Article Text

Abstract
Following the first COVID-19 case in Chiapas, Mexico in March 2020, the non-governmental organisation Compañeros En Salud (CES) and the state’s Ministry of Health (MOH) decided to join forces to respond to the global pandemic. The collaboration was built over 8 years of partnership to bring healthcare to underserved populations in the Sierra Madre region. The response consisted of a comprehensive SARS-CoV-2 infection prevention and control programme, which included prevention through communication campaigns to combat misinformation and stigma related to COVID-19, contact tracing of suspected and confirmed COVID-19 cases and their contacts, outpatient and inpatient care for patients with respiratory symptoms, and CES–MOH collaboration on anti-COVID-19 immunisation campaigns. In this article, we describe these interventions and their principal outcomes, as well as reflect on notable pitfalls identified during the collaboration, and we suggest a series of recommendations to prevent and mitigate their occurrence. As with many cities and towns across the globe, the poor preparedness of the local health system for a pandemic and pandemic response led to the collapse of the medical supply chain, the saturation of public medical facilities and the exhaustion of healthcare personnel, which had to be overcome through adaptation, collaboration and innovation. For our programme in particular, the lack of a formal definition of roles and clear lines of communication between CES and the MOH; thoughtful planning, monitoring and evaluation and active engagement of the communities served in the design and implementation of health interventions affected the outcomes of our efforts.
- COVID-19
- health systems
- public health
- prevention strategies
- descriptive study
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
SUMMARY BOX
The COVID-19 pandemic has highlighted the importance of developing collaborative strategies between governments and civil society to respond to health emergencies. However, little literature has thoughtfully described and reflected on these collaborative interventions, especially in low-resource settings.
In this study, we present the implementation and evolution of a comprehensive and equity-promoting collaborative SARS-CoV-2 infection prevention and control programme between the Chiapas Ministry of Health and the non-governmental organisation Compañeros En Salud in rural Mexico, including its outcomes and valuable lessons learnt from both stakeholders.
Sharing the successes and challenges faced by a civil society–government partnership in a low-resource setting can stimulate other stakeholders to develop similar collaborations, setting a precedent that can strengthen the preparedness of health systems for future disease outbreaks.
Introduction
During the COVID-19 pandemic, among the most affected countries in Latin America was Mexico, with over 260 deaths per 100 000 inhabitants in early February 2023,1 in part as a result of its unstable health system when the pandemic hit the country.2 Due to significant economic inequality among states (table 1), the impact of the pandemic varied greatly among regions, leaving poorer states such as Chiapas particularly vulnerable. Public hospitals in the region suffered an exacerbation of the pre-existing shortage of health professionals,3 medical supplies4 and beds.5
Characteristics of the population served by the joint programme for prevention and control of SARS-CoV-2 infection of Compañeros En Salud and the Chiapas Ministry of Health vs state and Mexico City comparison groups
With most of the public health system’s scarce resources concentrated in urban areas of Chiapas,6 the underserved populations living in rural areas of the state were left without sufficient support. In response to this, Partners In Health Mexico/Compañeros En Salud (CES) decided to join forces with the Chiapas Ministry of Health (MOH) to design, develop and implement a SARS-CoV-2 infection prevention and control (SIPC) programme in nine rural communities and one semiurban locality (figure 1). Although all beneficiary populations were and are affected by an adverse socioeconomic context, the programme’s interventions were designed and implemented with priority given to isolated rural communities with the lowest levels of educational attainment, economic opportunity and the poorest housing conditions (table 1).

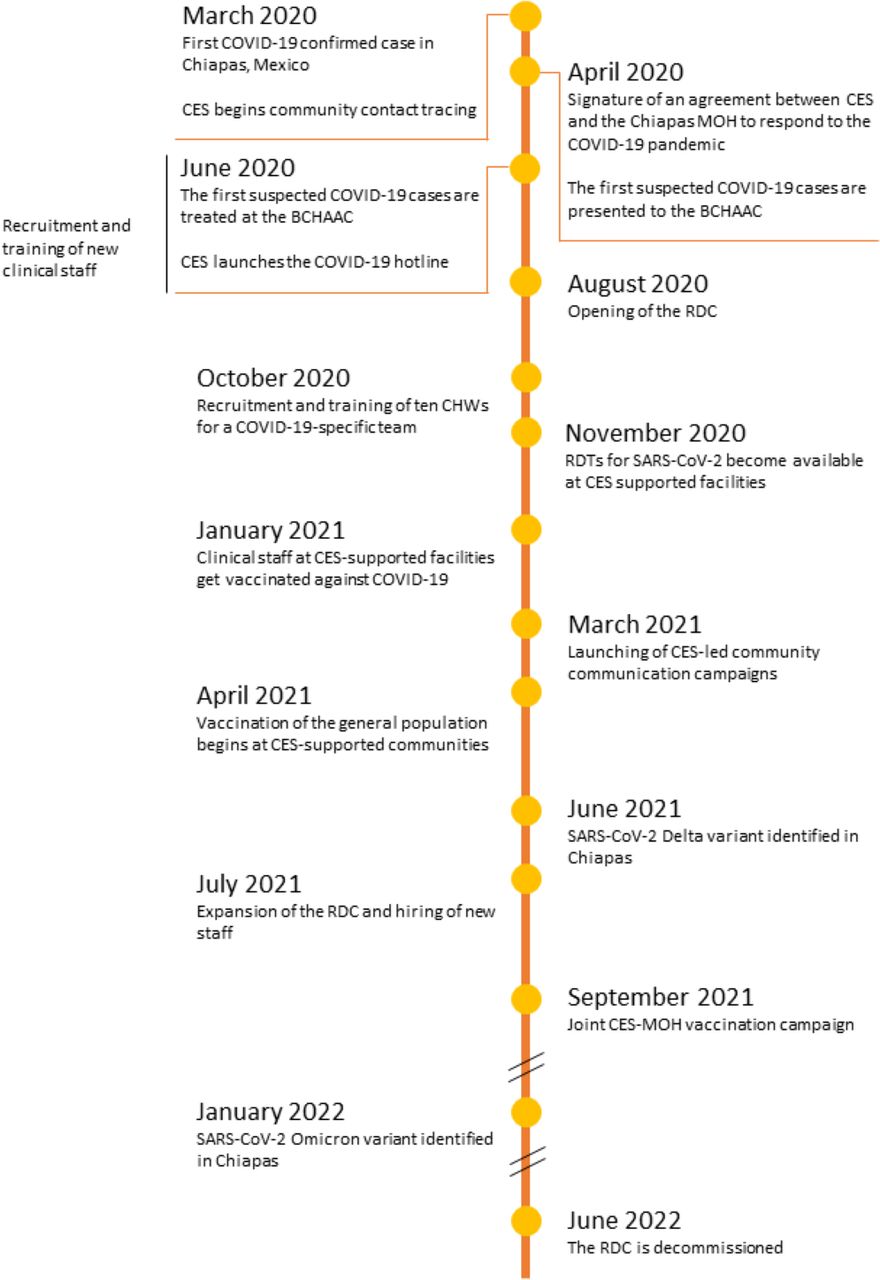
Chronology of the collaborative response to the COVID-19 pandemic between Compañeros En Salud and the Chiapas Ministry of Health. Data on the evolution of the COVID-19 pandemic in Chiapas were retrieved from the Chiapas Ministry of Health website (https://saludchiapas.gob.mx/). BCHAAC, Basic Community Hospital at Angel Albino Corzo; CES, Companeros En Salud; CHW, community health worker; MOH, Chiapas Ministry of Health; RDC, respiratory disease clinic; ROT, rapid diagnostic test.
The key role played by civil society during the COVID-19 pandemic,7–9 as well as the experience of states partnering with civil society to achieve more effective and human rights-focused responses have been reported.10–12 However, literature on the implementation, outcomes and insights of public–civil collaborative efforts to respond to the pandemic is still limited. This article aims to fill that knowledge gap by describing the experience of the CES–MOH partnership during the first 2 years of the COVID-19 pandemic in Chiapas, in which a health equity promotion approach was used,13 basing interventions on personal agency in health-related decisions and fair access to healthcare resources of the most underserved populations.
The Compañeros En Salud–Chiapas Ministry of Health joint SARS-CoV-2 infection prevention and control programme
The activities of CES span 10 outpatient clinics in nine rural communities, a Basic Community Hospital (BCHAAC) in the town of Ángel Albino Corzo, and an adjacent birthing centre and respiratory disease clinic (RDC) (figure 2). CES collaborates closely with the MOH (which manages the BCHAAC, the adjacent facilities and nine of the outpatient clinics) and with the Mexican Institute of Social Security (which manages one of the outpatient clinics). Both health institutions provide some staff, medical equipment and supplies that are supplemented by CES resources. The joint SIPC plan focused on preserving vital services and identifying COVID-19 cases utilising Partners In Health’s ‘Five essential elements for strengthening health systems’ approach: staff (qualified staff in sufficient quantity to respond to need), stuff (ensuring the tools and resources needed for care delivery and administration), space (appropriate spaces with capacity to serve patients), systems (leadership and governance, information and financing) and social support (providing basic necessities and resources needed to ensure effective care). ‘Systems’ was a key element in all the programme interventions (table 2), especially from a governance and leadership perspective. Local stakeholders were involved in the decision-making process and both CES and MOH staff participated in all phases of the programme. Detailed descriptions of the interventions are provided below.

{kind=link}
{kind=link}
Facilities supported by Compañeros En Salud in Chiapas, Mexico. *All facilities belong to the Ministry of Health of Chiapas with the exception of the Capitan Luis A Vidal rural outpatient clinic, which belongs to the Mexican Institute of Social Security.
Main implementation sites and interventions resulting from the collaboration between Compañeros En Salud and the Chiapas Ministry of Health in Chiapas, Mexico
Healthcare in rural outpatient clinics
In order to maintain our standard of care, nurses, health auxiliaries, hygienists and community health workers were hired and—along with physicians—trained in infection prevention and control measures, case identification and contact tracing, both clinical and psychosocial follow-up and referral criteria. Nurses and physicians were also trained in lung point-of-care ultrasound. At the same time, personal protective equipment (PPE), cleaning and disinfection supplies, oxygen, antigen tests and essential medicines were provided.
Adapting our clinical space was a main part of the response, triage areas and isolation zones for suspected cases were created both in waiting rooms and clinical facilities. Also, the provision of safe water, sanitisation services and garbage disposal systems were enhanced in all CES-supported outpatient clinics.
In addition, existing systems benefited from the development of remote training, epidemiological surveillance, improvement of the electronic supply chain record and warehousing system to prevent stock-outs, improved internet accessibility, enhanced referral of patients by health personal from the rural clinics to the BCHAAC and counter-referral from the BCHAAC, and the creation of social support schemes for respiratory patients. Social support included a food pantry with rice, oil, beans, soybeans, oatmeal and tuna for all family members during isolation; and a hygiene kit with gloves, chloride wipes, bleach solution, sanitising gel and soap. This social support was supplied to those families below a pre-established socioeconomic status threshold, and was maintained until the primary provider of income in the family could return to work.
Finally, formal and informal community collaborations were bolstered to reinforce existing community support networks and preserve stakeholder engagement.
Since the pandemic was declared in Mexico until June 2022, 1112 COVID-19 suspected and confirmed cases were attended and 2572 close contacts were identified in the 10 outpatient clinics supported by CES (total implementation site population=7608) (table 3).
Evolution of main output indicators of the collaborative response to the COVID-19 pandemic between Compañeros En Salud and the Chiapas Ministry of Health in Chiapas, Mexico
Home-based contact tracing with community health workers
Prior to the COVID-19 pandemic, CES was providing home-based support to patients with non-communicable diseases or maternal healthcare needs through the services of community health workers known as ‘acompañantes’ (ACMPs), a team of trained women from the rural communities in which they serve.
In March 2020, the ACMPs team started to conduct home follow-up visits to travellers from high-incidence areas, COVID-19 suspected cases and their close contacts, in order to control the spread of infections and identify high-risk or severely ill patients early. The repeated potential exposure to the virus during the home visits (as the lack of reliable internet or cellular connection precluded remote contact tracing) spread concern among the ACMPs team, which diminished from 89 to 43 individuals. Due to this attrition, CES increased its recruitment and retention efforts by raising ACMPs’ monthly stipends, ensuring access to PPE, and giving regular trainings and remote assistance. From October 2020 to June 2022, CES hired and cross-trained 10 ACMPs for a COVID-19-specific team, all of whom were previously ACMPs from the original programme (eight) or health auxiliaries (two) at CES.
From March 2020 until June 2022, the community contact tracing programme completed follow-up of 27% of all contacts identified at CES-supported outpatient community clinics (2572) (total implementation site population=5598) (table 3).
Communication campaigns to combat misinformation and stigma related to COVID-19
Since the beginning of the COVID-19 pandemic, a lack of reliable information about the disease and vaccination efforts were identified among CES-supported rural communities. This was further evidenced by widespread manifestations of social stigma against persons suspected of having COVID-19 as well as their close contacts. The stigma was rooted in the widespread view of COVID-19 as a death sentence, which made people who knew that someone had COVID-19-related symptoms shun them and their close circles. This made people with symptoms reluctant to tell others to avoid ostracism from the community.
To address these events and mitigate negative impacts on the effectiveness of the COVID-19 strategies that CES and the MOH had been implementing, the SIPC programme carried out an intervention that followed the Risk Communication and Community Engagement action plan guidance for COVID-19 preparedness and response tool provided by the WHO.14
The intervention was conducted in seven out of nine communities due to lack of human resources. It involved an initial assessment and a tailored-door-to-door communication strategy. The purposes of the assessments were to acknowledge and gather the risk perception of community members, general views, main communication channels, influences, knowledge, attitudes and social stigma manifestations related to COVID-19. In the first community evaluated, a questionnaire was carried out that included 71% of all 264 households. For the other six communities, due to the urgent need of the intervention as well as the lack of personnel to implement it, it was decided to shift the evaluation from household to health professionals and ACMPs through applying 3–5 semistructured interviews in each community (n=26) and focus group discussions composed of at least five professionals (n=35). In order to avoid different potential sources of bias, participants were randomly selected, the interviewer was a CES member independent from the clinical team based in the community, and questions were carefully designed to be non-leading.
Finally, key community stakeholders—such as rural agents, teachers, clerks or respected elders—were identified and participated in a social cartography activity (n=81; 8–15 in each community).15 The approach entailed a spatial, participatory and expressive dynamic in a poster in which participants expressed community health problems in the past, present and future. In the present, the transmission of SARS-CoV-2 and the COVID-19 pandemic were identified as one of the problems; it was also identified that action by community members was necessary and space was opened to resolve some doubts and put an end to myths. All participants in the household surveys, interviews, focus group discussions and social cartography were read a letter of informed consent before participation and were only included in the activities after affirmative oral consent was provided voluntarily.
After identifying knowledge gaps and misconceptions around SIPC, as well as attitudes that were counterproductive to the control of the virus, CES designed and implemented a door-to-door communication strategy tailored to the findings in each community, which resulted in changes in knowledge and attitudes of the population as reported by community stakeholders. Changes included an increase in the number of people stating they would attend the clinic if they developed symptoms and cases and contacts identified at the health clinic agreeing to receive follow-up visits from ACMPs. The door-to-door communication strategy could only be implemented in the seven communities in the initial assessment, as it needed to be tailored to each community’s perceived needs and context.
Creation of the respiratory disease clinic
The BCHAAC provides ambulatory and emergency care with only basic infrastructure and limited resources. This situation was exacerbated by the reduction of its clinical staff in the spring of 2020 due to an initiative of the MOH that removed health workers with underlying conditions that elevated their risk of severe SARS-CoV-2 infection from patient-facing work. To counter this situation, CES supported the hospital’s COVID-19 preparedness and response by hiring medical and paramedical personnel, training all staff in SIPC measures, implementing a respiratory triage protocol for all new admissions and establishing a dedicated respiratory ward.
Early in June 2020, the first patient requiring prolonged inpatient admission arrived at the hospital. Unfortunately, the lack of formal certification by the MOH to treat COVID-19 patients in the facility—only MOH facilities classified as Temporary COVID-19 Care Centres or hospitals reconverted as COVID-19 Hospitals could treat these patients—16 17forced health workers to divert COVID-19 suspected cases requiring urgent hospitalisation to other facilities. In addition, the stigmatisation of suspected COVID-19 patients by some health providers, repeated threats from the population against health personnel, and the saturation of the improvised respiratory area in the hospital all contributed to the need for a larger facility to treat COVID-19 patients.
The CES–MOH partnership established the RDC as an intermediate care facility adjacent to the BCHAAC in August 2020. Adaptations were made to an administrative building to manage respiratory emergencies and ambulatory care for suspected or confirmed cases of COVID-19, which was made possible by negotiations between the MOH and CES and by the fact that the centre was managed and operated by the non-state partner. To ensure an adequate oxygen supply, high-pressure oxygen cylinders and concentrators were acquired. In addition, a backup system was installed to maintain the oxygen supply in the event of a power outage.
Hospitalised patients in the RDC received comprehensive care, including diagnostic medicine through medical examination and point-of-care ultrasound, management of comorbidities such as diabetes, hypertension or kidney disease; provision of psychosocial support and palliative and end-of-life care as needed. Patients with severe illness requiring advanced respiratory support were referred for hospital admission or transferred to secondary or tertiary referral facilities.
The RDC was decommissioned in June 2022, due to the drastic decline in respiratory patients hospitalised in the previous months (table 3), which is likely attributable to the increasing immunisation rates in the region.18 During its operation, the RDC conducted 3752 consultations for a total of over 3000 ambulatory and hospitalised patients (total implementation site population=11 875), over 70% with confirmed or suspected COVID-19 (table 3). In addition, the clinic provided over 500 individualised packages of food, according to the needs of the beneficiary, to facilitate isolation for SARS-CoV-2 positive patients.
The COVID-19 hotline
In June 2020, as part of CES’s efforts to combat the pandemic in Ángel Albino Corzo and the surrounding areas—which have reliable mobile phone connection, unlike in rural partner communities—a remote contact tracing programme with a 24-hour hotline was established. Due to the absence of available testing, all suspected cases were initially considered confirmed, and both the patients and their close contacts were monitored in an attempt to break the chain of transmission. Patients with a suspected case of COVID-19 infection seen at the RDC had their general information and high-risk contacts—those living in the same household—entered into a database. This allowed for remote follow-up to begin within the first 24 hours after initial patient encounter.
The protocol was designed to conduct follow-up calls for a minimum of 10 days for all cases. The first call communicated proper isolation procedures and collected comorbidities and other risk factors in addition to symptom monitoring and the provision of psychological first aid. If a patient’s condition worsened, they were immediately referred to the RDC for care. A separate algorithm was used for high-risk contacts, who received quarantine guidance, as well as monitoring for the development of symptoms for the 14 days following their last potential exposure. After verbal screening for symptoms, if cough, fever or headache and dyspnoea, myalgia, arthralgia, odynophagia, chest pain, rhinorrhea or conjunctivitis were reported, they entered the suspected disease pathway and were referred to the RDC.
The COVID-19 hotline has remained active since its launch. From June 2020 to June 2022, the intervention reached 1427 suspected and confirmed COVID-19 cases and 3004 contacts (total implementation site population=11 875) (table 3).
Further collaborations with the public health sector in Chiapas
In addition to the above-described interventions, CES supported other public health facilities by donating rapid antigen tests, facemasks and surgical gowns; and by training on how to perform the testing the health personnel in these facilities. Also, CES collaborated with the MOH authorities to ensure access to anti-COVID-19 immunisations for a population of around 10 000 people.19
Lessons learnt and recommendations
Since the first case of COVID-19 was identified in Chiapas, CES–MOH’s response has been constantly adapting to the changing landscape of the pandemic. Interventions had to be designed and implemented in an emergency context without sufficient time for planning, monitoring and evaluating. Identifying our low rates of completion of contact tracing by ACMPs earlier (much lower than community health worker-led interventions in Oman, Nigeria or the USA)20–22 would have allowed us to modify this intervention sooner.
One of the main pitfalls in the CES–MOH collaboration was the lack of clarity in the roles of each actor. To improve this, we could have clearly specified in the signed agreement the responsibilities of each stakeholder, as well as have solidified communication channels earlier on. Also, at the beginning of the health emergency, some MOH healthcare professionals were reluctant to care for patients with respiratory symptoms out of fear and uncertainty. This placed the greatest workload on CES providers. The lack of official guidelines delineating the obligations of public healthcare practitioners during a pandemic situation made it difficult for the BCHAAC leadership (part of the MOH) to have the official backing needed to ensure that healthcare personnel cared for these patients.
The lack of pandemic preparedness affected all aspects of the Mexican healthcare system: the collapse of the supply chain for PPE,23 medicines24 and oxygen;25 the saturation of available beds in health facilities26 and the exhaustion of health personnel. The latter, due to understaffing, lack of supplies, lack of experience and lack of coping strategies, which appears to have manifested in a high burden of mental health issues among this personnel in Mexico and throughout the Americas.27 28 The CES–MOH team faced all these problems, which led both partners to look strategies to counteract them by involving management and operational staff in the discussions.
When the global supply chain allowed, sufficient supplies were procured to be able to cover the team’s needs for medicines and PPE for enough time to cover potential supply chain collapses in the future. Also, oxygen concentrators proved to be a great solution for oxygen shortages, which was used for patients with moderate respiratory conditions with success, as in other low-income and middle-income countries.29 30 It is worth mentioning that customs authorities in Mexico hindered the importation of oxygen concentrators and other goods such as rapid diagnostic tests from the USA, which impeded our response to the pandemic, despite the calls from international agencies to facilitate trade of life-saving goods.31 32 Further actions should be considered to avoid these barriers to access to supplies in global health emergencies.33
The shortage of beds was only partially solved with the creation of the RDC, as capacity was still limiting during case number peaks prior to immunisation of the population. The well-being of healthcare professionals was addressed by securing enough supplies, staff and training, providing a point of contact from the mental health team at CES, debriefing and defusing groups and virtual well-being groups.34
Finally, the promotion of equity was only partially achieved by the programme. To be health equity promoting, an intervention must address both personal agency and fair access to opportunities to achieve the best possible health.13 Equitable access to decision-making was constrained in the beginning of the pandemic, when most decisions were made in consultation with community leaders, mostly men with a key position in the community. Participatory strategies initiated in early 2021 broadened community consultation to ACMPs, teachers and youth, although the most resource poor and least educated portion of the community was still under-represented. Beyond equity, the importance of engaging communities to ensure the implementability of interventions during the pandemic has been noted in our programme and worldwide.11 35 36 On the other hand, although our interventions prioritised the most underserved rural populations among the implementation sites (tables 1 and 2), provision of social support to those most in need was irregular over time, depending on available resources and restricted by our limited supply chain. This made it difficult to ensure equitable access to opportunities to achieve the best possible health among the population served.
Conclusion
The pandemic highlighted the importance of collaborative work among all stakeholders in health systems. In our experience, we have confirmed the relevance of establishing clear roles for each stakeholder from the beginning of the collaboration and of having fluent communication between actors. We also maintain the importance of involving communities as a whole during the design and implementation of infection prevention and control interventions, monitoring implementation and effectiveness for continuous improvement, as well as building sustainable social support capacity. By describing our public–civil collaboration and lessons learnt, we seek to expand the scarce literature in the field and invite other partnerships like our own to share their valuable experiences, setting a precedent that can strengthen the preparedness of health systems for future disease outbreaks.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was carried out by collecting and analysing routine health data in accordance with the ethical principles of the Declaration of Helsinki. The study was approved by the Research Ethics Committee of the Instituto Tecnológico de Monterrey School of Medicine (P000666-COCESCOVID-CEIC-CR002).
Footnotes
Handling editor Seye Abimbola
Twitter @ZeusArandaR, @SebastianGorsk5
Contributors ALR and ZA are both first authors of the manuscript, and worked on the conceptualisation of the manuscript and all stages of its writing. ZA conducted the literature review. EB, SD, AE, EG, SG, AJ, CUM-O, LM, JM, BV and SV participated in writing the original draft and editing the final version of the text. SC-H worked on the conceptualisation of the manuscript, in all stages of writing, and oversaw the development of the manuscript. All authors discussed the results and provided comments on the manuscript. ZA, LM, ALR, SC-H and JM integrated the reviewer’s comments into the manuscript.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.