Article Text

Abstract
Introduction Electricity outages are common in low/middle-income countries and have been shown to adversely affect the operation of health facilities; however, little is known about the effect of outages on the utilisation of health services.
Methods Using data from the 2015–2016 India Demographic Health Survey, combined with information on electricity outages as reported by the state electricity provider, we explore the associations between outage duration and frequency and delivery in an institution, skilled birth attendance, and caesarean section delivery in Maharashtra State, India. We employ multivariable logistic regression, adjusting for individual and household-level covariates as well as month and district-level fixed effects.
Results Power outage frequency was associated with a significantly lower odds of delivering in an institution (OR 0.98; 95% CI 0.96 to 0.99), and the average number of 8.5 electricity interruptions per month was found to yield a 2.08% lower likelihood of delivering in a facility, which translates to an almost 18% increase in home births. Both power outage frequency and duration were associated with a significantly lower odds of skilled birth attendance (OR 0.97; 95% CI 0.95 to 0.99, and OR 0.99; 95% CI 0.992 to 0.999, respectively), while neither power outage frequency nor duration was a significant predictor of caesarean section delivery.
Conclusion Power outage frequency and duration are important determinants of maternal health service usage in Maharashtra State, India. Improving electricity services may lead to improved maternal and newborn health outcomes.
- electricity, power outage
- global health
- maternal health
- Asia
- India
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Electricity outages are frequent in many low/middle-income countries and have been shown to adversely affect the operation of health facilities.
Increasing the proportion of births that occur in a healthcare facility and that are attended by a skilled health professional is considered important in improving maternal and newborn health outcomes.
What are the new findings?
Our results demonstrate that the frequency of power outages is a significant predictor of both institutional deliveries and skilled birth attendance in Maharashtra State, India, while the duration of power outages is a significant predictor of skilled birth attendance.
This translates to an almost 18% increase in home births in a typical month assuming the average number of electricity interruptions (8.5) occurs.
What do the new findings imply?
The study findings suggest that improving electricity supply, specifically by reducing the frequency and duration of power outages, may result in increased rates of institutional deliveries and skilled birth attendance, which may lead to improved maternal and neonatal health outcomes in the long run.
Until reliable 24 hour power for all has been achieved, interventions to mitigate the impact of power outages on maternal health service usage are needed.
Introduction
Access to electricity is necessary to promote economic development, and has been associated with a number of development outcomes, including increased rates of female labour participation,1 2 higher school enrolment3 4 and improved health. Indeed, electrification rates have been found to be correlated with lower infant and maternal mortality across Indian districts,5 higher rates of immunisation and prenatal care in Pakistan6 and improved nutritional status in children in rural Bangladesh.7 Given its importance, expanding access to electricity, particularly in rural areas, is a global priority, and ensuring ‘universal access to affordable, reliable, sustainable, and modern energy’ has been selected as target 7 of the newly adopted Sustainable Development Goals. Despite this, approximately 15% of the world’s population (almost 1.1 billion people) still did not have access to electricity as of 2016 (Energy Access Outlook, 2017), and almost one-quarter of these people live in India.
Unreliable electricity supply can severely impede health service provision, affecting both the operation of health facilities and the quality of care received at these facilities. Power outages can cause interruptions in the use of essential medical and diagnostic devices, for instance, and may limit communication, both within healthcare organisations and between patients and healthcare providers.8 Furthermore, unreliable electricity can make it difficult to provide lighting or to refrigerate vaccines and medications properly in healthcare centres, hindering even the most basic maternal delivery and emergency procedures.9 10 Only a few studies have investigated the role of electricity in the demand and supply of health services. One study in Ghana, for instance, found that the risk of mortality increased by 43% on days in which facilities experienced a power outage for 2 or more hours11; however, it is unclear how generalisable these findings are to other contexts.
A country of approximately 1.3 billion people, the demand for power in India exceeds the current supply and electricity outages are common events.12 In one notable event in July 2012, over 620 million Indians lost power in the largest grid failure in human history. Although the Prime Minister of India pledged over 160 billion rupees (US$2.5 billion) in 2017 to electrify every household in India by the end of 2018, and to give 24 hour power to all by March 2019,13 access to reliable electricity remains an important issue in Indian healthcare facilities, and power outages have been blamed for a number of high mortality incidents across the country, the majority of which were caused by the failure of life-sustaining equipment such as ventilators and incubators.14–16
In addition to direct harm caused to patients, there is also concern that the frequent power outages occurring across India may affect care-seeking behaviours, particularly among expectant mothers. Although India has shown substantial progress in improving maternal health outcomes over the past few decades, the country continues to see high numbers of maternal deaths each year, and the Indian government has thus made increasing the proportion of births that take place in health facilities a key priority.17 A number of determinants of institutional deliveries have been identified, both in India and internationally, and, in addition to factors such as mother’s age and education, urbanicity, socioeconomic status and birth order, include distance and travel time to a facility, and quality of care,18–20 all of which may be affected by power outages. Healthcare facilities experiencing electricity outages may provide lower quality services, for example, due to a lack of lighting or an inability to operate certain medical equipment, or may be less able to accommodate new patients, increasing a woman’s odds of being turned away. Power outages may also impact transportation networks, limiting a woman’s ability to get to a healthcare facility, or may cause a woman to stay home in anticipation of reduced quality of services. Conversely, facilities that do have a generator may become a popular destination during electricity outages, resulting in an increase in the number of people seeking care and thus staff shortages and heightened wait times, or may lead to a woman travelling farther than usual in order to reach these facilities.
Despite these potential mechanisms, there has been little investigation in any international context into the association between electricity outages and the use of maternal health services. Given this gap, this study aims to quantify this effect using a population of women from Maharashtra, India; a state of 112 million people, in which power outages are common. Specifically, we assess the association between the frequency and duration of power outages in any given month and a woman’s likelihood of giving birth in a healthcare facility, as well as the likelihood that the birth is attended by a skilled healthcare practitioner, and the likelihood that the delivery is via caesarean section. The results of this paper will provide greater insight into the role of electricity in maternal health service usage and may inform future strategies to improve maternal and neonatal health outcomes.
Methods
Data source
The data analysed in this study come from the 2015–2016 India Demographic Health Survey (DHS); a large, nationally representative household survey of women of reproductive age (15–49 years). Our sample was restricted to women residing in the state of Maharashtra, due to the availability of high-quality data on electricity outages within this state. The sample was trimmed to eliminate months at the beginning and end of the survey period, in which there were only a small number of live births (<100) per month. The final sample thus spans the time period August 2010 to May 2015.
Patient and public involvement
No patients were directly involved in this study.
Measures
Institutional delivery rates were measured using self-reported data on the location of delivery of all live births within 5 years of the date of the survey. Response options included at home, at another person’s home, in a government hospital or facility, in another public facility, in a private hospital or clinic, or in another private sector facility. For analyses, location of birth was considered a binary variable and was coded as a non-institutional delivery if the birth occurred at home or at another person’s home, and an institutional delivery if it occurred in a government hospital or another public facility, or in a private hospital or another private sector facility. Information on whether or not the delivery was assisted by a skilled health professional, defined as a doctor, auxiliary nurse, or midwife (binary variable with response options yes and no), and whether or not a caesarean section was performed (binary variable with response options yes and no) was also collected and was used as outcome variables in secondary analyses.
Power outages were measured using electricity reliability data from the Maharashtra State Electricity Distribution Company (MahaDiscom), India’s largest power distribution utility, based on System Average Interruption Frequency Index (SAIFI) and System Average Duration Index (SADI) values, which describe the average number of and duration in minutes of sustained power interruptions per consumer in a given time period, respectively. For analyses, both SAIFI and SADI indices were treated as continuous variables.
Additional data on both the mothers and the households included in the sample were extracted from the DHS. For mothers, this included age in years (continuous), birth order of the child, which was considered a proxy for parity (continuous), and educational attainment (ordinal categorical variable with categories uneducated, at least some primary, at least some secondary and at least some tertiary). For households, this included urbanicity (binary categorical variable with categories urban and rural) and primary religion of the household (Hindu, Muslim, or other), which was included based on the findings of previous studies that suggest religious differences in the use of maternal health services. DHS calculated wealth indices for each household were also used to generate wealth quintiles for the state of Maharashtra (ordinal categorical variable).
Data analysis
Statistical analyses were conducted using R V.3.4.3. Descriptive statistics including means for continuous variables and percentages for categorical variables were calculated to describe the characteristics of the sample, as well as variations in the SAIFI and SAIDI power outage indices and in locations of delivery in Maharashtra over the survey period.
Multivariable binary logistic regression models were used to assess the relationship between the frequency and duration of power outages in any given month and delivery in a healthcare facility, controlling for individual and household-level covariates, and to determine which factors were most predictive of delivery in a facility. Secondary analyses using birth attendance by a skilled health professional and caesarean section delivery as the outcomes of interest were also performed. Subgroup analyses were used to further assess each relationship, in order to determine if power outages have different effects on maternal healthcare service use among different groups of the population. Specifically, each analysis was stratified by urbanicity, household electrification and socioeconomic status.
Additional analyses including multinomial logistic regression to determine whether power outage indices predict the odds of births occurring in public hospitals, private hospitals, or at home, logistic regression using extreme power outage frequency and duration, classified as a monthly power outage frequency or duration greater than the mean for the entire time period, as the predictor variables, logistic regression using whether or not the minimum recommended antenatal care visits were made as the outcome variable, and logistic regression using a restricted sample of each woman’s most recent birth only, were also conducted.
All models were adjusted for month and district-level fixed effects. Fixed effects for month were included to account for differences in both power outages and facility deliveries which may be due to events that are more common during certain months, such as extreme heat or other weather events, festivals and holidays. District-level dummy variables were included to account for any unobserved, district-specific characteristics, such as the number of healthcare facilities in the district, the availability of skilled healthcare professionals, the physical quality of the healthcare facilities and the local road network. A monthly linear time trend was also used to capture time-varying unobservable factors, such as overall adoption of new technologies, that could be correlated with the number of facility deliveries and electricity outages over the sample period. Multivariable regression was used to assess the effect of the power outage indices on several maternal characteristics including age at time of birth, education, wealth and place of residence, in order to rule out possible selection bias (see online supplementary appendix table 1). Bayesian generalised model estimation was employed in order to overcome perfect separation among non-electrified households. Unadjusted and adjusted estimates are presented. Bootstrapped SEs were used to minimise the spatial correlation between the error terms and 95% bootstrapped CIs are presented.
Supplemental material
Results
Characteristics of the sample
Sample demographics and information on power outage frequency and duration are presented in table 1. In total, 9125 births were reported within 5 years of the survey date. Mothers were an average of 25.95 years old at the time of the survey, and the majority, approximately 67%, had at least some secondary education. About a third lived in an urban setting, and 93% had electricity at home. Just 37% of women reported that distance to a health facility was not a problem for them, while almost one-quarter perceived distance to be a major barrier to accessing healthcare. The sample was evenly distributed across the wealth quintiles (not shown). Hindu was the most common religion and made up three-quarters of the sample. The vast majority of deliveries, approximately 89%, took place in a public or private health facility, compared with just 11% at home. Online supplementary appendix figure 1 demonstrates that the proportion of births in each location remained relatively stable over the study period, although a slight increase in public facility deliveries and slight decrease in home deliveries were observed overall. Correspondingly, 90% of births were attended by a skilled healthcare professional. About one in five deliveries were via caesarean section, and fewer than three-quarters of women obtained the recommended four or more antenatal care visits for her most recent delivery. On average, households experienced power outages about 8.5 times in any given month and these outages totalled to around 92 min/month.
Supplemental material
Characteristics of the sample
Electricity in Indian health facilities
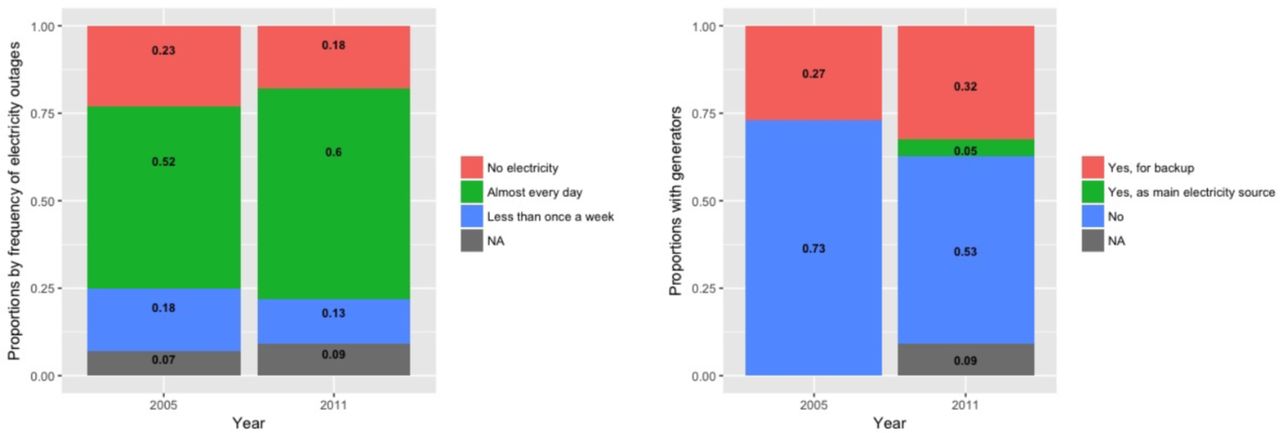
Figure 1 presents data from the 2011–2012 India Human Development Survey, which collected information on health facilities, including generator ownership. Overall, the proportion of health facilities with no electricity decreased by 5% from 2005 to 2011, however 18% still did not have access to electricity in 2011 and the proportion experiencing an outage almost every day increased. Similarly, the proportion of facilities without a generator decreased from 2005 to 2011 and a new category of facilities which used a generator as their main electricity source emerged. We were also able to evaluate monthly variations in the duration and frequency of power outages in Maharashtra State over the study period, the results of which are presented graphically in online supplementary appendix figure 2. A general downward trend in the frequency of electricity outages was observed between 2010 and 2015, while the duration of outages appeared to increase overall, although seasonal variation was apparent for both indices, with the number of frequencies peaking from May to October and the duration from June to October.
Supplemental material
{kind=link}
Electricity in Indian health facilities. NA, not applicable.
Relationship between power outages and delivery in a healthcare facility
The relationship between a woman’s likelihood of delivering in a healthcare facility and the frequency and duration of power outages is evaluated in table 2, with the marginal effects at the mean presented in online supplementary appendix table 2. Overall, an increase in the frequency of power outages was associated with a significantly lower odds of delivering in a healthcare facility, and this was true in both unadjusted (column 3) and adjusted (column 6) analyses. Specifically, each additional power outage instance was associated with a 2.08% (OR 0.98; 95% CI 0.96 to 0.99) lower odds of delivering in an institution, adjusting for individual-level covariates and month and district fixed effects; approximately a 17.68% lower odds if the mean of 8.5 monthly power outages occurs. In column 9, we also include household electrification status as a covariate in the model which leads to the outage frequency variable just failing to be a significant predictor of institutional delivery, though the effect size remains consistent. As electricity status is included in the calculation of the wealth index in the DHS, we suspect the inclusion of a potentially correlated variable may have affected our ability to find a significant effect, but we present these results to show that our effect size is consistent when this variable is included in the model.
Supplemental material
Effect of power outage indices on institutional delivery (log odds)
In examining the effect of the duration of power outages on a woman’s likelihood of delivering in a healthcare facility, the relationship was less consistent. In crude analyses, for example, a significant positive association was observed, however after adjusting for individual and household characteristics and month and district fixed effects, there was an insignificant negative relationship, with each increase in the duration of power outages of 1 min associated with a 0.20% (OR 0.99; 95% CI 0.99 to 1.00) lower odds of delivering in an institution.
Table 3 explores these relationships among key subgroups of the population, namely by urbanicity, household electrification status, socioeconomic status and perception of distance to a facility. Negative but non-significant associations between power outage frequency and delivering in a healthcare institution were observed for both urban and rural and low-wealth and high-wealth mothers, while among women who perceived distance to health facility as a major issue in accessing care, a statistically significant reduction in the odds of institutional delivery of 3.9% (OR 0.96; 95% CI 0.93 to 0.99) was observed, adjusting for individual and household-level covariates and month and district fixed effects.
Effect of power outage indices on institutional delivery: subgroup analyses (log odds)
In examining the effect of power outage frequency on delivering in a healthcare institution in electrified compared with non-electrified households, we found a statistically significant reduction in the odds of institutional delivery of 2.57% (OR 0.97; 95% CI 0.95 to 0.99) for women who resided in electrified households, adjusting for individual and household-level covariates and month and district fixed effects, but a small, non-significant positive association for women in non-electrified households. This discrepancy could also explain why adjusting for household electrification nullified the relationship between power outage frequency and institutional delivery in the full sample analysis. Similar trends emerged when assessing power outage duration as the independent variable, with small and non-significant negative effects observed for all subgroups, with the exception of women in non-electrified households, for whom there was again a small and non-significant positive relationship.
Relationship between power outages and birth attendance by a skilled professional
The relationship between the likelihood that a birth is attended by a skilled healthcare professional and the frequency and duration of power outages was also investigated and is presented in table 4. Both indices are significantly associated with a reduced odds of birth attendance by a skilled professional in full sample analyses, with a 2.76% (OR 0.97; 95% CI 0.95 to 0.99) lower odds observed for each additional power outage instance and a 0.40% (OR 0.996; 95% CI 0.992 to 0.999) lower odds observed for each additional minute of outage duration, adjusting for individual and household-level covariates and month and district fixed effects. In subgroup analyses, power outage frequency remained a statistically significant predictor of skilled birth attendance for urban women (OR 0.95; 95% CI 0.91 to 0.99), women residing in electrified households (OR 0.97; 95% CI 0.95 to 0.99) and women of high wealth (OR 0.96; 95% CI 0.91 to 0.99), while power outage duration was significantly associated with a reduced odds of skilled birth attendance for rural women (OR 0.995; 95% CI 0.990 to 0.999), and women residing in electrified households (OR 0.996; 95% CI 0.991 to 0.999), adjusting for individual and household-level covariates and month and district fixed effects.
Effect of power outage indices on skilled birth attendance (log odds)
Relationship between power outages and caesarean section delivery
The relationship between the likelihood of delivery via caesarean section and power outage frequency and duration is demonstrated in table 5. No statistically significant associations were observed between the power outage indices and caesarean section delivery in either the full sample or the subgroup analyses.
Effect of power outage indices on caesarean section delivery (log odds)
Additional analyses
The results of a series of additional analyses are presented in online supplementary appendix tables 3–6. Online supplementary appendix table 3 assesses the association between power outage frequency and duration indices and whether a birth takes place in a public hospital, private hospital or at home. Using home delivery as the reference category, we found that a higher frequency of power outages was associated with a 2.27% lower odds of delivering in a private facility (OR 0.98; 95% CI 0.96 to 0.99) and a 2.08% lower odds of delivering in a public facility (OR 0.98; 95% CI 0.96 to 0.99), controlling for covariates. In subgroup analyses, power outage frequency was significantly associated with a reduced odds of delivering in a public facility for rural women and a reduced odds of delivering in a private facility for low-wealth women.
Supplemental material
Online supplementary appendix table 4 evaluates the effect of extreme power outages, which take a value of 1 if the frequency and duration indices for a given month are greater than the average of each outage index, on institutional delivery. No significant associations were observed in full sample analyses, however subsample analyses reveal that extreme power outage frequency yields a 27.39% lower odds of delivering in a healthcare facility among low-wealth women (OR 0.73; 95% CI 0.53 to 0.95), suggesting that the poor may be the most vulnerable to extreme events.
Supplemental material
Online supplementary appendix table 5 investigates the relationship between power outage frequency and duration indices and the likelihood of a woman attending four or more antenatal care visits. We found no statistically significant association in either full sample or subsample analyses.
Supplemental material
Lastly, online supplementary appendix table 6 evaluates the effect of the power outage frequency and duration indices on the likelihood of institutional delivery in a restricted sample, consisting only of each woman’s most recent birth. Overall, increased power outage frequency was associated with a 3.54% lower odds of delivering in a facility (OR 0.96; 95% CI 0.94 to 0.99), while increased power outage duration was associated with a 0.6% lower odds (OR 0.994; 95% CI 0.988 to 0.999). In subsample analyses, both power outage frequency and duration remained significant predictors of institutional delivery among women from electrified households, while in rural households, low-wealth households and high-wealth households, power outage frequency was significantly negatively associated with institutional delivery.
Supplemental material
Discussion
This study investigated the impact of power on rates of healthcare facility delivery in Maharashtra State, India, as well as on skilled birth attendance and caesarean section delivery. Using data from the 2015–2016 India DHS, we found that, controlling for other previously identified determinants, including urbanicity, household wealth, maternal education, age, parity and religion, electricity interruptions were associated with a statistically significant reduction in a woman’s likelihood of giving birth in a healthcare institution. Specifically, each additional electricity interruption was found to yield a 2.08% lower likelihood of delivering in a facility, which translates to an almost 18% increase in home births per month if the average number of 8.5 power outages occurs. These findings are in line with the results of previous studies, such as that by Ghosh,21 who identified a positive association between maternal health services use and an index of development indicators which included access to electricity. Interestingly, power outage duration was not a significant predictor of institutional delivery in either full or subsample analyses. We speculate that these findings may be consistent of evidence that power outages directly affect women’s decision to seek care: a woman may decide to stay home if there is an outage but without any knowledge of how long the power outage will last.
Along with reduced odds of delivering in a facility, our results demonstrated a significant association between both more frequent and longer power outages and a reduced likelihood of a skilled health professional attending the birth in full sample analyses. In subsample analyses, the effect of power outage frequency was stronger in urban women, women from electrified households and women of higher wealth status, while the effect of power outage duration yielded greater reductions in the odds of skilled birth attendance in rural women, and women from electrified households. These discrepancies may indicate that, even among those who are better able to access healthcare, due either to physical proximity or increased financial resources, the quality of care received may be reduced during a power outage. For example, personnel shortages during a blackout may result in some women delivering without a healthcare professional in attendance even within a facility, while power outages may make it more difficult for a woman to communicate with health professionals, preventing them from attending home deliveries.
Importantly, we did not observe any significant association between electricity interruptions and the likelihood of a caesarean section delivery. This lack of a statistically significant relationship may be due to the fact that caesarean sections are generally emergency procedures that require specialised health professionals and medical equipment and must therefore be performed in a healthcare facility, which may be more likely to own a generator. Indeed, rates of caesarean section are relatively modest overall, accounting for approximately 18% of births in our sample, and thus the majority of these procedures are likely non-elective, and are therefore given priority within a healthcare facility, even during a blackout.
Implications for policy and practice
This study highlights the importance of electricity in the use of maternal health services in India and suggests that improving the reliability of the supply may be an effective strategy for increasing the proportion of births that occur in a healthcare facility or are assisted by a skilled health professional in Maharashtra State, India. Given the link between institutional delivery, skilled birth attendance and maternal and neonatal mortality rates,22 23 this finding is important and reflects the need to develop programmes and policies that aim to improve the quality of electricity in India. Such efforts could take the form of increased financial investments in power, and Prime Minister Narendra Modi’s recent commitment to give 24 hour power to all by March 201913 is a promising start. Additionally, programmes that attempt to reduce the impact of electricity interruptions on maternal health service usage may be an important short-term strategy, and could include supplying facilities with additional generators or implementing mobile clinics, which would allow women to receive the care they need even when they are not able to deliver in an institution, for example, due to a power outage. Mobile clinics already exist in some low/middle-income countries such as in Tanzania, where they have been found to improve coverage of maternal and child health services to underserved populations,24 and are now being implemented in India. Expanding the presence of trained midwives in low/middle-income countries may also prove effective at increasing skilled birth attendance, particularly in rural areas where healthcare facilities are often few and far between. Increased midwife availability would reduce the need for women to travel to give birth during a power outage, and would eliminate any concerns about the quality of care received. Indeed, there is evidence to suggest that attendance at delivery by trained midwives can reduce maternal mortality in resource-poor settings,25 and the WHO has thus promoted midwifery as essential in improving maternal and infant health outcomes in low/middle-income countries.26 Despite this evidence, the Government of India has not invested substantially in midwifery training,27 and there is thus a shortage of midwives in the country, with only about 2.4 nurses and nurse-midwives per 10 000 people, the majority of whom remain concentrated in urban centres.28 Improving access to midwives would therefore result in positive outcomes, both in times of electricity interruptions and not.
Limitations
This study is not without limitations. First, although the availability of high-quality power outage data made Maharashtra State a suitable setting in which to conduct this study, it may not be representative of the country of India as a whole, or of other low-income countries in which electricity interruptions may be an issue. Indeed, Maharashtra State has high rates of electrification relative to the national average, and comparatively good maternal and child health indicators. While we do not have data for other states, it is probable that these areas also experience power outages, likely at higher rates than the relatively well-off Maharashtra State, and that they have even lower rates of institutional delivery. Therefore, it can be assumed that power outages are also an important determinant of delivering in a healthcare facility in these other states, and may in fact be an even greater impediment. Furthermore, our measures of power outages are weighted state averages for all mothers, regardless of their connection to the electricity grid and place of residence, and not all are likely to be affected in the same way. We also do not have data on the exact date of each birth, nor the exact date of the power outages. While more precise data would likely have allowed us to make more precise estimates of the impact of outages on delivery rates, we do not believe it substantially biased our results. Finally, we do not have data on whether or not each health facility or household owned a generator. Such information may have potentially allowed for a deeper understanding of the mechanisms behind the aggregate effect that is measured in this study.
Conclusion
In this study of women in Maharashtra State, India, we provided new evidence of an association between electricity interruptions and maternal health service usage. Specifically, we found that more frequent power outages predicted a reduced odds of delivery in a healthcare facility for women from electrified households, while longer and more frequent power outages were associated with a reduced odds of birth attendance by a skilled professional. Given the importance of these outcomes in order to reduce maternal and neonatal mortality rates, our results reflect the need to reduce the frequency and duration of power outages in India and throughout the developing world. In the meantime, future research should focus on developing practices and policies to lessen the effects of these electricity interruptions on maternal health services so that adverse health impacts on women and babies are minimised.
Acknowledgments
We acknowledge that this work was conducted on the Haldimand Tract, traditional territory of the Neutral, Anishinaabe and Haudenosaunee peoples. We are grateful to the AXA Research Foundation for financial support for this project. We are also grateful for comments by participants at the Canadian Health Economists’ Study Group hosted by McGill University in Montreal in June 2018.
References
Footnotes
Handling editor Sanni Yaya
Contributors MK codeveloped the research idea and conducted the analysis, and authored the first draft of the manuscript. BRI edited and authored the manuscript. KG codeveloped the research idea and assisted with drafting and editing of the manuscript.
Funding This study has been funded by AXA Research Foundation, Future of Health Systems Award.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.