaching or are already in the third demand phase.9 Countries need to ensure they adopt and effectively implement a range of strategies to ensure vaccine demand continues and wastage is minimised until such time global vaccination targets are achieved.
The authors of this paper represent the Vaccine Advisory Firm for Central and West Asia, a project funded by the Asian Development Bank since August 2021 and implemented by Crown Agents in partnership with FHI 360. The project provides technical assistance and advisory support to Kazakhstan, Azerbaijan, Uzbekistan, Tajikistan, Georgia, Armenia and Kyrgyzstan. We propose that all these seven countries in the Central and West Asia region are currently in the third phase of demand, with decreasing vaccination rates across the region.
As shown in figures 1 and 2, the level of vaccination coverage varies between the seven countries in the region, with 19% of the total population fully vaccinated (two doses) in Kyrgyzstan compared with 52% in Tajikistan (as of 14 May 2022).9 Positively, Azerbaijan and Kazakhstan achieved the WHO target of 40% coverage by December 2021, with Tajikistan and Uzbekistan reaching this target before March 2022.9 Unfortunately, none of the seven countries reached the WHO target of 70% coverage by mid-2022.9

Share of population fully vaccinated against COVID-19 as of 14 May 2022.

Trend in the share of population fully vaccinated against COVID-19.
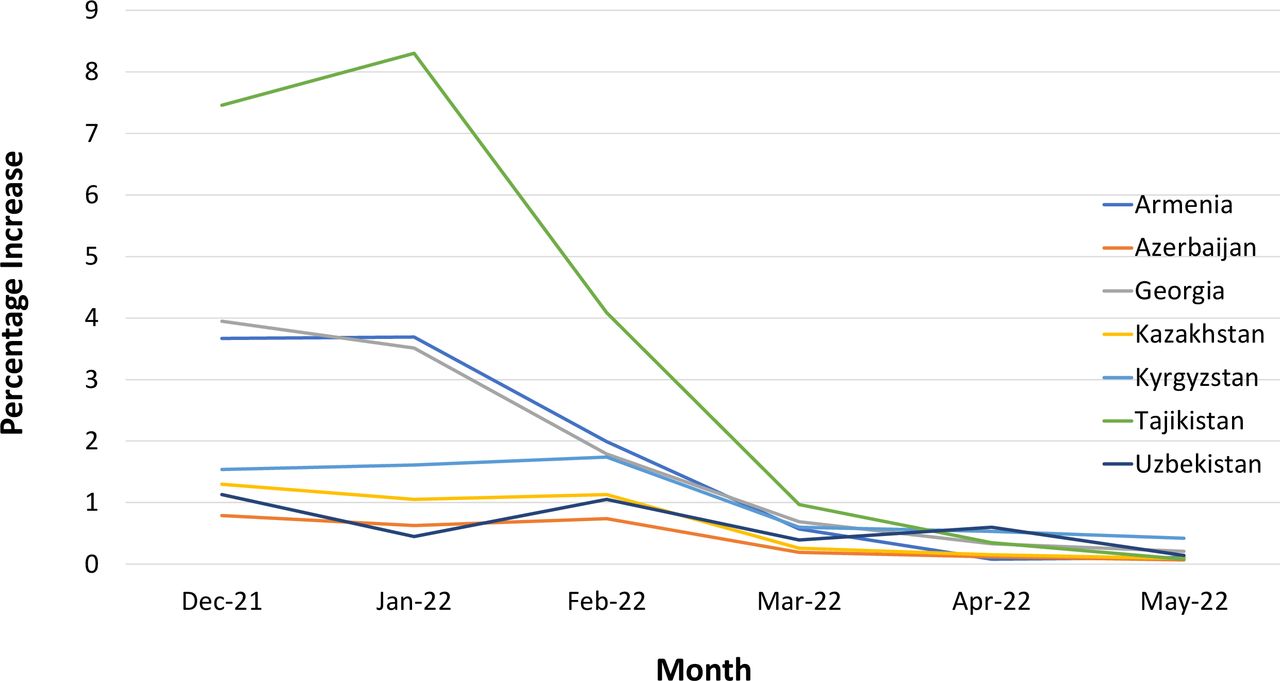
The monthly trend in the percentage of the population across these countries that have received at least one dose of a COVID-19 vaccine is illustrated in figure 3, clearly depicting the slowing pace of vaccine uptake across all seven countries.7
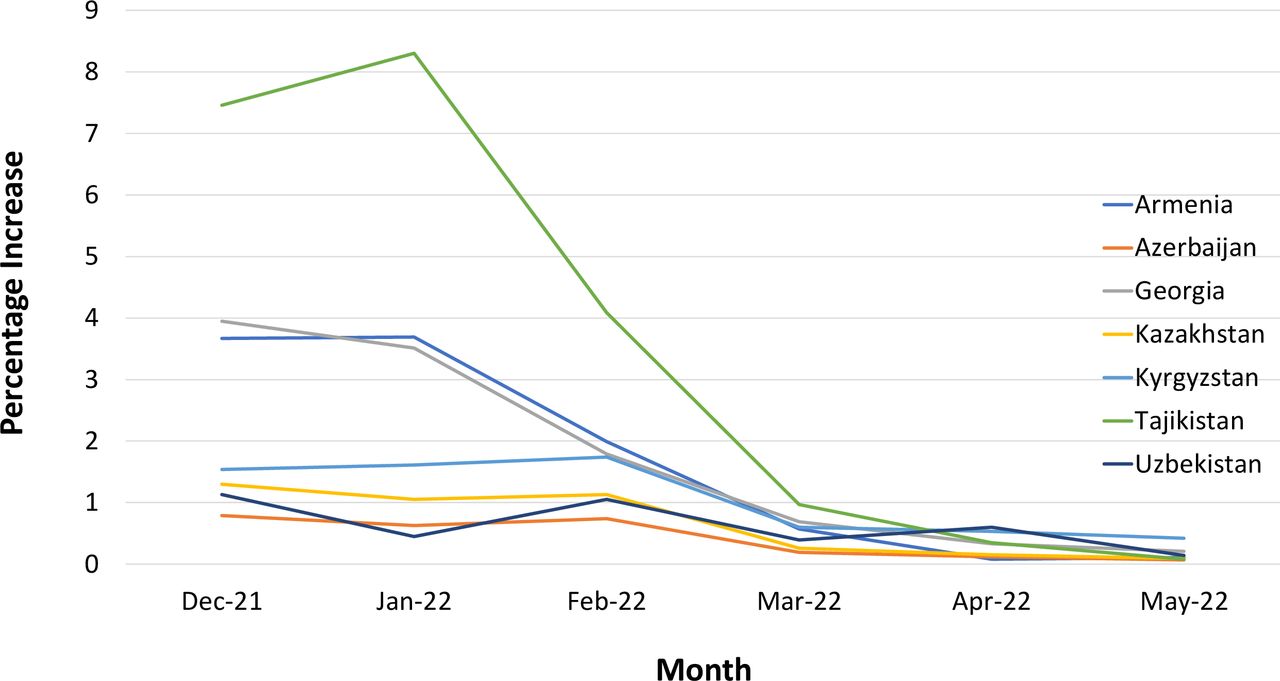
Monthly increase of population that has received at least one dose of COVID-19 vaccine.
In addition to decreasing rates of vaccine uptake, we have summarised the total doses delivered over time for these seven countries in figure 4.10
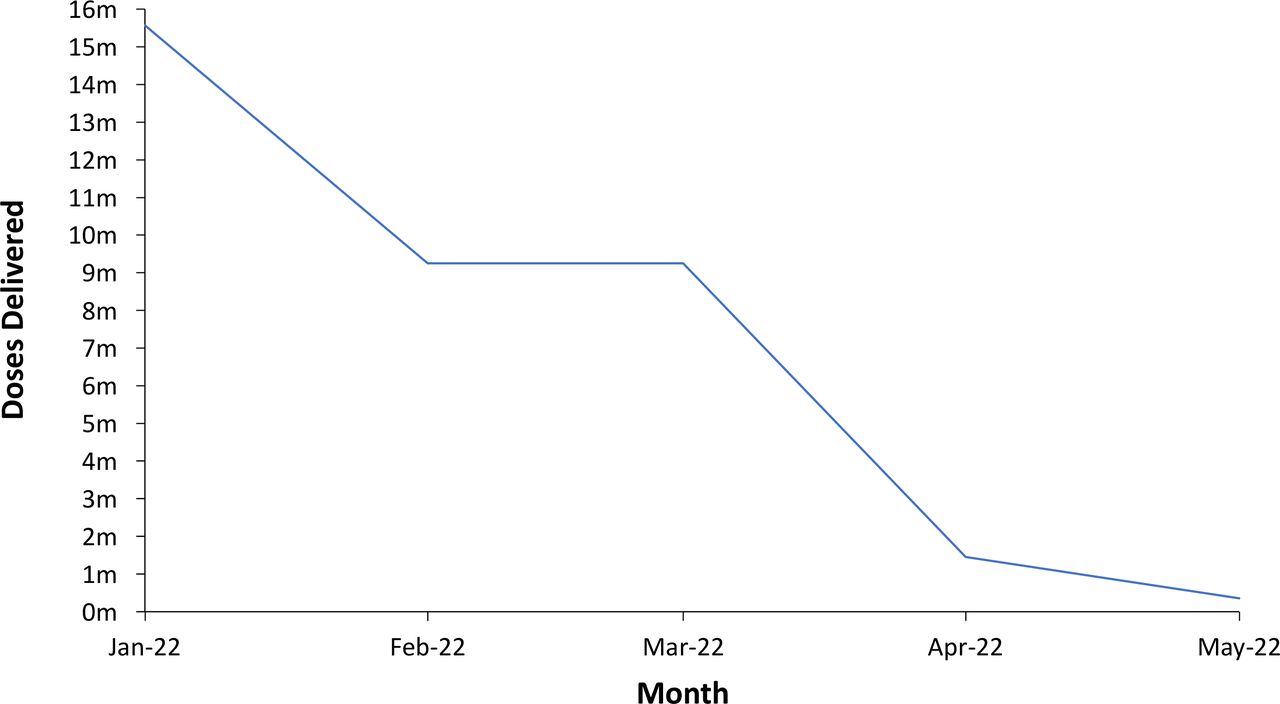
Total COVID-19 vaccine doses delivered across the Central and West Asia region.
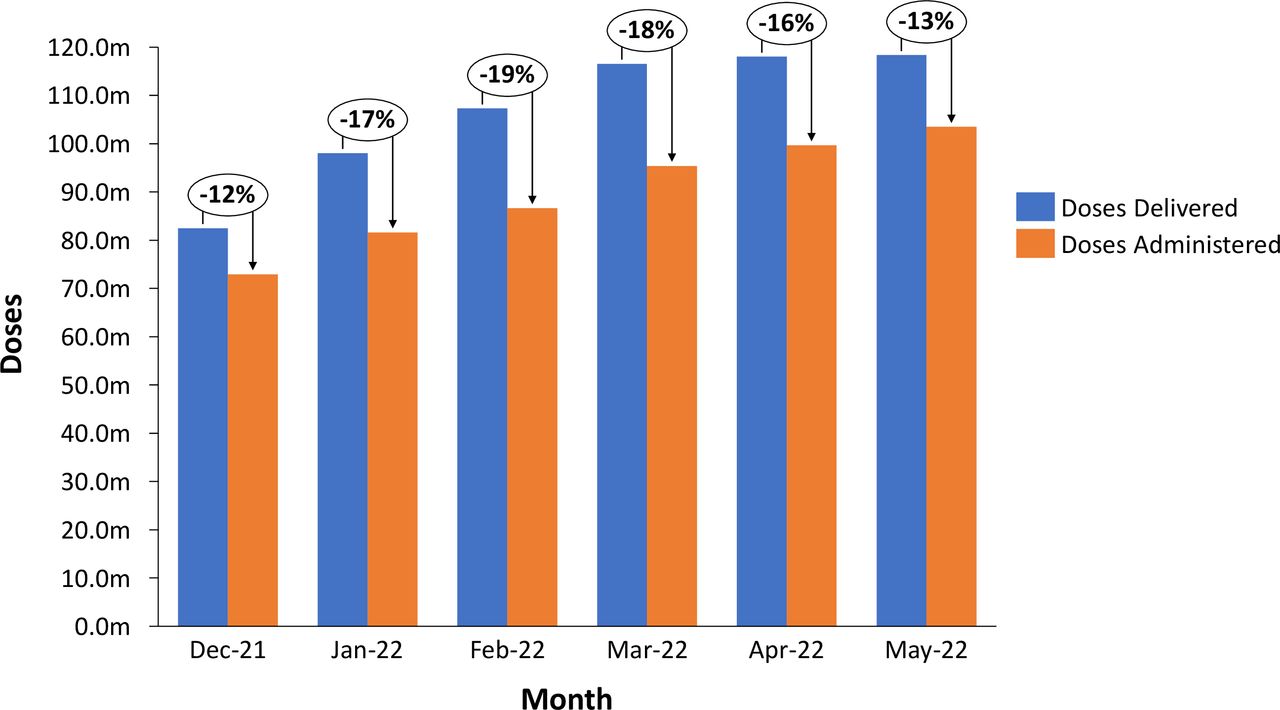
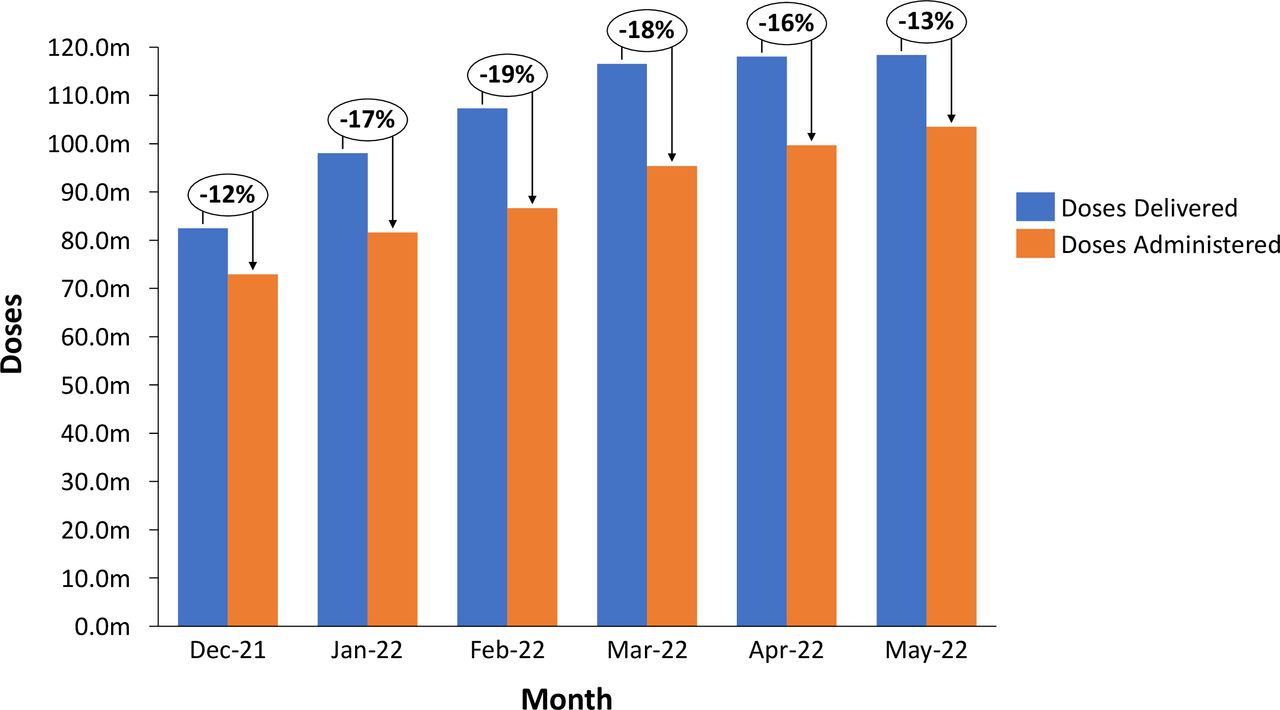
In addition to the vaccination rate analysis and doses delivered, we have analysed excess doses by subtracting the total doses administered from the total doses delivered over time. It is important to note that wastage is not accounted for in the subsequent analysis s this is not consistently reported across countries in the Central and West Asia region. Figure 5 shows excess doses available across the region are consistently decreasing from February 2022, a sign that countries are accurately predicting uptake and scheduling deliveries of vaccines appropriately. Collectively, the figures demonstrate that all seven countries are in the third phase of the COVID-19 vaccination demand.9 10 Although demand for vaccination is decreasing, countries are managing stock on hand by reducing vaccine orders in line with demand.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Analysis of excess COVID-19 doses in the Central and West Asia region.
Vaccine nationalism has been widely discussed during the rollout of COVID-19 vaccines globally, with frequent calls and efforts to ensure that vaccine is distributed based on global need rather than an individual country’s purchasing power. While vaccine nationalism and equity of access have been significant issues during the COVID-19 vaccine rollout, it is also true that this issue is becoming less apparent over time, particularly in the third demand phase, which many countries are experiencing now.11–14
COVID-19 vaccine hesitancy has also been a significant issue that has been widely discussed during the rollout of COVID-19 vaccines. While many countries will attempt to estimate the extent of vaccine hesitancy early in implementation of their COVID-19 vaccination programmes, the extent of vaccine hesitancy is only truly realised during the third demand phase when vaccine supply is high and demand for vaccine plateaus. This is likely occurring in the Central and West Asia region, with recent data suggesting that there are both high rates of COVID-19 vaccine hesitancy and countries without publicly available data on the extent of COVID-19 vaccine hesitancy.15
Suggested responses
Based on the aforementioned information provided, Central and West Asian countries are currently experiencing the third phase of demand for the COVID-19 vaccine defined by high supply and low demand for vaccination. To address the challenges of maintaining demand, increased wastage from expiries and cold chain breaches, 10 suggested responses are provided:
Quantify and develop strategies to address vaccine hesitancy. Regionally, the extent of vaccine hesitancy varies significantly across countries and demographics. While concerns for safety, side effects and effectiveness are commonly identified as causes for hesitancy, local community consultation is necessary to understand the extent of and strategies to address vaccine hesitancy.16–20
Adjust COVID-19 vaccine deliveries to account for extent of vaccine hesitancy. To effectively forecast vaccine requirements, it is essential that countries and COVID-19 vaccine programme administrators continually monitor the extent of vaccine hesitancy in their jurisdiction and set targets that consider the population likely not to accept a COVID-19 vaccination.
Publish COVID-19 vaccination and delivery data. In addition to understanding the extent of vaccine hesitancy, COVID-19 vaccine programme administrators should facilitate frequent and transparent uptake of COVID-19 vaccination data to allow interpretation by all stakeholders including academic and public health organisations. Sharing of COVID-19 vaccination rates will facilitate the early identification of trends in vaccine uptake, changes in the number of excess doses, and identifying the extent and causes of vaccine wastage.
Implement strategies to reduce COVID-19 vaccine wastage. Vaccine wastage can be categorised as either closed-vial or open-vial wastage. Open-vial wastage occurs at the clinic level, where improper storage, handling, reconstitution or administration results in not all doses within a product unit being used. Productive education and practice of key vaccine storage and management principles (‘early expiry first use’), adequate supply of required consumables and mandatory reporting of wastage at a clinic level are key in reducing open-vial wastage. Closed-vial wastage is the result of poor temperature control and monitoring, unsuitable transportation and storage, or stock that is unable to be used by the manufacturer’s expiry. Effective use of vaccine logistics management systems or purpose-built vaccine management platforms such as Real-time Vaccination Monitoring and Analysis assist in minimising wastage; however, accurate forecasting of vaccine demand and subsequent ordering of vaccines with expiry consistent with this volume is the predominant factor in reducing wastage.21–24
Consider manufacturer’s shelf life and stock on hand before placing additional orders. Consideration of the manufacturer’s shelf life and any subsequent expiry restrictions varied on storage conditions is essential in finalising orders for the COVID-19 vaccine, with most COVID-19 vaccines having an initial shelf life of 6–9 months from the manufacturing date. The rationale for making this consideration is to guide the amount of buffer stock that can be held with minimal risk of wastage. Countries should consider historical monthly and subsequent forecasted throughput to ensure that the doses on hand do not exceed months of stock beyond the manufacturer’s shelf life.
Measure cold chain capacity for all relevant temperature ranges and consider when placing additional orders. As demand decreases and COVID-19 vaccine deliveries continue, stock on hand is likely increased and may exceed cold chain capacity. Noting that vaccines have different cold chain requirements (to include long-term storage in ultralow-temperature environments, standard freezer temperatures and standard refrigerator temperatures), capacity should be considered in the mix of vaccines procured and likely maximum value of stock holding in a decreasing demand environment. In addition to cold chain capacity, countries should also place increased importance on the repair and maintenance of cold chain equipment in this phase, as well as strategies to reduce risk in single sites (including backup power and decentralisation of stock holding).25 Detailed planning should be completed by all countries to ensure that sufficient cold chain capacity exists for the COVID-19 vaccine procured across all three phases.
Redistribute COVID-19 vaccines to areas of higher demand. It is very common for uptake of vaccines to vary in neighbouring countries, and therefore it is likely that different locations will enter the third phase of demand and have stock increases at different points in time. Therefore, one strategy that can be deployed domestically is to reverse the logistics of vaccines from health centres to central storage and subsequent redeployment of vaccines to an area of higher demand. In addition, countries could also consider diplomatic channels and regional mechanisms to redeploy vaccines if vaccine stock on hand is increasing in certain areas.
Collaboration with COVID-19 vaccine manufacturers to extend shelf life. An additional consideration to minimise wastage is extending the original shelf life of a vaccine through collaboration with the manufacturer and the national regulatory body. This strategy has been deployed by several countries across different COVID-19 vaccines to temporarily avoid the significant wastage of vaccines. For example, the Food and Drug Administration in the USA, the Therapeutic Goods Administration in Australia and the European Medicines Agency have extended the manufacturer’s shelf life of the Pfizer-BioNTech vaccine by an additional 3 months when stored in an ultralow-temperature environment.26–28
Consider remaining shelf life when accepting donations. Countries should also be cautious when accepting donations from countries that are in the third phase of demand, as there is an increased risk that the doses have a short remaining shelf life. There have been several reports of ‘dumping’ of short-dated COVID-19 vaccines as countries aim to minimise wastage of vaccines in their own countries and increase donations to other countries.
Implement and leverage data from logistics and health information systems. The use of an electronic Logistics management system or purpose-built vaccine management system, as well as integration of health information systems, is recommended to ensure that critical metrics including vaccination rates, wastage and stock on hand are captured and reported at a regular interval with all stakeholders.
The aforementioned recommendations should be considered by countries that are experiencing decreasing demand for COVID-19 vaccination. The analysis to support these recommendations has been made during an evolving pandemic that requires countries to adapt their vaccination programmes to respond to the appearance of new variants and new evidence that supports expansion of COVID-19 vaccine programmes to include additional doses or to vaccinate new cohorts (including children). Changes to the aforementioned items are likely to result in new demand phases for specific vaccines in the future.
Conclusions
This paper has described the three demand phases for COVID-19 vaccination, highlighting that there is a range of different challenges and solutions across each of these phases. Countries and COVID-19 vaccine programme administrators should plan for these different phases and implement strategies to maximise COVID-19 vaccine uptake and reduce wastage. Given that vaccination rates are significantly decelerating globally, this paper focused on the challenges for the third phase of demand, which is defined by high supply and low demand.
By reviewing multiple datasets including vaccination rates, COVID-19 vaccine delivered and estimated excess doses in seven countries across the Central and West Asia region, we determined that these countries are currently in the third phase of demand. Importantly, these countries are adjusting upcoming orders and implementing strategies to consider decreasing demand.
With the aim of addressing challenges for the third phase of demand, we provided 10 recommendations to reduce wastage and maintain demand. These recommendations covered areas including vaccine hesitancy, vaccine deliveries, publishing national COVID-19 data, wastage, vaccine shelf life, cold chain capacity, redistribution of COVID-19 vaccine, considerations when accepting COVID-19 vaccine donations, as well as the importance of leveraging available logistics and health information data. While countries face challenges associated with decreasing demand for COVID-19 vaccination, we believe that these can be addressed through sufficient planning and deployment of a range of strategies to ensure increased uptake and reduced wastage of vaccine.
Data availability statement
Data are available in a public, open access repository.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Handling editor Seye Abimbola
Contributors BC, GR, LK and AB conceptualised the study. AB reviewed the literature, conducted the analysis, wrote the initial draft of the manuscript and made subsequent edits. GR and LK reviewed and edited an early draft of the manuscript. BC reviewed and edited the manuscript and provided overall supervision. All authors read and approved the final manuscript.
Funding This study is funded by the Asian Development Bank. The findings, interpretations, and conclusions expressed do not necessarily reflect the views of ADB, its Board of Governors, or the governments they represent. Any designation of or reference to a particular territory or geographic area, or use of the term “country” is not intended to make any judgments as to the legal or other status of any territory or area. Boundaries, colors, denominations, and other information shown on any map do not imply any judgment on the part of the ADB concerning the legal status of any territory or the endorsement or acceptance of such boundaries.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein) or of any geographical or locational reference does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.