Article Text

Statistics from Altmetric.com
Summary box
Rabies, a fully preventable viral encephalitis, still claims at least 59 000 victims per year. Pre-exposure prophylaxis (PrEP) increases the probability of survival in bitten individuals but is hardly available to high-risk groups—like children—in endemic settings.
The availability of simplified PrEP schedules and new modes of administration with a focus on specific risk groups should be seen as game-changers for PrEP feasibility in low-income and middle-income countries.
We contend that there is a moral imperative to change the current paradigm where PrEP is available for international travellers to endemic regions but not to local individuals at risk.
We call for a global effort to make simplified rabies PrEP available and affordable to those in need.
Introduction
On September 28 this year, the World Rabies Day came as a reminder that a fully preventable viral encephalitis still claims at least 59 000 victims per year in over 150 countries; and particularly in rural Africa and Asia, where over 40% of individuals bitten by a suspect rabid animal are children. Sadly, these figures are probably underestimated.1
Rabies is one of the Neglected Tropical Diseases (NTDs) announced by the WHO, that is, a diverse group of communicable diseases that particularly affect poor populations, without adequate sanitation, and living in close contact with infectious vectors. In 2013, the World Health Assembly called to intensify measures against NTDs.2 In 2015, the WHO called for action to achieve zero dog-mediated rabies deaths in humans by 2030.3 Therefore, it is crucial to enhance prevention, diagnosis, control and treatment through an integrated One Health approach. Pre-exposure prophylaxis (PrEP) with rabies vaccine plays an important role in prevention but is almost unavailable in high-endemic settings.
Pre-exposure and post-exposure prophylaxis
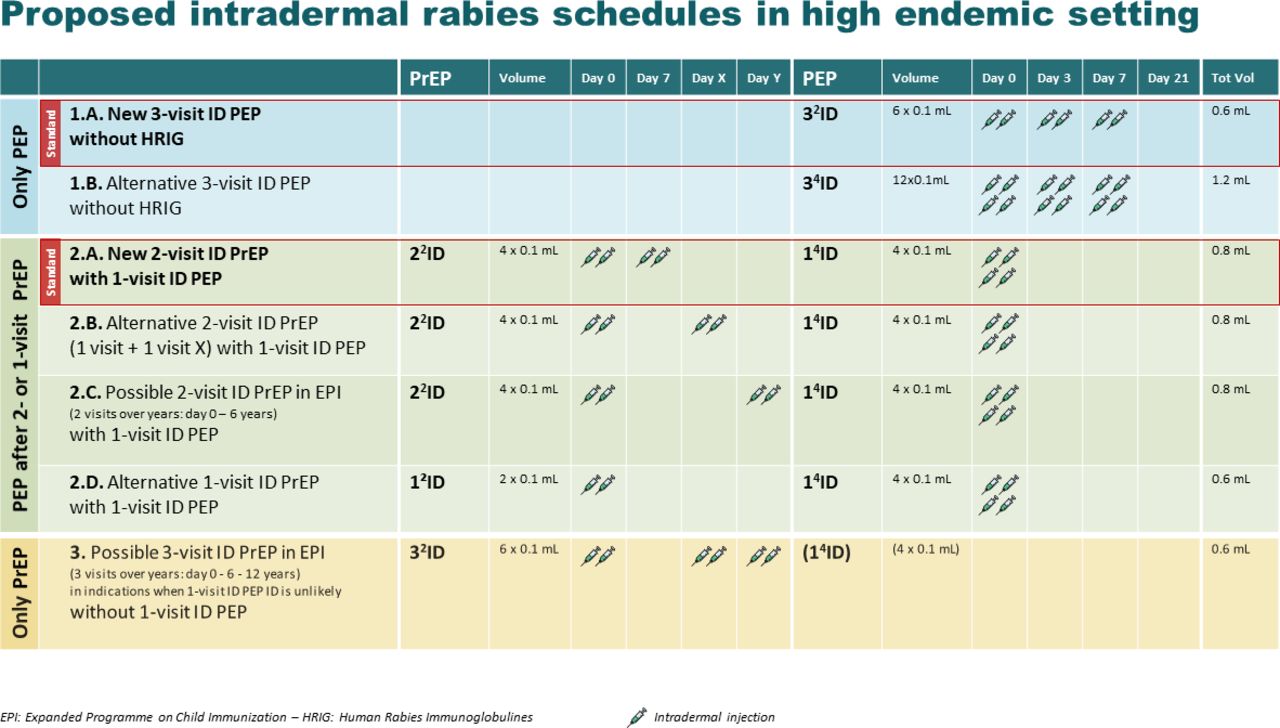
Post-exposure prophylaxis (PEP) vaccination is life-saving, if given as soon as possible after exposure. It requires several vaccination sessions and the availability of immediately acting but costly immunoglobulins (RIG). However, if individuals bitten by a rabid animal are ‘primed’ with PrEP, they only need as PEP a single-visit intradermal booster vaccination of 0.1 mL at four anatomical sites (figure 1: 14ID, schedule 2.A). Two clinical trials showed that even lower doses (single-site 0.1 mL or two-sites 2×0.1 mL) during a single-visit booster session can activate memory cells and trigger the immune cascade in primed individuals4 5 and induce an accelerated immune response compared with those who receive PEP alone.6 Additionally, primed individuals do not require RIG, which is complex to administer and mostly unavailable in low-and-middle-income countries (LMICs).7 In short, PEP without PrEP is slower-acting, time-sensitive and time-consuming, while PrEP increases the likelihood of survival in bitten individuals, particularly in case of so-called ‘category 3 exposure’ (eg, transdermal bites/scratches) when RIG is unavailable. Some authors even argued that PrEP might provide sufficient protection, if exposure goes unrecognised, or when PEP is delayed, incomplete or unavailable.6
{kind=link}
Proposed rabies schedules for pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP). ID, intradermal.
Traditionally, PrEP required three vaccinations spread over 1 month. Since 2018, the WHO recommends a simplified two-visit schedule, with two intradermal microinjections of 0.1 mL in each arm, on days 0 and 7 (figure 1: 2²ID). This schedule shows a robust immune response with a good safety profile in all age groups and the potential of high adherence.7 The (2018) WHO guidelines also recommend a simplified PEP (without PrEP) schedule with six intradermal microinjections of 0.1 mL at days 0, 3 and 7 (figure 1: 3²ID, schedule 1.A) instead of the current four to five visits over 21–28 days in combination with RIG. However, these conventional PEP schedules are still the first recommended strategy in LMICs where PrEP does not exist.
New perspectives
Given the life-saving potential of the prime-and-boost approach, it may come as a surprise that the WHO does not recommend inclusion of rabies PrEP in expanded immunisation programmes (EPI), apparently due to doubts about cost-effectiveness.7 8 However, is PrEP really not cost-effective? We argue that factors such as the availability of shorter schedules, new modes of administration and focus on specific risk groups could change this economic equation.
Cost-effectiveness
To the best of our knowledge, Peru and the Philippines are the only two middle-income countries that transiently provided three-visit PrEP vaccination for children in highly endemic areas.6 A study from the Philippines suggested that, assuming an annual bite incidence of 2.6%, a 31ID PrEP followed by 21ID PEP, is more cost-effective than a 32+11 ID PEP plus equine RIG.9 Conversely, a modelling study from Thailand suggested cost-effectiveness only if the bite incidences were between 3% and 23% in the target population depending on the PEP given. As an actual bite incidence of 2.3% was calculated (meaning 30% of the children had been bitten by the age of 15 years), three-visit PrEP was not introduced.6 Overall, more research is needed to clarify issues of cost-effectiveness.
Optimisation of resources
Recent trials suggest that a simulated PEP booster—delayed for years—in combination with a 2²ID or 1²ID PrEP will improve the anamnestic responses after the booster.4 Hence, instead of three vaccinations in 1 week (32ID PEP), the 2²ID PrEP schedule, followed by a 14ID PEP in case of exposure, can improve feasibility in endemic LMICs due to longer time intervals (figure 1: schedule 1.B, 1.C, 1.D). Countries can also consider a double-dose schedule at three different visits, using the 32ID PEP vaccinations in a PrEP schedule, which would fit in the EPI programme: at the age of 9–12 months, and at the age of 6 and 12 years (figure 1: schedule 3).
In addition to improving feasibility, the simplified regimens imply better adherence and lower costs. Recent research findings suggest that even single-visit ID PrEP and PEP schedules would be safe and immunologically adequate in adults.7 A study from Thailand in children and adults suggested sufficient protection after a simulated single-visit PEP (14ID) 5 years after priming.10 More research is urgently needed to evaluate single-visit schedules, particularly in vulnerable groups like children in endemic settings.7 Long-term prospective trials should assess repeated bite exposure and longer booster intervals, to understand the optimal spacing of boosters over a lifetime; evaluation of cost-effectiveness should be systematically included.
It is generally estimated that a vaccine vial containing one intramuscular dose (0.5 or 1.0 mL) can be used for 4 up to 10 intradermal injections (0.1 mL).8 Hence, implementation of rabies PrEP would become cheaper if vials and needles were manufactured for administration with intradermal devices, allowing to reduce the volume.11 Existing needle-free injection devices could be trialled for rabies vaccination; the results of a study that assessed such a device in 268 subjects are pending. Further data will be needed to validate these tools in rabies PrEP and PEP.
Regrettably, the Philippines discontinued the PrEP programme due to vaccine shortages, indicating a need to increase the worldwide production.6 Otherwise, there is a risk that production predominantly addresses the needs of those high-income countries that (rightly) promote PrEP in travel clinics. Investing in prequalified vaccines becomes attractive, if there is an opportunity to become suppliers for countries and for international agencies. An explicit demand from countries could result in higher production volumes and therefore economies of scale, facilitating preferential prices to endemic LMICs. In the long term, manufacturers could adopt new technologies such as microfacilities reducing production costs with low ecological footprints.12 Vaccines with improved thermostability, longer shelf-life and reduced packaging volume would ease transport and delivery at community level.7
Raising awareness
Sensitisation and education of those at risk, their caregivers and communities, remains critical to ensure awareness of how to avoid exposure, recognise the risk and timely access, start and complete treatment. Social science research, codesigned with the community, is needed to understand perceptions, expectations and fears and to develop locally tailored communication and sensitisation tools.
Containment of the reservoir
The importance of veterinary interventions cannot be overemphasised: dog vaccination is relatively inexpensive and it could eliminate dog-mediated rabies by 2035, thus ending 99% of human cases. However, it needs to reach at least 60%–70% of the dog population and requires long-term vigilance and continued political commitment.7 In recent years, large-scale efforts were successfully launched worldwide. Ideally, dog vaccination campaigns would be linked to PrEP vaccination campaigns for humans in the next coming years.
A moral imperative
Everyone has the right to promotive, preventive, curative and rehabilitative health services of quality without financial hardship.13 Yet the vaccine-preventable disease rabies kills one child about every 20 min—now and every day to come until elimination.
Are you still thinking of the lack of cost-effectiveness of PrEP for Thai children and of the vaccine shortage in the Philippines? Meanwhile, a monthly bite risk of 0.3%–1.5% in travellers to highly endemic settings resulted in a major mind-shift in favour of PrEP in this group.14 15 While we agree that rabies PrEP is actively promoted in international travellers, we contend that there is a double standard: why is PrEP available for travellers to endemic regions but not to those who are born there, who share a similar or higher risk? This gap in access is morally questionable, and even more now that simplified schedules can lower costs and improve feasibility of PrEP, particularly 2²ID +14 ID (figure 1: 2.A-2.B-2.C).
Low-cost intradermal PrEP should be offered to all infants and children in high-endemic countries, either as part of the EPI or through mass campaigns. We call politicians, policy makers, the public and private sectors, the civil society, academia, governments and donors to join forces in this effort, as part of the collective moral obligation to promote and support universal health coverage.
Footnotes
Handling editor Seye Abimbola
Twitter @RRavinetto
Contributors This commentary is based on the research experience of the authors in the field of rabies vaccines. PS and NB-R wrote the first draft, which received significant inputs from RR, EB, PVD and YVH. PS, RR and NB finalised the manuscript, which was approved by all coauthors. PS is the guarantor of this commentary and the corresponding author.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement No data are available.