Article Text

Abstract
Introduction During the COVID-19 crisis, researchers had to collect data remotely. Telephone surveys and interviews can quickly gather data from a distance without heavy expense. Although interviewer-administered telephone surveys (IATS) can accommodate the needs of international public health research, the literature on their use during infectious disease outbreaks is scarce. This scoping review aimed to map the characteristics of IATS during infectious disease outbreaks.
Methods IATS conducted principally during infectious disease outbreaks and answered by informants at least 18 years old were searched from PubMed and EBSCO. There was a manual addition of relevant documents identified during an initial search. Overall trends were reported using different groupings, including WHO regions, and study details were compared before and during the COVID-19 pandemic.
Results 70 IATS published between 2003 and 2022 were identified. 57.1% were conducted during the COVID-19 pandemic. Among 30 IATS conducted before the COVID-19 pandemic in the world, only 3.3% were carried out in low-income and middle-income countries (LMICs). This percentage of studies in LMICs out of all the IATS rose to 32.5% during the pandemic. The share of qualitative studies grew from 6.7% before the COVID-19 outbreak to 32.5% during the outbreak. IATS performed during the COVID-19 pandemic focused on more diverse, specific population groups, such as patients and healthcare professionals. Mobile phones are increasingly used for IATS over time.
Conclusion IATS are used globally with high frequency in the Western Pacific Region and high-income countries. Technical and financial challenges continue to exist, and assessments of inclusiveness and representativeness should be carefully conducted. A lack of details related to methods was observed, and this scoping review urges researchers using this data collection method in the future to specify how they executed IATS for better use and more efficient deployment.
- Public Health
- Systematic review
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Telephones have been playing an important role in data collection especially when data need to be gathered quickly and remotely, and infectious disease outbreaks are a good example of such situations.
The use of online surveys is increasing globally alongside digitalisation and technological development.
However, there is little literature on interviewer-administered telephone surveys (IATS), and changes in the use, including how, when and where this data collection method has been used.
WHAT THIS STUDY ADDS
Our scoping review found that the number of IATS conducted in low- and middle-income countries during the COVID-19 pandemic (13 IATS) sharply increased from the pre-COVID-19 era (one IATS).
We learnt that IATS during the pandemic have investigated more specific and diverse population groups than in the prepandemic period.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The increased usage of cell phones to operate IATS aligns with the growing mobile phone ownership, thanks to which the global mobilisation of this remote survey mode might be accelerated in the future.
We observed inadequate information on study details, including the number of languages spoken by interviewers as well as technologies and techniques to improve and optimise the administration of IATS.
We encourage sharing techniques and knowledge among researchers whereby IATS could be further improved and contribute to more inclusive public health research.
Introduction
Remote data collection is particularly relevant during infectious disease outbreaks when traditional face-to-face modalities are inappropriate. Although it is rare to witness infectious disease outbreaks requiring lockdowns and restrictions on movement, infectious disease outbreaks occur more frequently than in the last century1 2 despite better sanitation and improved healthcare access and quality. The COVID-19 crisis is a great example, during which researchers were obliged to collect data remotely given physical distancing, lockdowns and travel restrictions to contain the virus. Likewise, in the context of natural disasters and conflicts, and for convenience, it is likely that remote data collection methods will continue to be widely used.
There are various ways to gather data remotely. Alongside the wide use of online data collection modes like web-based questionnaires, it seems that phone surveys and interviews continue to play an important role. While both smartphone ownership and also (stable) access to the internet is taken for granted in some countries, the telephone without internet access often remains to be a vital communication tool in resource-scarce settings.3 The existing literature addresses phone-based data collection,4 5 but often focuses only on specific countries or regions rather than the entire world. In other words, there is limited understanding of the use of phones to remotely collect data in different parts of the world. Combined with the recent rise of infectious disease outbreaks worldwide, it appears to be worth examining the use of telephone surveys under epidemic and pandemic conditions.
Among several tools to remotely collect data, telephones are especially useful for quickly gathering both qualitative and quantitative data from a distance without heavy expense.6 7 This modality tends to have higher response rates than postal and electronic surveys too.8 Phone surveys are also effective to study ‘the temporality and social context’ in which questions are asked and responded to; when administering phone-based surveys, researchers can make use of computers to record responses, which can be continuously monitored, thereby quality control is also managed.9 In contrast to surveys and questionnaires which are often very structured, respondents, while being usually allowed to talk freely, can provide more nuanced information during interviews. In addition, unlike other remote data collection modes, in-depth interviews allow investigators to develop rapport and build trust.10 Good interviewers can also ask detailed, complex questions which require clarification,5 and this aspect is practical for quantitative research which requires accuracy. Notwithstanding the utility, there is limited knowledge of how researchers make use of the telephone and what kind of research questions they aim to scrutinise with phone surveys and interviews.
Surveys and interviews involving interaction between live interviewers and informants (hereinafter interviewer-administered telephone surveys, IATS) over landlines and cellphones (therefore excluding calls using applications as well as internet-based or video calls) can accommodate the specific needs of international public health research. In many cases, high-income countries (HICs) fund and carry out studies in low-middle-income countries (LMICs), which are more vulnerable and exposed to infectious diseases.11 When surveyed or interviewed by researchers from HICs, informants from resource-scarce nations may feel vulnerable due to poverty, widespread illiteracy and linguistic barriers,12 given the linguistic diversity in these countries.13
Despite the usefulness of IATS during infectious disease outbreaks, the literature on this subject is scarce. It is unclear in what context and how this remote data collection method is used in the time of infectious disease outbreaks. This scoping review aimed to identify and map characteristics of IATS responded to by informants of at least 18 years old during infectious disease outbreaks.
Methods
While a systematic review often addresses a precise question, a scoping review aims to investigate the way research is conducted on a specific subject as well as to identify characteristics of studies.14 The objective of this research is in line with the purpose of a scoping review, and therefore this type of review was considered appropriate.
Reflexivity statement
This scoping review intended to produce a global picture illustrating how IATS have been used. SA was a paid master of public health intern at CloudlyYours, a for-profit business specialising in digitalisation, including technological support for telephone surveys, as well as the French National Research Institute for Sustainable Development, a French public research institution. These institutions have collaborated on some projects, including phone surveys in Africa.15 MFB, ZT, EB, AF and VR have worked together and used IATS. To improve operation of IATS and gain updated information as well as insights, SA was assigned the task of researching phone surveys. Although SA principally formulated the protocol and performed data searches to conduct this scoping review efficiently, MFB, ZT, EB, AF and VR contributed to the screening and selection of documents as well as analysis. By working remotely, the authors from HICs and LMICs were given opportunities to give feedback and exchange insights. MFB, AF and VR are living in Senegal. There were one female and one male early career researchers, who took the lead in the scoping review. Given the diversity of the authors’ backgrounds, this scoping review, a product of an international collaboration, can provide insightful ideas for future research and particularly methods in need of sufficient attention and consideration in global health.
Patient and public involvement
No patients were involved.
Protocol and registration
The final version of the protocol16 was made available on 17 June 2022 online (www.protocols.io/).
Eligibility criteria
Following the Joanna Briggs Institute (JBI) Manual for Evidence Synthesis for scoping reviews,17 the PCC (Population/Participants, Concept, Context) framework was used to identify eligibility criteria. This review included telephone surveys distributed to and responded to by adults, anyone at least 18 years old (Population/Participants).
Because this research aimed to capture global characteristics and trends of IATS rather than specific sociodemographic factors, sex or gender information was not extracted. Telephone surveys, including both landline and mobile phones, were included. This review was limited to studies that relied on the single method of IATS, and those using other data collection modes together with IATS were excluded. There are different approaches to address technical and financial challenges, and some researchers have used different technologies and techniques to optimise as well as enhance the operation of IATS. For example, a common technique is computer-assisted telephone interviewing (CATI), which was considered a type of IATS and therefore included in this scoping review. CATI signifies any computer-supported feature of telephone interviews, both hardware, and software, which can be a sole part or combined components.18 IATS are often accompanied by other techniques such as a reactive auto dialer (RAD), random-digit dialling (RDD) and short message service (SMS). RAD allows automatic and optimised calls.19 RDD is a form of probability sampling by randomly choosing phone numbers.18 SMS can be used to contact potential informants.19–23 These innovations are particularly practical for reducing the burdens of interviewers who otherwise would need to dial manually and record answers by hand and minimising human errors. IATS using these techniques were included in this scoping review (Concept).
This scoping review included the telephone surveys whose data were collected during infectious disease outbreaks, epidemics and pandemics regardless of scale or severity. No criteria were set to focus on outbreaks associated with large-scale movement restrictions. Furthermore, to be included in this scoping review, topics or objectives of the IATS did not need to be related to infectious diseases. This is because this review aimed to understand what kind of subjects researchers attempt to explore while using IATS (Context).
Information sources and search
SA conducted an initial limited search of MEDLINE and found the text words in relevant articles as well as Medical Subject Headings (MeSH) terms. Using these words, SA drafted and refined the search strategy in accordance with feedback from a librarian, who suggested two databases, as well as MFB, ZT, EB, AF and VR. Based on the feedback, SA modified the search strategy, which was agreed by all authors, and performed database searches in PubMed and EBSCO on 5 April 2022 without restrictions on language or publication date. To allow the searches to be widest possible, terms like ‘infectious disease’ were used instead of specific illnesses. The following combination was used for the both database searches: (((‘telephone*’ OR ‘cellular phone*’ OR ‘phone*’ OR ‘cell phone*’ OR ‘mobile phone*’ OR ‘mobile telephone*’) AND (‘survey*’ OR ‘interview*’ OR ‘cross-sectional survey*’ OR ‘longitudinal survey*’)) OR (‘interviewer-administered survey*’ OR ‘interviewer administered survey*’ OR ‘computer-assisted telephone interviewing’ OR ‘computer assisted telephone interviewing’)) AND ((‘outbreak*’ OR ‘epidemic*’ OR ‘pandemic*’) AND (‘infectious disease*’ OR ‘communicable chronic disease*’ OR ‘communicable infectious disease*’ OR ‘infectious illness’ OR ‘infectious virus*’)).
Additional documents consulted during an initial search before the protocol development were also added as potentially relevant studies. A protocol was developed by SA and agreed by MFB, ZT, EB, AF and VR.
Selection of sources of evidence
SA and MFB independently screened the potentially relevant documents using a web-based platform, Covidence (www.covidence.org/). Duplicates were removed automatically. Due to the reviewers’ language proficiency, studies were excluded if not written in English, French, Spanish or Japanese. Any disagreements were resolved by discussions.
Data charting process and items
Using Microsoft Excel V.16.61.1, SA drafted a data extraction form. This form was reviewed by all authors and continuously updated as needed. Data were extracted by SA, which was later reviewed and verified by MFB, ZT, EB, AF and VR. Information extracted from each study includes general information and study details, and a full list of the extracted items can be found in table 1. The included studies were sorted in alphabetical order by the corresponding author’s last name.
List of items extracted from included studies
Critical appraisal of individual sources of evidence
Unlike systematic reviews, scoping reviews do not require a critical appraisal or risk of bias assessment.17 24 We appraised neither methodological quality nor risk of bias of the included studies. The quality or the ratings were not presented. However, the MMAT V.201825 was employed as a set of standards to determine the study design of each included article.
Synthesis of results
The reporting of this scoping review follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Review guidelines.24 Considering that the prevalence of infectious diseases varies in different countries and regions, the included IATS were grouped geographically (WHO region) for descriptive analyses. Furthermore, given that LMICs are more likely to be exposed to infectious diseases and study sites than HICs, a financial grouping (World Bank income classification) was also used to detect trends in the use of telephone surveys. RStudio V.4.2.1 was used for the descriptive analyses.
Results
Selection of sources of evidence
A total of 526 records were retrieved via database searches, and four documents were added as supplemental studies. After removing duplicates, 420 potential studies were screened by title and abstract. Of these, 146 were screened by full text, and 70 were included in the analysis. Of these, 66 studies were identified via database searches, and four were manually added. There were four reasons for exclusion; 46 studies were excluded because data collection methods in addition to or other than IATS were used, or because the telephone was not clearly stated as a data collection tool (wrong data collection method); 20 studies were excluded because the data were not collected during an infectious disease outbreak (wrong period) although studies in which the data collection started during an infectious outbreak and ended a few months after the end of the outbreak were considered acceptable and included; 12 studies were excluded because people aged 17 or younger were interrogated by interviewers, or because age is not mentioned in the inclusion/exclusion criteria (wrong population). Studies in which parents or caregivers at least 18 years old participated on behalf of their children were included; two studies were excluded because the content is not written in English, French, Spanish or Japanese (wrong language). Despite this linguistic criterion, no study in French, Spanish or Japanese met the rest of the selection criteria, and all the included studies are written in English. The screening process can be found in figure 1.
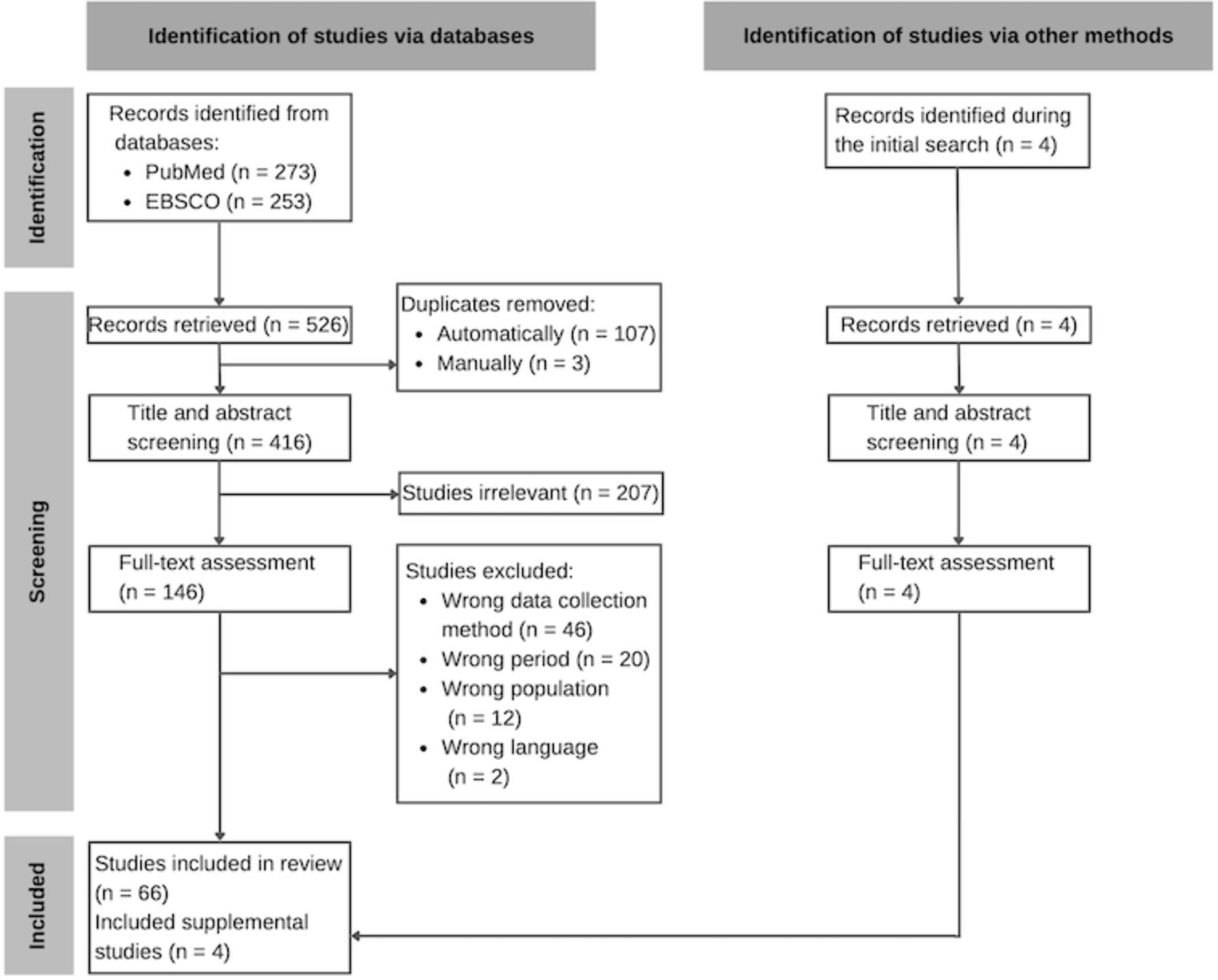
Screening process.
Characteristics of sources of evidence
This scoping review included 70 IATS published between 2003 and 2022 from all over the world. The included studies were performed during the following infectious disease outbreaks: Chikungunya, COVID-19, Dengue, Ebola, H1N1, H5N1, H7H9, SARS, Seasonal influenza and Zika. There was an upsurge in the number of IATS published during the COVID-19 pandemic. In addition, another increase was observed between 2009 and 2011. Between these years of the H1N1 influenza pandemic, 13 IATS (seven in China, four in Malaysia and two in the USA) were performed.
Results of individual sources of evidence
A full list of all the included studies in this scoping review can be found in online supplemental materials 1 and 2.
Supplemental material
Synthesis of results
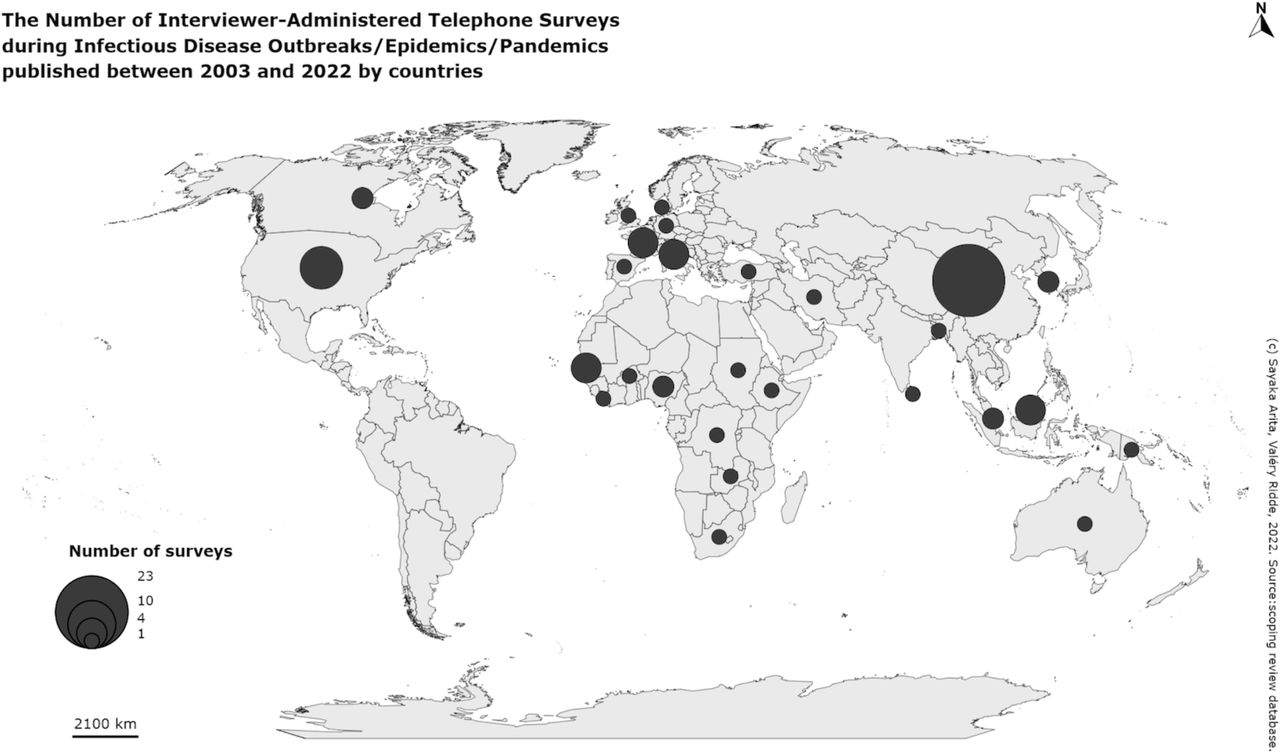
Seventy IATS were found in all the six WHO regions as seen in figure 2; 33 IATS (47.1%) were found in the Western Pacific Region (WPRO), 13 (18.6%) in the European Region (EURO), 10 (14.3%) in the Region of the Americas (AMRO), 10 (14.3%) in the African Region (AFRO), two (2.9%) in the Eastern Mediterranean Region (EMRO) and two (2.9%) in the South-East Asia Region (SEARO).
{kind=link}
{kind=link}
Number of IATS during infectious disease outbreaks/epidemics/pandemics published between 2003 and 2022 by country.
Among the 70 IATS, 27 (38.6%) were found in HICs, 29 (41.4%) in upper-middle income countries, 10 (14.3%) in lower-middle income countries and three (4.3%) in low-income countries. In addition, there was one international IATS (1.4%) performed in low and lower-middle income countries (Burkina Faso, Ethiopia and Nigeria). These income groups were further merged and simplified. When high and upper-middle income countries were combined as HICs, and low and lower-middle income countries were put together as LMICs, 56 (80.0%) IATS were found in HICs and 14 (20.0%) in LMICs.
Among the 70 IATS, the smallest sample size was 11,26 and the largest was 31 332.27 There were 35 quantitative descriptive studies (50.0%), 16 quantitative non-randomised studies (22.9%), 15 qualitative studies (21.4%), three mixed-methods studies (4.3%) and one quantitative randomised controlled trial (1.4%). In terms of the scale, 35 IATS were at the local level (50.0%), 22 regional (31.4%), 12 national (17.1%) and one international (1.4%).
Among all the included IATS, adult individuals were the most surveyed population with 34 studies (48.6%). There were 10 IATS targeting patients (14.3%), seven healthcare professionals (HCPs, 10.0%), seven households (10.0%) and 12 other groups (17.1%). Although 35 IATS did not specify the phone type (50.0%), 21 IATS relied on landlines (30.0%); 11 IATS used mobile phones (15.7%) and three studies used fixed and cell phones at the ratio of 1 to 1 (4.3%).
Of 70 IATS, 40 (57.1%) were carried out during the COVID-19 pandemic, one of which was conducted in the Democratic Republic of the Congo where an outbreak of Ebola was also declared.28 There were 30 IATS which took place before the COVID-19 pandemic, and 17 were realised during the H1N1 pandemic, one of which compared social-cognitive factors on personal hygiene practices between the H1N1 and H5N1 outbreaks in Hong Kong.29 All the infectious diseases during which the included IATS were carried out are listed in table 2.
Number of IATS by infectious disease; N (%)
The use of IATS greatly increased during the COVID-19 pandemic, and some characteristics changed since the prepandemic period as seen in table 3. For example, there were no IATS conducted in EMRO and SEARO before the COVID-19 pandemic. However, during the pandemic, this remote data collection method was mobilised in all WHO regions. WPRO remains the region where this method has been most frequently used. Furthermore, the share of IATS in LMICs among all the IATS rose from 3.3% before the COVID-19 pandemic to 32.5% during the pandemic. The composition of phone types transformed too. While 66.7% of all prepandemic IATS relied on fixed phones, the share of landline IATS shrank to 2.5% during the COVID-19 outbreak. On the contrary, the percentage of mobile IATS among all the IATS increased from 3.3% before the COVID-19 outbreak to 25.0% during the outbreak.
Characteristics of IATS before and during COVID-19 pandemic
There were other aspects that altered during the global outbreak of COVID-19. The range of sample sizes widened. The share of qualitative studies grew from 6.7% to 32.5%. While local IATS continue to be the dominant study scale both pre-COVID-19 and during the COVID-19 pandemic periods (56.7% and 45.0%, respectively), the share of national IATS expanded from 6.7% to 25.0%, respectively. In terms of the population, before the pandemic, 70.0% of the IATS targeted adult individuals. However, during the pandemic, IATS focused on more diverse, specific population groups, such as patients (25.0%) and HCPs (17.5%), who were not surveyed before the pandemic. The share of IATS concerning adult individuals decreased to 32.5% in the time of COVID-19.
Regarding the objectives of the included IATS, there were some commonalities. The most common theme was vaccines, and this topic was studied in seven IATS. Four20 30–32 of these IATS were carried out during the COVID-19 pandemic; two33 34 during the H1N1 pandemic and one35 during a seasonal influenza outbreak. Mental health and psychological effects were also seen across some infectious disease outbreaks. Anxiety was examined in three IATS: during the H1N1,36 H7N937 and COVID-1938 pandemics. Psychological responses were assessed in three IATS: during the H1N139 40 and COVID-1941 outbreaks. There was one study that addressed psychological distress during the COVID-19 pandemic,42 and another study examined fear and psychosocial impact during the H1N1 influenza outbreak.43 Similarly, there was one study44 investigating mental health in the time of COVID-19. Furthermore, many studies concerned specific behaviours. Three IATS discuss protective behaviours: one during a Dengue outbreak45 and two during the H1N1 pandemic.46 47 Preventive behaviours were examined in six IATS: one during the COVID-19 pandemic,48 three during the H1N1 influenza pandemic,33 36 49 one during a Zika outbreak50 and one during the SARS outbreak.51 Avoidance behaviours appeared in three IATS: one in the time of COVID-19 pandemic,27 one under the presence of the H7N9 virus37 and one during the H1N1 pandemic.39 Precautionary behaviours were addressed in one study during the COVID-19 pandemic42 and another during the H1N1 outbreak.52 Likewise, one study assessed both protective and also avoidance behaviours under the H1N1 outbreak.43
Discussion
The findings demonstrated that IATS have been carried out around the world with greater frequency in WPRO. Although having been mobilised in restricted regions before the COVID-19 pandemic, this remote data collection method was used more globally amid the pandemic. This phenomenon corresponds to the fact that COVID-19 was spread and studied internationally, whereas other infectious diseases were more local and regional. The expanded usage of cell phones to administer IATS during the COVID-19 outbreak accords with the recent technological advancement particularly in LMICs. Thus, the technological development might have led to the wider use of IATS amid the COVID-19 pandemic to some degree. The same number of IATS performed in AFRO and EURO during the worldwide COVID-19 outbreak appears to hint at the suitability of this remote data collection method during infectious disease outbreaks regardless of the geographical location or income level. It is possible that a further expansion of network coverage and affordability of mobile phones, thanks to which cell phone ownership is increasing in LMICs,4 will accelerate the global mobilisation of IATS in the future.
On the other hand, before the COVID-19 outbreak, a lot fewer IATS have been carried out in LMICs even though these countries are more affected and exposed to infectious diseases. The less frequent use of IATS prior to the COVID-19 pandemic, despite the higher prevalence of other infectious diseases,11 might indicate that public health research in LMICs is not sufficient. Or, other data collection modalities were preferred and considered appropriate in LMICs before the COVID-19 outbreak. As discussed earlier, it seems that the rapid growth of mobile phone ownership contributes to spurring the wider use of IATS globally. However, phone ownership is not universal, and technical and financial obstacles continue to exist. Hence, sharing of techniques and knowledge is encouraged to ameliorate IATS in resource-scarce settings, like LMICs, especially given the lack of information on techniques, such as RAD, RDD and SMS, unique to telephone surveys among the included studies.
Knowledge sharing also seems practical for strategising and running IATS in a novel, complex circumstance, notably in LMICs where there are individuals with several cell phone subscriptions.13 53 The new situation regarding phone ownership4 makes it difficult to accurately estimate the degree of representativeness and the characteristics of (non-)respondents too. As seen in the included IATS, demographic information is essential when understanding and interpreting the results. Furthermore, socioeconomic factors often help more accurately comprehend the survey answers. Nonetheless, it is not always easy to obtain and verify socioeconomic variables in LMICs. When relatively recent, reliable data, like censuses, are not accessible as a reference, researchers might need to consider narrowing down the target population, rather than trying to achieve a nationally representative sample of the general public. Having a narrower target population is likely to enable researchers to estimate the representativeness of their samples more accurately, thereby the reliability of their data would also be ensured. Representativeness is particularly important for quantitative descriptive studies, the most prevalent study design among the 70 included studies, to perform statistical analyses. Various established sampling methods to acquire large, representative samples for IATS already exist,54 and these methods should be applied to achieve better representativeness.
Researchers should also pay attention to inclusiveness. As highlighted in some studies, it is important to consider which groups of people are included in and excluded from telephone surveys. Whereas some argue that mobile phones can be useful to communicate with harder-to-reach subgroups,13 others assert that the most marginalised, including those without a stable signal or any form of telephone, are often excluded from research.30 55 56 There are several methods to make research more inclusive. For instance, thanks to the low price of phones, when investigating or attempting to include the most disadvantaged or people without telephones in rural areas, researchers can distribute affordable cell phones to the selected respondents5 although this solution requires ethical, technical and financial consideration. Another solution to avoid participants’ financial burdens, especially when targeting the disadvantaged, is using toll-free numbers or offering financial compensation. Adequate consideration for questions themselves is also the key to good IATS. For instance, characteristics of the questions, such as their form or difficulty, influence item non-response to some extent.57 The use of simple, easy words should be used, especially when interviewing or surveying the vulnerable.
Understanding and accommodating local needs is vital to more inclusive research and efficient deployment of IATS too. As many IATS were at the local level, it is also important to acknowledge the context specific to the study site. To do so, it is crucial to include local staff and experts, who both reinforce localised knowledge helpful to plan surveys and better comprehend the results and also communicate with informants. Recruitment of multilingual locals and training of interviewers can facilitate building rapport and trust between operators and informants. Among the included studies, the biggest number of languages spoken by interviewers was six in three studies in Senegal.20 21 30 Coupled with cultural and linguistic appreciation and proficiency, compared with paper-based or self-administered surveys, more personal and direct communication between interviewers and informants in IATS can contribute to minimising miscommunication and misunderstanding. To answer phone surveys, respondents do not need to be literate or have internet access. IATS also allow probing and clarification. These are strengths of this data collection method when gathering data and studying public health topics in LMICs under pandemic or epidemic conditions. However, most of the included studies lacked sufficient information on languages spoken by interviewers. More information on consideration and arrangements for IATS in LMICs needs to be exchanged among researchers.
In terms of topics, vaccine hesitancy and mental health, important aspects of public health, were found in some infectious disease outbreaks. These themes might be seen as sensitive and therefore hard to discuss face-to-face for certain people. Anonymity, thanks to which respondents might be more willing to provide sensitive information,9 is also an advantage of IATS. Thus, it is possible that IATS, even though not always voluntarily chosen under the presence of infectious diseases, work well to study certain topics. Furthermore, probing and clarification are particularly practical for in-depth, qualitative research. At the same time, when conducting IATS for qualitative research, it should also be remembered that keeping surveys or interviews short (no longer than about 20–30 min)5 58 can contribute to minimising informants’ fatigue.7 Qualitative research tends to involve lengthy interviews, but researchers can consider having some short sessions rather than a long single session. In some of the 15 qualitative studies identified in this scoping review, the length of each session was prone to be long (over 40 min).59–63 Besides, behaviours are commonly examined by IATS during different infectious disease outbreaks, and this indicates the suitability of this remote data collection method in research when quick data collection is required or when the context in which such research is done is important (for instance, in the context of public health crises). However, researchers should be aware of bias due to self-reporting and careful when setting study objectives and formulating survey questions.
Another noteworthy finding is the significant change in the target population, patients and HCPs in particular. The shift during the COVID-19 pandemic seems to correspond to the change in the focus of IATS. For example, there was an acute interest in HCPs and healthcare systems affected by the COVID-19 crisis, which has upset and revealed the existing fragile health sector all over the world.64 It has been reported that HCPs have experienced a variety of challenges, such as lack of preparation, protocol, information, preventive equipment, in addition to ‘stress, anxiety, fear, helplessness, hopelessness, anger, and stigma’,65 and these aspects characterise the COVID-19 pandemic as distinct from other infectious disease periods. This scoping review seems to have grasped the particulars during the most recent public health emergency. Moreover, this change in the target population from the general public to more specific groups of people appears to imply that IATS are useful to understand both epidemiological or quantitative aspects of infectious diseases, like incidence, prevalence and mortality, and also other dimensions of public health or qualitative topics, including personal experiences and mental health.
Limitations
To make this scoping review feasible, studies using multiple or hybrid data collection methods like online questionnaires and meetings in addition to interviewer-administered surveys were excluded although these methods are becoming ubiquitous. Furthermore, only two databases were searched, and all the included studies were published in English. Moreover, unpublished studies were not included due to the limited time and resources to conduct this scoping review. By omitting unpublished work, this scoping review aimed to examine and compare the included IATS consistently and systematically. The inclusion of unpublished literature might have led to more nuanced results and analysis. Finally, non-MeSH terms were omitted when developing the search strategy. The use of non-MeSH terms might have resulted in a wider range of IATS as each database uses a distinct indexing system with a different thesaurus. Consequently, if other databases or thesauruses had been used, this scoping review could have produced different results. Nonetheless, this scoping review examined as many as 70 IATS, and the search strategy was validated by a librarian.
Conclusion
The included studies demonstrated several changes in the use of IATS during the COVID-19 pandemic. For instance, IATS were concentrated in WPRO, EURO and HICs before the COVID-19 pandemic, but the use of this data collection method increased and spread to more countries, particularly in AFRO and LMICs, during the COVID-19 pandemic. Other interesting changes observed include the more diverse target population as well as the increase of qualitative and national studies. These findings seem to indicate that IATS are useful during infectious disease outbreaks regardless of the geographical location or income level.
On the other hand, we believe that this data collection modality can be further improved if researchers share more techniques and knowledge by detailing their methods when publishing their studies. We recognised the upsurge of IATS during the COVID-19 outbreak, notably in LMICs. Together with the complexity and expansion of mobile phone ownership, researchers who intend to do phone surveys and interviews in resource-scarce settings need to prepare and strategise their studies carefully. Special consideration for the hard-to-reach groups and the most disadvantaged is necessary too.
For future public health research to be more inclusive and representative, it is important to understand and accommodate local needs, such as linguistic and cultural diversity, by recruiting experts or operators who know the context specific to the study site, for example. Moreover, like other data collection modes, researchers should try to mitigate any financial burden and distress incurred by IATS. The large number of telephone surveys nowadays can cause pressure on respondents. This pressure might further lead to more informants’ refusal to participate in IATS. Moreover, questions should be carefully formulated and structured so that higher response rates can be achieved. It will be interesting to see the trend in response rates in future research.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not required.
Acknowledgments
This research is a scoping review concerning the existing literature. Therefore, no patients or human subjects were involved in this research, and it was not necessary to obtain any approval from the ethics committee. We would like to thank Lola Traverson for her insightful comments and suggestions that we received while drafting a protocol. We would also like to recognise the assistance of Flore-Apolline Roy, who created the world map demonstrating where interviewer-administered telephone surveys have been conducted.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @sayaka_arita, @mavalo76, @ValeryRidde
Contributors SA principally conceived and designed the protocol in consultation with ZT and VR. SA performed data searches to collect relevent documents, which were screened and selected by SA and MFB. SA worked on most of the presentation, analyses and interpretation of the results with support from VR. SA took the lead in drafting the manuscript. MFB, ZT, EB, AF and VR provided critical feedback and helped shape the manuscript.
Funding As required to complete the Master of Public Health program at l’École des Hautes Études en Santé Publique, SA worked as a paid intern at CloudlyYours and the French National Research Institute for Sustainable Development and conducted this scoping review.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests CloudlyYours is a for-profit business, which provides data management solutions, including technological support for telephone surveys, with its expertise in digital transformation and development. SA, as a paid master of public health intern, conducted this scoping review with other authors to produce insights into telephone-based surveys, which CloudlyYours could use to determine areas of improvement. Therefore, the theme of this scoping review aligns with one type of service that CoudlyYours provides, telephone surveys.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.