Article Text

Abstract
Introduction Mental disorders account for a substantial burden of disease and costs in low-income and middle-income countries (LMICs), but attract few resources. With LMIC governments often under economic pressure, an understanding of the external funding landscape is urgently needed. This study develops a new typology of external actors in global health adapted for the sustainable development goals (SDGs) era and uses it to systematically map available evidence on external actors in global mental health.
Methods The new typology was developed in line with conceptualisation in the literature and the SDGs to include 11 types of external actors for health in LMICs. Five databases (EconLit, Embase, Global Health, MEDLINE, PsycINFO) were searched for manuscripts published in peer-reviewed journals in English, French, Italian, Portuguese or Spanish between 1 January 2000 and 31 July 2018 and reporting information on external actors for mental disorders in LMICs. Records were screened by abstract, then full-text against inclusion criteria. Data were extracted and synthesised using narrative analysis.
Results 79 studies were included in the final review. Five were quantitative studies analysing the resource flow of development assistance for mental health globally over the last two decades. The remainder were qualitative studies providing a description of external actors: the majority of them were published in the last decade, focused on Africa, and on public sector (bilateral and multilateral governmental organisations) and third sector organisations (non-governmental organisations). Evidence was particularly scarce for for-profit organisations and individual households.
Conclusion This study reveals opportunities for unlocking additional funding for global mental health in the SDG-era from an ecosystem of external actors, and highlights the need to coordinate efforts and to use sustainable, ethical approaches to disbursements. Further research is needed to understand all external actors and the allocation of their contributions in different settings.
- global mental health
- sustainable development
- external actors
- low-income and middle-income countries
- typology
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- global mental health
- sustainable development
- external actors
- low-income and middle-income countries
- typology
- systematic review
Key questions
What is already known?
Governments lack the funding to address mental disorders in low-income and middle-income countries: identifying key external actors is therefore crucial.
What are the new findings?
In line with the United Nations sustainable development goals, the new typology of external actors in global health includes a wide range of actors.
79 scientific publications were found, highlighting the prominence of third sector organisations in global mental health and the lack of evidence on for-profit organisations and individual households.
What do the new findings imply?
A large ecosystem of external actors for mental disorders already exists presenting opportunities for unlocking additional resources, though coordination of efforts is crucial, and the use of a sustainable and ethical approach is a moral imperative.
Further research is needed to understand all external actors and the allocation of their contributions in different settings.
Introduction
More than 1 billion people live with mental disorders (including substance use disorders, self-harm and dementia),1 over three-quarters of whom live in low-income and middle-income countries (LMICs) and their number is projected to increase.2 Although effective and low-cost interventions are available,3 fewer than 10% receive support.4 Resources are scarce: mental disorders receive as little as 1.6% of LMIC government health budgets4 and 0.4% of development assistance for health.5 The Lancet Commission on Global Mental Health and Sustainable Development recently called for an increase in resources to address mental disorders, both domestically and externally.2
With most LMIC governments already under considerable economic pressure, external funding is urgently needed. In line with the Addis Ababa Action Agenda,6 the United Nations sustainable development goals (SDGs) recommend the mobilisation of additional external funding from a wide range of sources (eg, development assistance, foreign direct investments (FDIs), remittances) while assuring sustainability through local ownership and a gradual increase in domestic resources.7 It is therefore important to identify who those key external actors are in global mental health.
However, evidence is extremely limited. A rapid review8 on actors in global mental health, emphasises the prominence of donor states and identifies some non-state donors, such as philanthropists, private-sector foundations, and organisations using innovative financing mechanisms. Another study9 mapping the ecosystem of global mental health research funders includes some actors disbursing to LMICs, such as Wellcome Trust and Grand Challenges Canada.
This study has two aims: first to develop a typology of external actors in global health adapted for the SDG-era; second to use this typology to systematically map the evidence on external actors in global mental health in order to identify available evidence and opportunities for unlocking additional resources.
Methods
Typology of external actors in global health
To date the ecosystem of potential actors in global health has been explored either from a health governance or from a health financing perspective. The global health governance literature explores power relationships of a growing plurality of external development actors and the emergence of non-state actors (eg, philanthropic organisations, private industry, civil society organisations, global health initiatives) alongside state actors (eg, donor country governments, United Nations organisations, multilateral development banks).10 By contrast, the global health financing literature focuses mainly on donors, using a simplified path of resource flows from donor organisations representing the primary source of funding (eg, states, private industry, philanthropic organisations, individuals), through channel organisations disbursing funding to implementing institutions providing support in recipient countries (eg, development aid agencies, non-governmental organisations).11 The combination of the two perspectives, however, is yet to be done.
I propose a new typology of actors in global health adapted for the SDG-era which includes a wide range of external actors (figure 1). The new typology brings together the two aforementioned approaches: global health governance and global health financing. On the one hand, the plurality of actors from the global health governance literature allows an understanding of each actor not only as its own entity, but also as operating within a group of organisations sharing common characteristics, and part of a larger ecosystem. On the other hand, expanding the definition of channel organisations from the global health financing literature, in the new typology external actors include organisations and individuals not only channelling development assistance but also investments to institutions providing goods and services in LMICs.

Typology of external actors in global health: four overarching groups and their types of actors. DFIs, development financial institutions; GOs, governmental organisations; SME, small and medium enterprises.
First, I identified 11 types of organisations and individuals from the literature in global health governance and global health financing (Box 1). Second, I selected four overarching groups of financial actors in line with conceptualisations in the literature and in the SDGs7: public sector, private sector, third sector and multisector partnerships. Those groups were introduced to facilitate both the understanding of commonalities (eg, legal status and modus operandi) across actors and comparison with corresponding domestic actors. Finally, organisations were ordered by group.
External actors
Public sector
Governmental organisations in high-income and middle-income countries provide goods and services in low-income and middle-income countries (LMICs), in agreement with recipient country governments. Bilateral governmental organisations in agreement with recipient countries are funded by just one state and include aid agencies (eg, US Agency for International Development) and other governmental agencies investing in development (eg, ministries of foreign affairs or their equivalents, research councils). Multilateral governmental organisations are funded and composed by multiple states at the regional (eg, European Commission), international (eg, Colombo Plan), or global level (eg, WHO).
Development finance institutions (DFIs) are organisations offering financial products (eg, loans) in contexts where commercial banks would not usually invest, due to what might be perceived to be high political, socioeconomic or environmental risks. Bilateral DFIs are funded by just one state and provide financial products usually at a commercial rate (eg, US Overseas Private Investment Corporation). Multilateral DFIs provide financial products usually at facilitated rates and are funded by multiple states, at the regional (eg, African Development Bank), international (eg, Islamic Development Bank) or global level (eg, World Bank).
Private sector
Corporations and small and medium enterprises are for-profit organisations providing goods and services through foreign investments and corporate social responsibility (CSR) initiatives. Foreign investments include foreign direct investments (FDIs), foreign portfolio investments (FPIs) and commercial loans. FDIs are substantial physical invetsments and purchases usually made by corporations in another country. FPIs are foreign indirect investments made by corporations, financial institutions and private investors using both equity (eg, stocks) and debt instruments (eg, bonds). CSR includes financial and in-kind contributions, in both products and human resources.
Foundations include non-profit organisations either created and mainly funded by private-sector companies (eg, Microsoft Philanthropies) or created by wealthy individuals and their families and funded through gifts of shares or endowments (eg, Bill and Melinda Gates Foundation).87 They are often grant-making entities.
Individual households contribute through donations, including financial and in kind-contributions in goods or services, and private foreign investments. A small number of individuals are described as ‘high-net-worth’: individuals with financial assets greater than US$1 million. A different and larger group of individuals are diaspora movements, including almost three-quarters (186 million) of international migrants coming from LMICs.88
Third sector
Third sector organisations constitute the most heterogeneous group of non-profit organisations providing goods and services in LMICs. Among others, this group includes non-governmental organisations (eg, BasicNeeds), professional associations (eg, World Psychiatric Association) and research centres (eg, universities).
Multisector partnerships
Multisector partnerships are a similarly heterogeneous group of organisations arising from arrangements between actors from two or more sectors aimed to leverage additional funding for global health, usually for specific conditions. Amongst others, this group include global health initiatives (eg, Global Fund to Fight AIDS, Tuberculosis and Malaria) and innovation funds (eg, Dementia Discovery Fund).
Systematic evidence mapping
I used systematic evidence mapping instead of systematic review and meta-analyses because this was more appropriate for identifying actors given the extent of available evidence, not the strengths and directions of relationships or tracking funding.12 The only quality criterion was publication in scientific journals.
I followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) (see supplementary appendix 1). I systematically searched five medical and social sciences databases (EconLit, Embase, Global Health, MEDLINE, PsycINFO) for manuscripts published in peer-reviewed journals in English, French, Italian, Portuguese or Spanish between 1 January 2000 and 31 July 2018. Searches were run in August 2018. The search strategy was designed for MEDLINE combining MeSH terms with keywords for mental disorders, external actors, and LMICs, and then adapted for each database (see supplementary appendix 2 for full search strategy). Mental disorders were defined according to the WHO definition to include common and severe mental disorders, mental disorders in children, substance use disorders, self-harm and suicide, and some neurological conditions (dementia, epilepsy).13 External actors included all actors external to recipient countries as described in the new typology. LMICs were defined according to the World Bank classification.14
Supplemental material
To be included, manuscripts had to report information on external organisations or individuals providing financial or in-kind contributions to mental disorders in LMICs (eg, actor description, contributions, activities funded). Contributions had to target either people living with mental disorders, their families and other carers, or populations at risk (eg, people living with HIV infection and acquired immune deficiency syndrome, HIV/AIDS). Manuscripts had to be original articles using any study design or other scientific publications (personal communications, commentaries, letters and editorials). Grey literature was excluded. Supplementary searches included snowballing citations from the reference lists and tracking citations using Google Scholar.
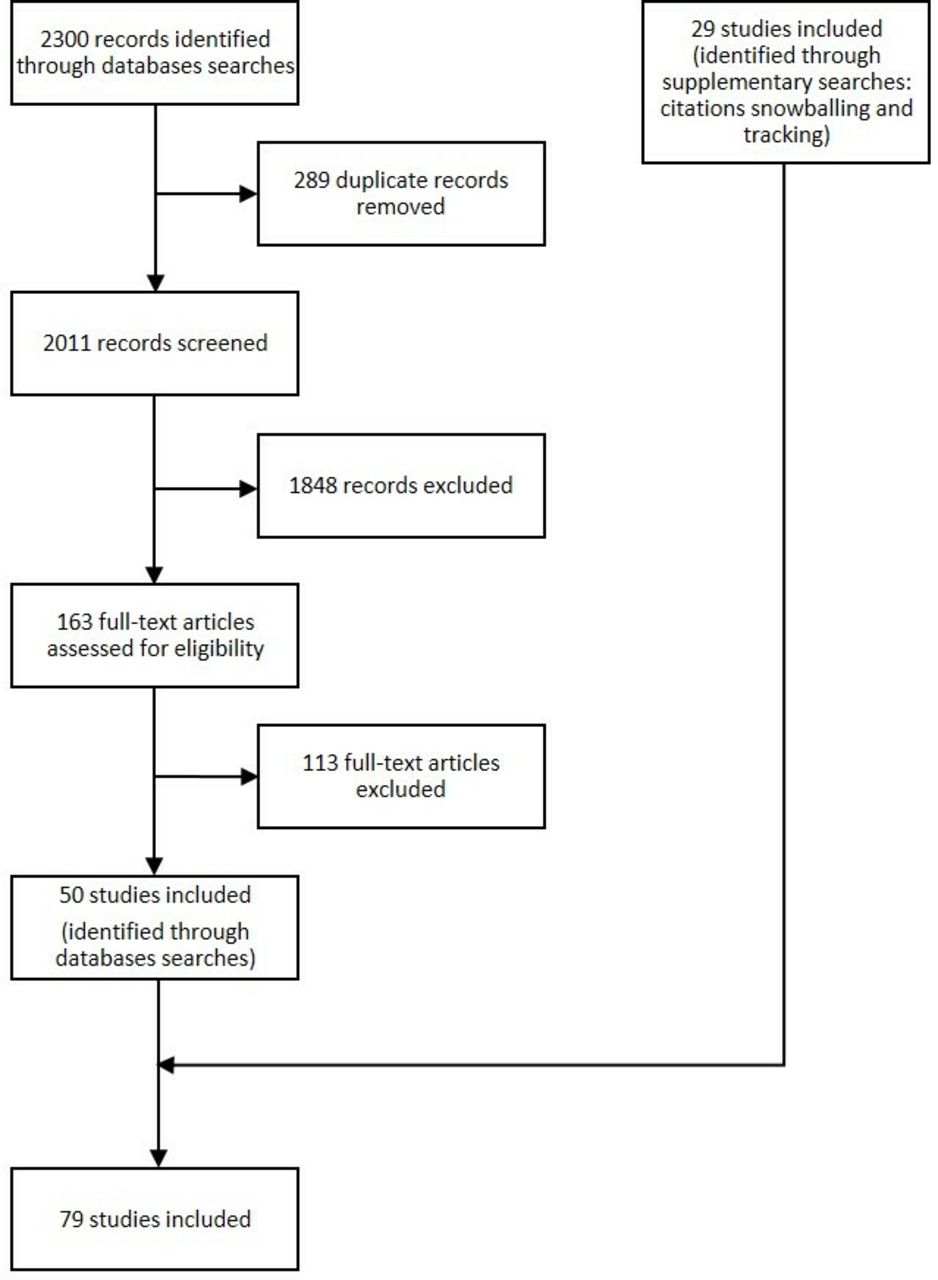
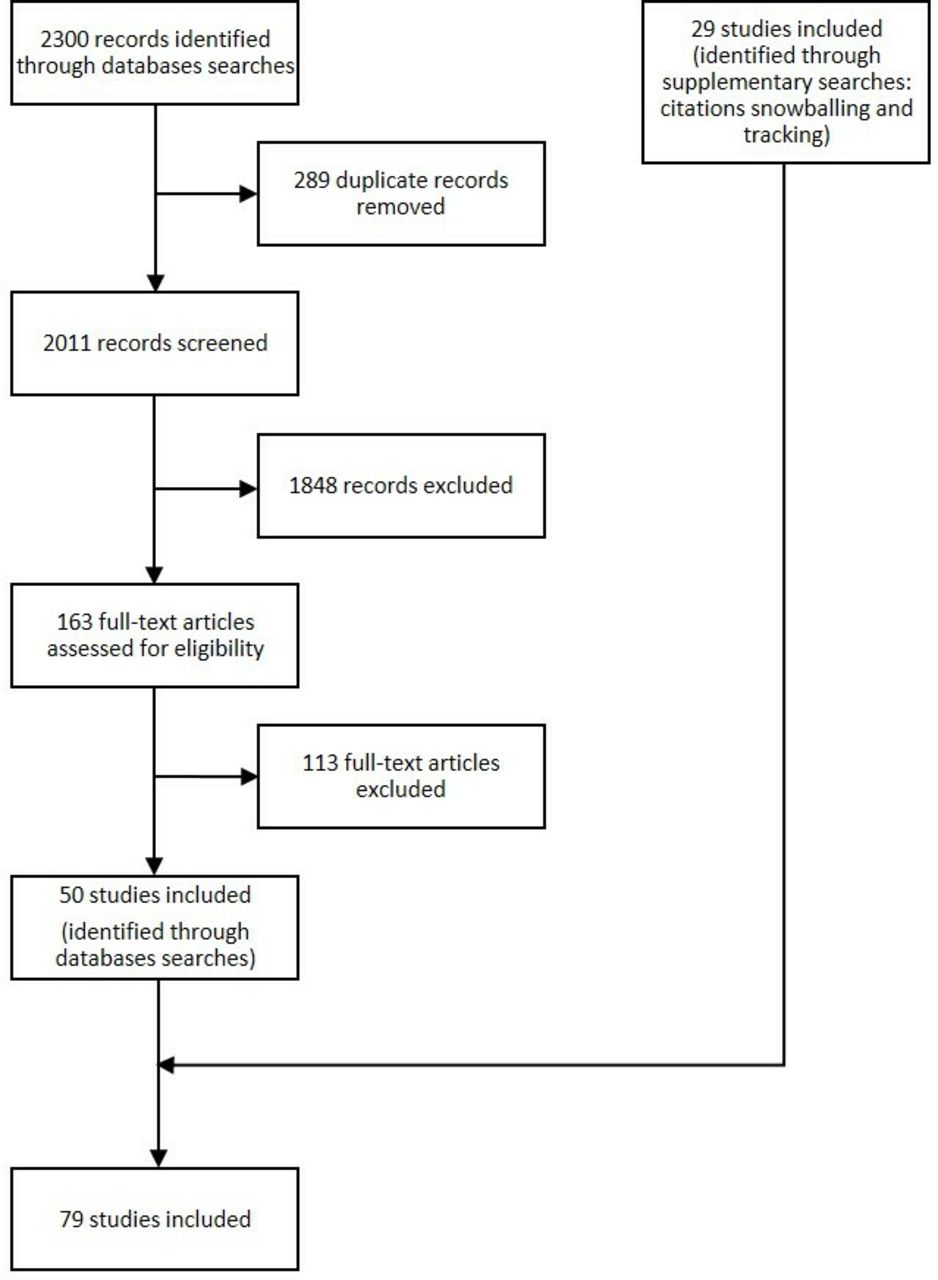
The database searches identified 2300 records (figure 2). After removing duplicates, the title and abstract of 2011 records were screened against the inclusion criteria using EndNote X8.15 Out of the 163 full-text articles assessed for eligibility, 50 were included in the review. The supplementary searches led to the inclusion of 29 additional records.
{kind=link}
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart.
I extracted data from the eligible manuscripts, including: publication characteristics (author, year), study characteristics (mental disorder, population, country, study type), and contributions from external actors (type of organisation, activities and revenues mobilisation). For quantitative studies only, additional study characteristics (dataset, years covered, type of analysis) were extracted. Data were extracted in Excel.16 Narrative analysis was used to synthesise findings.
Results
Five5 17–20 of the 79 studies analysed the resource flows for development assistance for mental health (DAMH) only, defined as financial and in-kind contributions disbursed from donors through channel organisations into LMICs with the aim of preserving or improving mental health (table 1). They were published over the last decade, had a global geographical focus, and include data on organisations from the public sector (bilateral and multilateral governmental organisations, multilateral development institutions), private sector (foundations), third sector (non-governmental organisations) and multisector partnerships (global health initiatives). They focused on disbursements for health activities only,7 humanitarian activities only,19 or activities in multiple areas (eg, health, humanitarian, education, government and civil services)17 18 20 (see supplementary appendix 3 for data extraction table of quantitative studies).
Study characteristics (n=79)
The remaining 74 studies provided a description of the external actors and funded activities. Over three quarters of them were published in the last decade. The majority of them focused on the African region (n=17) or globally (n=15). Public and third sector organisations were the most studied, in particular through bilateral and multilateral governmental organisations and non-governmental organisations respectively. Studies focused mostly on contributions to activities of capacity-building, service provision, and research and research capacity-building (see supplementary appendix 4 for data extraction table of qualitative and other studies). The next sections describe in details evidence on global trends in external contributions for mental disorders in LMICs from quantitative studies and on each group of external actors from all studies.
Global trends
Despite the sixfold increase in DAMH over the last two decades, in 2015 mental disorders still received a small proportion of development assistance for health (0.4%, US$132 million), accounting for less than US$1 of development assistance for health per disability-adjusted life year (ie, year of ‘healthy’ life lost) compared with, for example, US$144 for HIV/AIDS.5 A study17 that also included disbursements to non-health sectors found a similar mean annual estimate (0.7%, US$134 million), of which 48% was directed to humanitarian assistance, education and governments. Among populations at higher risk of mental disorders, as little as 13% (US$190 million) of DAMH disbursed between 2007 and 2015 targeted children and adolescents, mainly in humanitarian contexts.18 Similar estimates (17%, US$88 million) were found in another study.20 Among humanitarian assistance disbursed between 2007 and 2009, only a tiny proportion (0.1%, US$226 million) targeted programmes including mental health and psychosocial support (MHPSS).19
Public sector
Bilateral governmental organisations accounted for 18% (US$222 million) of DAMH disbursed by channel organisations between 2000 and 2015.5 They supported global mental health through programmes targeting their priority countries and areas, and including activities spanning mental health system capacity, mental health service provisions, humanitarian response, advocacy and research.
For instance, the UK’s Department for International Development (DFID) funded numerous activities including mental health policy development in Kenya,21 community-based mental health services in Nepal22 and research into primary mental healthcare across Africa and South Asia.23 The US Agency for International Development supported the integration of mental health into primary care after the 2003 conflict in Iraq24 and capacity-building and research in Zimbabwe through the US President’s Emergency Plan for AIDS Relief in collaboration with the US National Institute of Health.25 The Swedish International Development Cooperation Agency contributed to mental health reform after the war in Bosnia and Herzegovina (1992–1995), funding capacity-building and research capacity-building in mental health.26
Multilateral governmental organisations accounted for 18% (US$228 million) of DAMH disbursed by channel organisations between 2000 and 2015, over two-thirds of which was by United Nations agencies.5 They supported global mental health through normative and programmatic work, with activities linked to their missions and priorities.
For instance, the WHO developed the Mental Health Action Plan 2013–2020 and clinical guidelines for mental health treatment in non-specialised settings.27 UNICEF was the biggest contributor to DAMH for children and adolescents in the health sector between 2007 and 2014, principally through psychosocial support in child friendly spaces.20 The International Organization for Migration provided MHPSS and capacity-building activities in humanitarian and emergencies settings, such as conflicts in Nigeria and South Sudan28 and the 2010 earthquake in Haiti.29 At the regional level, the Pan American Health Organization promoted deinstitutionalisation in Latin America and the Caribbean,30 and the European Commission research and research capacity-building in Africa and South Asia.31
No evidence was found on contributions of bilateral development finance institutions (DFIs) to global mental health. Multilateral DFIs accounted for 1% (US$14 million) of DAMH disbursed by channel organisations between 2000 and 2015,5 contributing to global mental health through technical advice and programmatic work linked to their priority countries and areas. For instance, the World Bank supported the reconstruction of better mental health services after the conflict in Bosnia and Herzegovina (1992–1995)26 and research in Sri Lanka.32 At the regional level, the Inter-American Development Bank supported the evaluation of mental health services reforms in Latin America and the Caribbean along with other stakeholders.33
Private sector
Limited evidence was found on corporations and small and medium enterprises. Among transnational and multinational companies investing in healthcare in LMICs, pharmaceutical industries were the most profitable, with the top three also active in the market of psychotropic drugs: Pfizer (USA), Johnson & Johnson (USA), GlaxoSmithKline (UK).34 US’ companies were the major player in the hospital sector in LMICs.34 No evidence was found on FDIs for health insurance or health technologies (eg, Apps) except for drugs. Similarly, no evidence was found on foreign portfolio investments (FPIs) or commercial bank loans for global mental health.
Corporate social responsibility (CSR)-supported activities in global mental health were aligned to areas of expertise of the businesses or the interests of their employees. For instance, multinational alcohol corporations are increasing presence in LMICs, such as Diageo in India35 and SABMiller in South Africa.36 SABMiller partnered with the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM) to provide HIV education and counselling to heavy drinkers in South Africa.36 Other companies supported humanitarian response and reconstruction, such as Nestlé, Holcim and Sika with psychosocial support in schools after the 2008 earthquake in Sichuan, China.37
Foundations created and predominantly funded by private sector companies invested in global mental health through activities linked to the parent company or the interests of their employees, while foundations created by wealthy individuals and families were more aligned to the interests of their founders. In 2015, foundations disbursed less than US$10 million to DAMH directly to implementing organisations in LMICs, and potentially a much larger amount through other channels.5 For instance, between 2000 and 2015 Bill and Melinda Gates Foundation (BMGF) disbursed 85% (US$11 million) of DAMH through non-governmental organisations and United Nations agencies.5
Among foundations created by private sector companies, Lilly Foundation supported a global collaboration on diabetes and depression aiming to raise awareness and improving diagnosis and treatment.38 Among foundations created by wealthy individuals, BMGF funded psychosocial support for children affected by the 2010 earthquake in Haiti,17 MacArthur Foundation activities of a civil society in global mental health in collaboration with other partners39 and Wellcome Trust research and research capacity-building in LMICs.40
No evidence was available on individual households, both for donations and foreign investments to global mental health, including private FDIs and FPIs. Similarly, no evidence was available on contributions from the diaspora through remittances allocated to mental health or from the smaller group of ‘high-net-worth’ individuals.
Third sector
Third sector organisations supported and often delivered activities covering many aspects of global mental health, from advocacy to service provision, humanitarian response and research. In 2015, international non-governmental organisations disbursed US$54 million to DAMH as channel organisations.5
Among the numerous non-governmental organisations, BasicNeeds (now part of Christian Blind Mission, CBM) received funding from DFID to deliver community-based mental health services in Nepal,22 and CBM partnered with the local government to scale-up community-based mental health services in Niger.41 Carter Center42 and International Medical Corps43 provided psychosocial support and collaborated with local governments to ‘build back better’ mental health systems after the 2014–2015 Ebola outbreak in Liberia and the 2004 tsunami in Aceh (Indonesia), respectively. A large number of non-governmental organisations, including CBM, Doctors of the World, Doctors without Borders, Handicap International (now Humanity and Inclusion), members of the International Red Cross and Red Crescent Movement, and Partners in Health, delivered MHPSS activities after the 2010 earthquake in Haiti.44 Grand Challenges Canada, a non-for-profit organisation primarily funded by the government of Canada, committed US$19 million for innovations in global mental health.45
Multisector partnerships
Limited evidence was found on global health initiatives. Between 2007 and 2015, GFATM disbursed as channel organisation US$551 million to DAMH for children and adolescents, focusing on psychological support for individuals living with or at risk of contracting AIDS/HIV.18 For instance, GFATM supported services for illicit drug users in Thailand46 and physical and psychosocial support for individuals living with HIV/AIDS in sub-Saharan Africa and East Asia,47 the Global Alliance for Chronic Diseases research in global mental health.48
Discussion
This new typology illuminates the ecosystem of external actors in global mental health. This is crucial in the new landscape of the SDG-era: the plurality of actors requires good understanding of each of them, not only as single entities but also as part of a larger ecosystem. The majority of the evidence focused on the public and third sector, with almost two-thirds of DAMH disbursed to LMICs through the third sector. Evidence on the private sector and multisector partnerships is scarce or inexistent. Overall, evidence remains very limited for a number or reasons.
First, across sectors, studies have focused primarily on donors. However, many investors are already active in global health. In the public sector, DFIs’ annual commitments grew from US$10 billion in 2002 to US$70 billion in 2014,49 though healthcare attracted a small (2%–3%) share of investments,50 which could have included investments in mental healthcare. For instance, United States Overseas Private Investment Corporation invested in private healthcare businesses in sub-Saharan Africa and South Asia through healthcare funds.51 In the private sector, FDIs represent the largest (39%, US$671 billion) external source of finance in LMICs, more than three times the contributions from official development assistance and other official flows (11%),52 though the amount directed to healthcare is small53 and to mental health is unknown.
Second, none of the studies explored the role of individual households. The wealth of high-net-worth individuals amounts to over US$70 trillion and is expected to reach US$100 trillion by 2025.54 Among the members of the Giving Pledge, a group of wealthy individuals committed to donate more than a half of their wealth, Bill Gates committed US$100 million of personal investments to fight dementia.55 Moreover, over the last decade contributions from a larger group of individuals, diaspora movements, through remittances increased to US$429 billion in 2016 and are expected to grow further.56 They represent the second most important source of external financing in LMICs (24%) and are responsible for more than twice the amount of official development assistance and other official flows.52 While remittances could unlock additional resources in global mental health, examples are difficult to find.
Third, studies have focused on external actors from high-income countries. External actors from other LMICs are gaining power in global health, in particular middle-income countries. For instance, official development assistance for health from China was estimated at US$1.6 billion between 2000 and 2013, focusing predominately on health infrastructures, supplies and drugs in Africa and Asia,57 though evidence on mental health is lacking.
Fourth, comparison of financial estimates across studies requires consideration of limitations due to the use of different datasets and methodologies. Studies in this review used three datasets: the development assistance for health database (Institute for Health Metrics and Evaluation),7 the aid activities dataset from the Creditor Reporting System (Organisation for Economic Co-operation and Development),17–20 and the Financial Tracking Service (United Nations Office for the Coordination of Humanitarian Affairs).19 Estimates may vary as different datasets capture different information (eg, actors, sector of activities)58 and may employ different methodologies to identify and compute estimates from the same source.59 In particular, different methodologies influence financial estimates for programmes that tackle multiple health conditions.
Fifth, a limited number of funding instruments were used in the studies included in this review (grants, technical assistance, in-kind contributions). However, the use of both financial instruments from the private sectors and innovative financial instruments is growing in global health.60 For instance, the World Bank is currently considering issuing social purpose bonds for global mental health.61 The venture capital fund Acumen is facilitating investments in health in LMICs, such as affordable health insurance in Kenya and hospitals and emergency medical care for the lower income groups in India,62 though not yet in mental health. Investment-based crowdfunding platforms are facilitating investments in health (potentially including mental health),63 although with very limited presence in LMICs.
Sixth, allocations of funding to global mental health were often limited to geographical allocation. Only one study7 reported misalignment of disbursement relative to needs, measured as burden of mental disorders. Similarly, development assistance for health has been found to be misaligned with disease burden,64 with some conditions such as HIV/AIDS displacing other health funding priorities65 and more aid targeting conditions with more cost-effective interventions.66
Seventh, funded activities focused primarily on treatment in healthcare and humanitarian or post-conflict settings. One study22 reported on support for people with mental disorders in income-generating activities and another37 on psychosocial support in schools. However, multiple dimensions of the lives of people with mental disorders, their families and other carers are affected and effective interventions are available. Those include support for children with intellectual disabilities in schools, stress-reduction programmes in the workplace, and support for carers of people with dementia.3
Eighth, partnerships with domestic actors were numerous but often restricted only to external actors in the public and third sectors. For instance, Doctors of the World collaborated with the local government to provide and ‘build back better’ mental health services after the 2007 earthquake in Peru,67 and the Organisation of American States with the University of São Paulo to build research capacity on drugs in Latin America.68 This reflects historical tensions in the field between biomedical and social explanations of and responses to mental disorders.69 However, partnerships in global health are increasing in number and types of actors, allowing for pooling of a variety of resources and skills,70 though posing new challenges such as in relation to accountability and sustainability.
Finally, few studies uncovered by this review addressed ethical concerns, such as accountability, equity, and conflict of interests. Three studies analysed conflict of interests between corporations’ investments and CSR initiatives,36 accountability of partnerships,71 and human rights abuses in funded programmes.72 The financialisation of global health (ie, the increase in size and influence of financial institutions and markets) introduces new ethical challenges spurred by financial motives,73 such as conflicts of interest between global health foundations and food and pharmaceutical corporations,10 ‘responsible banking’ of the financial sector investing in global health,74 and equitable access to private healthcare.75 Ethical concerns in global mental health are often limited to conflict of interests in practitioners,76 while a systemic approach to ethical financing is lacking.
Limitations
This study has limitations. Systematic searches in electronic databases were only run in English between 2000 and 2018 and included only manuscripts published in peer-reviewed journals in English, French, Italian, Portuguese and Spanish. Given that the purpose of the study was to review external actors, those searches captured the main languages used for publications in high-income countries and many LMICs. The exclusion of grey literature made possible the introduction of a quality criterion in the systematic mapping. Mental health was defined to include mental disorders only, excluding positive aspects and social determinants of mental health. Finally, the exclusion of external actors not providing financial or in-kind contributions, such as political leaderships and consultative fora, might have discarded an important influencer of disbursements.
Recommendations
Mental disorders in LMICs require urgent political attention. Mental disorders account for a substantial proportion of the overall burden of poor health and high economic cost (US$0.9 trillion in 2010),77 and their impact is expected to increase further due to projected demographic and epidemiological changes and an increase in (adverse) social determinants, such as economic inequalities and natural disasters associated with climate change.2 The SDGs7 and WHO Mental Health Action Plan 2013–202078 provide an unprecedented framework for global action. Tools are available to decision makers for designing better mental health system and services, such as the Mental Health Atlas,4 as well as guidelines for mental health policy, planning and service development,79 and for interventions in non-specialised settings.80
However, the low resources allocated to mental disorders both domestically and externally hinder progress. With LMIC governments often at full capacity, external funding needs to be unlocked. The results of this review suggest a large ecosystem of external financial actors are already disbursing to global mental health, and untapped resources could be mobilised. However, drawing on this review, I suggest that the pluralism of actors requires five adaptations in order to achieve a sustainable impact.
First, a global coordination mechanism that involves all actors in global mental health should coordinate and monitor financial efforts over time, favouring partnerships and accountability. A global partnership for mental health81 has been recommended by experts for coordinating efforts, and the recently launched Countdown Global Mental Health 2030 is expected to monitor progress towards decreased disparities in mental health across countries.82 Second, collaborations across actors should be preferred to the establishment of new organisations. For instance, while a multidonor fund for non-communicable diseases and mental health has been proposed by the WHO Independent High-Level Commission on noncommunicable diseases,83 its establishment could contribute to the fragmentation of efforts in global health. Third, local ownership and sustainability should be at the centre of funding decisions: mental disorders should be included in LMIC government priorities84 with an incremental approach for increasing domestic spending and coverage,85 external funding should be aligned with those priorities, and humanitarian and development funding coordinated.86 Fourth, it is paramount to collect better data that include contributions from all external actors in global mental health to favour planning and accountability. Finally, ethical considerations should be integrated into decision-making and monitoring processes in external financing for global mental health. This could favour the establishment of partnerships across sectors while preserving core values in global mental health.
Further research is needed to understand the role of external actors in global mental health, especially outside the public sector. Qualitative studies should map external actors for mental disorders in different settings, using the grey literature and this new typology to support consistency and inform comparisons. Studies tracking external resource flows should take a comprehensive approach and go beyond DAMH to include disbursements from other external actors. Quantitative studies should assess whether external funding for global mental health are allocated effectively, efficiently and equitably. Quantitative and qualitative studies should explore what financial instruments work in global mental health, including feasibility and acceptability in different local contexts, effectiveness, cost-effectiveness, equitability, scalability and sustainability. Finally, studies that examine ethical issues related to external funding in global mental health are needed, in particular studies of the financialisation of global mental health.
Conclusion
Addressing mental disorders in the SDG-era requires mobilisation of additional external funding from multiple sources, along with an incremental increase in domestic funding. Unlocking external funding is possible, but coordination of efforts across actors is crucial, and the use of a sustainable and ethical approach is a moral imperative. This study presents opportunities to engage with a multitude of external actors in global mental health. In addition, it suggests a new typology of external actors that could provide a helpful framework for future policy planning and research on sustainable development in global mental health and global health.
Acknowledgments
The author is extremely grateful to Martin Knapp, Ernestina Coast, Clare Wenham (London School of Economics and Political Science) for reviewing previous versions of this manuscript, to Alexis Palfreyman, Jessica Ng, Laura Sochas (London School of Economics and Political Science) for advice during the systematic review process, and to Daniel Chisholm (WHO) and United for Global Mental Health for enriching discussions that have informed the study.
References
Footnotes
Handling editor Soumyadeep Bhaumik
Twitter @ValentinaIemmi
Contributors VI has conceived and designed the study, searched the literature, extracted, analysed and interpreted the results, and written the paper.
Funding The author has not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.