Article Text

Abstract
Background There is little evidence of the association between digital marketing of formula and baby food and infant and young child feeding (IYCF) practices.
Objective Assess parents’ exposure to digital marketing of formula and baby food for children <2 years and its association with the purchase and IYCF practices in Mexico.
Methods Parents ≥18 years recruited from a market research panel completed an online survey (n=1074) and capture-on-screen (n=95) between December 2020 and January 2021. Logistic regressions were used to estimate the association between exposure to digital marketing of formula and baby foods with its purchase, motivation, consumption and IYCF practices.
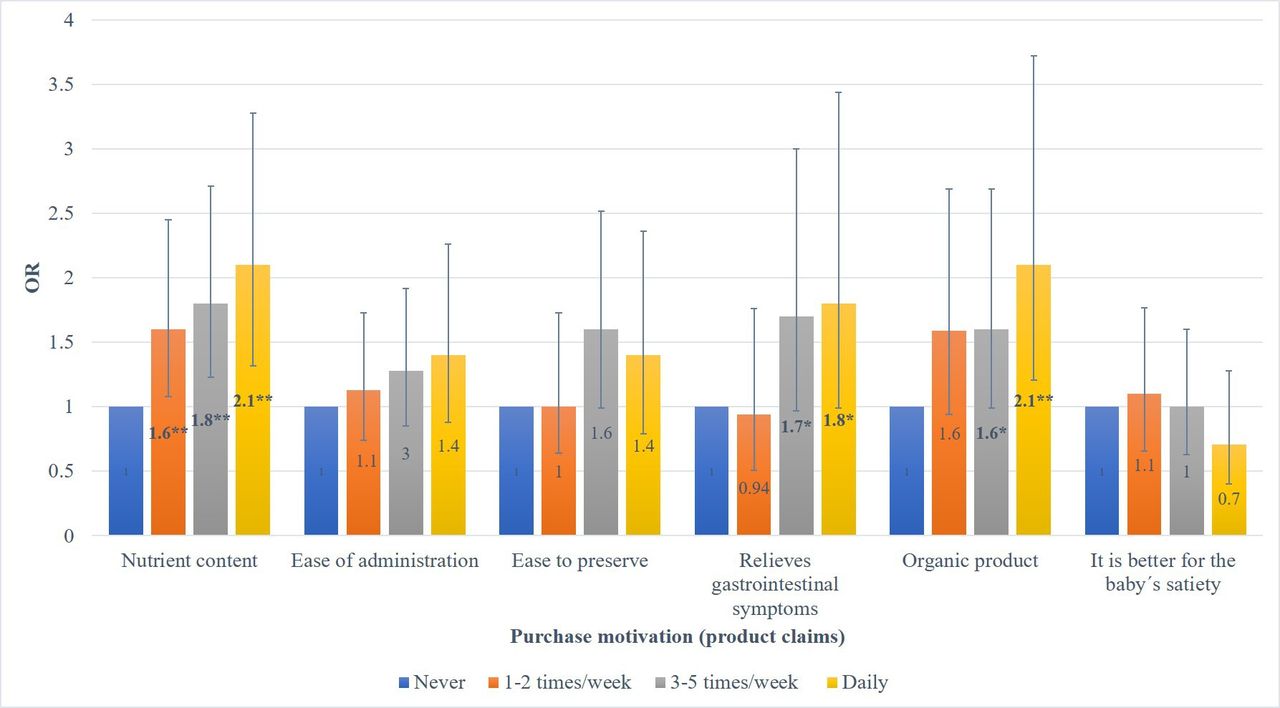
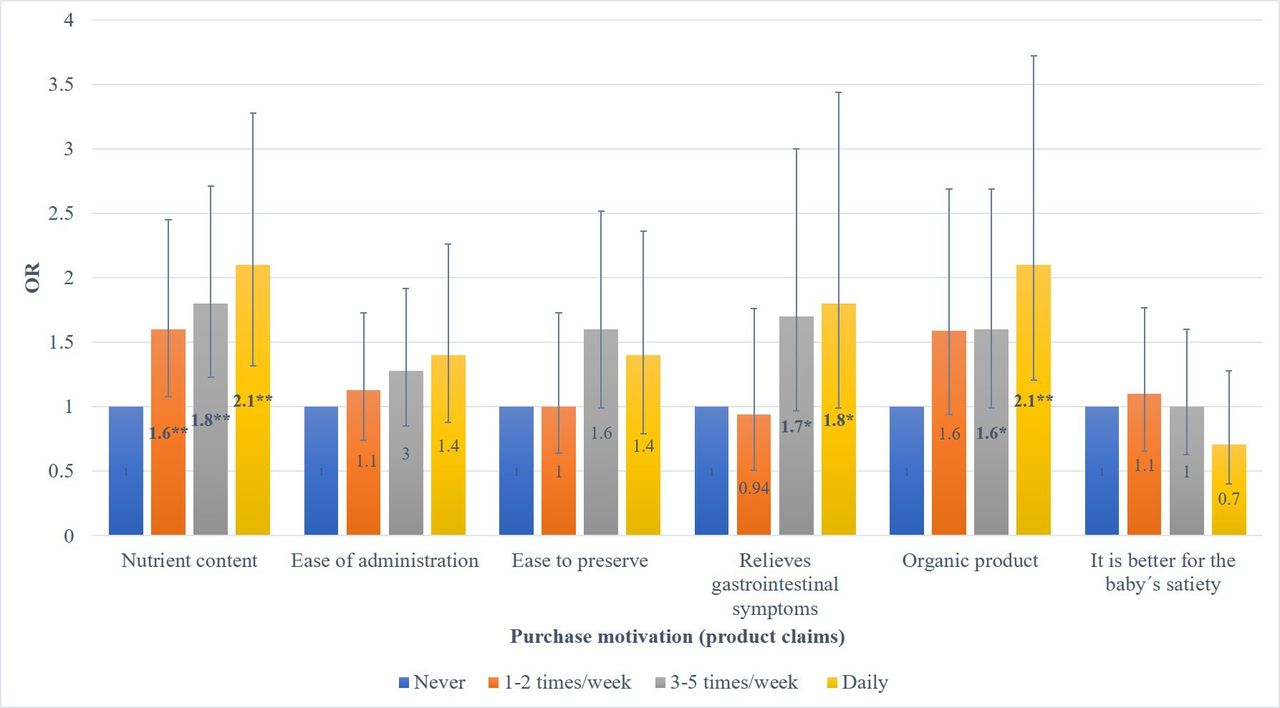
Results Digital marketing of formula and baby food was self-reported by 93.9% of parents in the online survey and observed by 93.7% in the capture-on-screen. Recorded ads did not comply with the International Code of Marketing of Breast-milk Substitutes. Parents who self-reported seeing a higher versus lower number of ads were less likely to exclusive breast feed (OR=0.38; 95% CI: 0.19 to 0.78), and more likely to give mixed feeding (OR=2.59; 95% CI: 1.28 to 5.21), formula (OR=1.84; 95% CI: 1.34 to 2.53), processed foods (OR=2.31; 95% CI: 1.59 to 3.32) and sugary drinks (OR=1.66; 95% CI: 1.09 to 2.54). Higher exposure to ads was associated with a higher chance of purchasing products motivated by nutritional (OR=2.1; 95% CI: 1.32 to 3.28) and organic claims (OR=2.1; 95% CI: 1.21 to 3.72).
Conclusions Digital marketing of formula and baby food may negatively influence IYCF and should be regulated to ensure children’s nutrition and health.
- Cross-sectional survey
- Child health
- Nutrition
- Public Health
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Digital marketing of formula and baby food is increasing worldwide and may affect infant and young child feeding (IYCF) practices, but there is limited evidence.
WHAT THIS STUDY ADDS
Exposure of parents to formula and baby food promotion in digital media may increase the chance of giving formula, sugary drinks and processed foods to their children.
Parents with a high versus low exposure to digital marketing were 62% less likely to exclusively breast feed their children during the first 6 months of life.
Purchase of formula and baby foods may be motivated by the nutritional content claims found in marketing.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Marketing regulations should ban breast-milk substitutes and baby food promotion in digital media and the use of health claims, since they may confuse parents about optimal IYCF.
Background
Breastfeeding and adequate infant and young child feeding (IYCF) practices promote optimal development, generate healthy eating habits and play a crucial role in health outcomes in childhood and throughout life.1–3 One of the main barriers to successful breast feeding is the marketing of breast-milk substitutes, which presents it as a safe option equal to or better than human milk, downplays the benefits and safety of breast feeding4 and influences social norms and adoption of infant formula use.5–7 The International Code of Marketing of Breast-milk Substitutes (Code) recommends that countries implement regulations to prohibit marketing of these products.8 Within its provisions, it is established that informational and educational material should state the benefits and superiority of breast feeding, instructions for the proper use of infant formula and should contain no pictures of infants or other pictures idealising the use of breast-milk substitutes. In addition, no company should seek direct or indirect contact with pregnant women or mothers, fathers and caregivers, including through social media channels.8 Subsequent resolutions of the World Health Assembly recommend the prohibition of companies from donating, disseminating or providing IYCF information and educational materials to parents, providing incentives to health professional, or using health and nutrition claims in relation to infant formula and baby foods.9
Marketing of baby foods, defined as commercial foods and beverages for infants and young children, is associated with a decrease in prolonged breastfeeding10 and poor IYCF practices.11 Baby foods are advertised as a better alternative to natural foods, but many contain excess sugars, fats and salt,12–14 while infant formula (0–6 months), follow-on formula (6–12 months) and growing-up milk (milk-based formulas intended for consumption by children aged 12–36 months) usually contain a high sugar content increasing the risk of caries and overweight or obesity.15
The internet and social media represent a source of information used by parents and caregivers who seek support in feeding their children.16 17 This has allowed companies to have greater reach and better opportunities to promote their products, using unethical campaigns, such as manipulative marketing tactics that exploit parents’ anxieties and aspirations, make inappropriate health and nutrition claims, and encourage health professionals to promote formula milk products,6 many of which are not regulated.18–21 Digital marketing is defined by the WHO as a promotional activity, delivered through a digital medium, that seeks to maximise its impact with creative or analytical methods to activate implicit emotional persuasion.22 Only one study in the USA has documented that exposure to the marketing of formula on websites during the prenatal period decreases breastfeeding intention and initiation.23
In Mexico, only 28.6% of children under 6 months are exclusively breast fed, 42.9% of children under 1 year consume infant formula24 and more than 35% of children between 6 and 23 months consume sugary drinks.25 The promotion of formula has been documented in both traditional26 27 and digital media28 and has been recommended by health professionals.29 Mexican regulations state that marketing of infant formulas (0–6 months) should encourage breast feeding, indicate its benefits and include proper use information.30 Also, formulas should be recommended only when the child is intolerant to breast milk, in the mother’s absence or inability to give milk, in any other well-founded health reason and ban its promotion in healthcare centres and hospitals.31 Since more than 75% of women of reproductive age in Mexico use the internet through a smartphone,32 and the number of internet users is growing,33 analysing digital marketing of formula and baby food is relevant to providing evidence for countries with similar contexts.
This study aimed to estimate the exposure of parents with children <2 years to digital marketing of formula and baby food, its association with the purchase of these products and breastfeeding and complementary feeding practices. The CLICK (Comprehend the digital ecosystem, Landscape of campaigns, Investigate exposure, Capture-on-screen, Knowledge sharing) monitoring framework methodology, proposed by the WHO, was adapted to assess the marketing of unhealthy food aimed at children in digital media.22
Methods
Parents with infants or young children who participated in a nationally representative panel of a market research company34 were invited to complete an online survey. The survey collected information regarding brands, products and digital platforms where parents reported seeing advertisements for formula (infant formula and growing-up milks) and baby foods. Also, the survey asked about purchases made, the intention and motivation to purchase these products and how children’s feeding practices are influenced by digital marketing, as well as IYCF practices of their children including breastfeeding intention and practices. Parents’ knowledge about the Code, their opinion regarding digital marketing regulation and their perception of the company’s responsibility were also investigated.
The participants were recruited by the company through advertisements on apps, social media such as Facebook, several web databases and telephone messages via SMS. Participants had to be over 18 years, live in Mexico, have a mobile device with available internet service, have a child between 0 and 24 months and agree to participate in the study. As a reward for participating, participants received points from the company that they accumulate to redeem for products or cards with electronic balance.
A pilot test was carried out on a sample of 101 individuals to test the instrument, and adjustments were made to the questionnaire. Participants (n=1074) responded to the survey from December 2020 to 23 January 2021.
Sample size estimation
A sample size of 1000 individuals, assuming a 50% prevalence of exposure to digital marketing, a maximum error of 3.1% and a 95% confidence level would allow us to detect an OR of 1.28 between exposure to digital marketing and child feeding practices.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination of the research.
Variables of analysis
The survey had 63 questions, divided into eight sections: (1) sociodemographic characteristics, (2) breastfeeding intention and IYCF practices, (3) use of internet and social media, (4) children’s use of mobile devices, (5) exposure to digital marketing, (6) purchase and motivation of purchasing formula and baby food, and intention and change of children’s feeding practices, (7) perception of infant formula consumption concerning baby’s health and (8) knowledge of the Code, regulations and corporate responsibility (see online supplemental file 2 for full questionnaire).
Supplemental material
Sociodemographic characteristics
Information was obtained on the age and sex of participants, the number of children, sex and age of the youngest child, occupation, marital status, region (North, Centre, Mexico City and South) and years of schooling. Socioeconomic level was measured with the Mexican Association of Market Intelligence and Public Opinion Agencies scale,35 which consists of six questions through which households are classified into seven levels that go from the highest to the lowest (A/B, C+, C, C−, D+, D− and E).
Breastfeeding and child feeding practices
Breastfeeding and complementary feeding practices were evaluated according to status quo or ‘current status’ indicators, constructed with the parents’ recall about their child’s consumption of breast milk and other food and beverages the previous day, as recommended by the WHO and the UNICEF.11 We inquired about early initiation of breast feeding (in the first hour after birth), initial intention of feeding the child before birth (exclusive breast feeding and mixed/formula feeding), exclusive breast feeding in children 0–5 months (consuming only breast milk the previous day), mixed feeding (breast milk and any other type of non-human milk) and continued breast feeding from 6 to 23 months.
IYCF indicators were estimated considering the children’s consumption the day prior to the interview for the following food groups: grains, roots and tubers, legumes, dairy, meat, eggs, fruits and vegetables, breast milk, formula milk (infant formula 0–6 months, follow-on formula 6–12 months, growing-up milk +12 months and formula for special needs), sugary beverages (commercially produced and packaged sweetened beverages such as soda, 100% fruit juice as well as fruit-flavoured drinks to which sweeteners have been added) and processed products which included commercial baby food and other industrialised products (such as chips, candies, cakes, pastries and other baked or fried confections) (online supplemental table 1).
Supplemental material
Use of internet and social media
Parents were asked about the frequency of internet use (never, less than three times a week, three times a week, every day/almost every day), preferred devices to do so and most used social media platforms. The study inquired about the online searches conducted in the last month on topics such as nutrition and infant feeding, information about specific infant formula or baby food products, breast feeding, parenting, child health and development or any other topic related to their children’s health/nutrition. Also, parents were asked if they had visited formula and/or baby food companies’ websites or social media or attended any webinars and if those were held by formula and baby food companies.
Children’s use of mobile devices
Parents were asked if their youngest children used mobile devices, if they had ever downloaded games, baby apps or advergames, defined as free online games that integrate advertising messages, logos and trade characters36, and if they had identified infant formula or baby food advertising on these apps.
Exposure to digital marketing of formula and baby foods
Formula milk was defined as an infant’s liquid food preparation based on cow’s milk or soy protein, given as a substitute for breast milk. This included infant formula (0–6 months), follow-on formula (6–12 months), growing-up milk (12–36 months) and formulas for babies with special needs (lactose free, hypoallergenic, premature baby).
Baby foods were defined as commercial foods and beverages for children under 2 years of age. This category included cereals, porridge, yoghurt, snacks, cookies, puffs, biscuits, juices, baby water and supplements such as Pediasure, a specialised milk containing nutrients for children +12.
Logos of formula and baby food brands and images of their products (online supplemental file 2) placed in the online survey were selected based on the following criteria: (1) products with the highest sales in the Euromonitor report on baby food sales in Mexico,37 (2) most consumed by children according to the National Health and Nutrition Survey (ENSANUT 2018–2019)38 or (3) had a high number of followers on the company’s social media. Products with increasing sales trends were also added to the survey (online supplemental table 2). In the online survey, parents were asked to self-report if they had seen the logos and/or images in the last month on digital media, including banners, sponsored links, websites, search engines, social media (ie, Facebook, Instagram, Twitter), apps, email, news, webinars, YouTube channels and other sources reported by participants.
Exposure to digital marketing of formula and baby food (self-report) was classified as: (a) the weekly frequency in which parents reported observing advertisements in digital media (never, 1–2 times/week, 3–5 times/week, daily) and (b) tertiles of the number of advertised products that parents reported seeing in the last month.
Purchase and motivation of purchasing formula and baby food, and intention and change of children’s feeding practices
Parents were asked if they had purchased any formula or baby food products (online and physical stores) and their motivation for purchasing (for nutritional content, practicality, ease of administration, relief of gastrointestinal symptoms, declaration of being an organic/natural product and satiety of the baby compared with breast milk). We asked if they decided to change their baby’s current feeding, either to stop breast feeding or buy packaged infant feeding products and/or infant formulas due to messages seen in digital marketing.
Knowledge of the Code, regulations and corporate responsibility
The survey inquired if parents were familiar with the Code and, from a list of provisions (ban on breast-milk substitutes advertisement, samples, gifts, donations or low-priced sales and on images of babies or text that idealise their use, and the requirement to state the superiority of breast feeding, to consult with health personnel and to contain health risk warnings), we asked them to indicate which ones they knew or had heard of and if they considered that current regulations were sufficient. We also asked if they considered that the advertising of infant formula and baby food made them think that these products were equivalent or better than breast milk.
Capture-on-screen
A subsample of parents of the online survey (10%) was asked to make three-screen recordings of their mobile device (two during the week and one on the weekend) with a duration of 10 min each (30 min of total recording per person). They were instructed to record while browsing the internet or looking for information on breast feeding, child feeding or while checking their social media, mobile applications or watching maternity/paternity, parenting or feeding videos. They were also asked to record the pages where they searched for or bought formulas and/or baby foods in online stores or search engines. The information was collected in the weeks 14–21 December, 18–25 January and 4 March.
We counted the number of advertisements for formula and baby food products seen in the 10 min of recording and classified them as (a) intentional searches for the product and (b) unintentional searches.
We analysed the type of digital marketing (graphic ads, images or text, discounts and giveaways, learning material, storytelling and peer reviews, cartoon characters or celebrities and webinars), the specific formula and baby food brands and products observed in ads and breaches to the Code including: (1) lack of statements of the superiority of breast feeding, (2) lack of warning by improper preparation, (3) lack of statement about consulting health personal for using the product, (4) invitation to visit a website of the product, (5) invitation to join online parents club, (6) idealisation of the use of formula or baby food and (7) cross-promotion of infant formula (0–6 months) with formulas for older children (+6 months).
Statistical analysis
Sociodemographic characteristics of the participants, their exposure to digital marketing and main IYCF outcomes were described using means and SD for continuous variables and percentages for categorical variables.
Logistic regression models were estimated with the full sample (n=1074). As previously described, exposure to digital marketing was measured as: (a) the weekly frequency reported (never, 1–2 times/week, 3–5 times/week, daily) and (b) tertiles of the number of advertised products reported.
The analysed outcomes were: (1) purchase of any formula and baby foods in the past month; (2) purchase motivation and (3) change in child’s feeding at any time due to marketing (stop breast feeding and/or give formula and baby food). Also, IYCF outcomes included: (4) exclusive breast feeding (0–5 months); (5) mixed feeding (0–5 months); (6) continued breast feeding (6–23 months); (7) consumption of processed products (0–23 months); (8) consumption of formula (0–23 months) and (9) consumption of sugar-sweetened beverages (0–23 months), all on the day prior to the survey.
To reduce bias due to confounding, the models were adjusted for the participant’s age, sex, education, occupation, number of children, child’s age, marital status, socioeconomic level and region, which are the main variables associated with breastfeeding and IYCF practices in the country.24 39 Sensitivity analyses were performed stratifying the models with the initial intention of feeding the child before birth (exclusive breast feeding and mixed/formula feeding).
A subgroup analysis was performed of the association between tertiles of observed formula and baby food ads in the capture-on-screen subsample, both from the result of intentional and unintentional searches, with purchases and IYCF outcomes already described. All analyses were conducted in Stata SE-6 V.4 statistical package.
Results
Sample characteristics
Online survey
Overall, 1080 individuals were invited to participate, and 6 individuals did not answer the survey. Overall, 1074 participants had complete information on all variables. Sociodemographic characteristics of the participants of the online survey are shown in table 1, column A. In total, 62.3% of participants were women. On average, they were 28 years old and had 1.8 children. Half of the children were less than 1 year. Their main occupation was employed or salaried (43.2%), most were married (45.2%), had a bachelor’s degree (44.4%), lived in the Central region (38.4%) and their main socioeconomic level was high (22.5%), average high (24.5%) or average (40.9%) (table 1, column A).
Sociodemographic characteristics of parents with children under 2 years of age who responded to the online survey and capture-on-screen in Mexico
Breastfeeding and complementary feeding practices
Exclusive breast feeding among children under 6 months was 32.6% and continued breast feeding after the first year of life was 45.2%. Among children 0–23 months, 58.2% consumed formula milk, 42.6% consumed sugary drinks and 72% consumed processed foods the day previous to the survey (online supplemental table 3). In the preceding month, 87.2% of parents reported purchasing formula or baby foods in physical and online stores, and 17.7% only in online stores. The main reasons given for the purchase were its nutrimental content (44.6%), ease of preparation (37.1%) and preservation (22.5%) (online supplemental table 3).
Exposure to digital marketing of formula and baby foods
Online survey
In total, 93.9% of parents reported seeing digital marketing on at least one site in the preceding month. Weekly frequency of seeing digital marketing was reported by 86.4% of parents, being most mentioned 3–5 times/week (34%) and 1–2 times/week (25.4%), while 4.5% reported none and 9.0% did not answer. Marketing was observed mainly on social media (77.4%). The mean number of advertised products reported was 26±0.51 SD. The most observed brands in digital marketing were Gerber, Nido and Nan (Nestlé), Enfagrow and Enfamil (Mead Johnson) and Danonino (Danone). Parents reported that the most advertised formulas on digital media were infant formulas (91.9%) and growing-up milk (89.3%), while porridge (77.3%) and yoghurt (70.8%) were the most advertised baby food products (table 2).
Exposure (self-report) of parents of children under 2 years of age to digital marketing of formula and baby food in Mexico
The products were presented in different advertising formats. The ones that the participants remembered the most were graphic ads, images or text (41.9%). In terms of content, participants also recalled seeing promotions, offers, discounts, giveaways (35.9%) and educational material, such as articles, blog posts and menus (31.4%). Parents reported having used social media to share advertising content for formula and baby foods (45.6%). Only 12.7% of parents reported knowing the Code, and less than half (47.7%) considered that the existing regulations for marketing formula and baby food were insufficient. Close to 55% felt that advertising suggests that formula is an equal or even better alternative to breast milk (results not shown).
Capture-on-screen
Overall, 95 out of 101 parents completed 30 min of device recordings (n=285 10 min recordings). Sociodemographic characteristics of the participants of the online survey are shown in table 1, column B. A higher proportion of participants were married, had a bachelor’s degree and had a higher socioeconomic level compared with the online survey participants (table 1, column B).
Overall, 89 parents (93.7%) observed at least one formula and/or baby food ad in their 30 min recordings. A mean of 6.8 ads for infant formula and baby foods/10 min of recording was observed by parents when doing an intentional search on the internet, and 1.7 ads/10 min of recording for unintentional searches. The most advertised product observed in the recordings was growing-up milk (intended for children ≥12 months) (42.3%), although advertising for infant formulas (0–6 months) was also identified (20.2%).
In each 10 min recording, there was at least one piece of advertising for infant formula or baby food was identified (n=168), and all contained Code violations. The main ones related to the lack of statements about the superiority of breast feeding (95.8%), warning of risk or damage by improper formula preparation (95.2%), consulting health personnel about the use of these products (93.5%) and invitation for parents to visit websites, social media or links to purchase their products (69.6%) (figure 1).
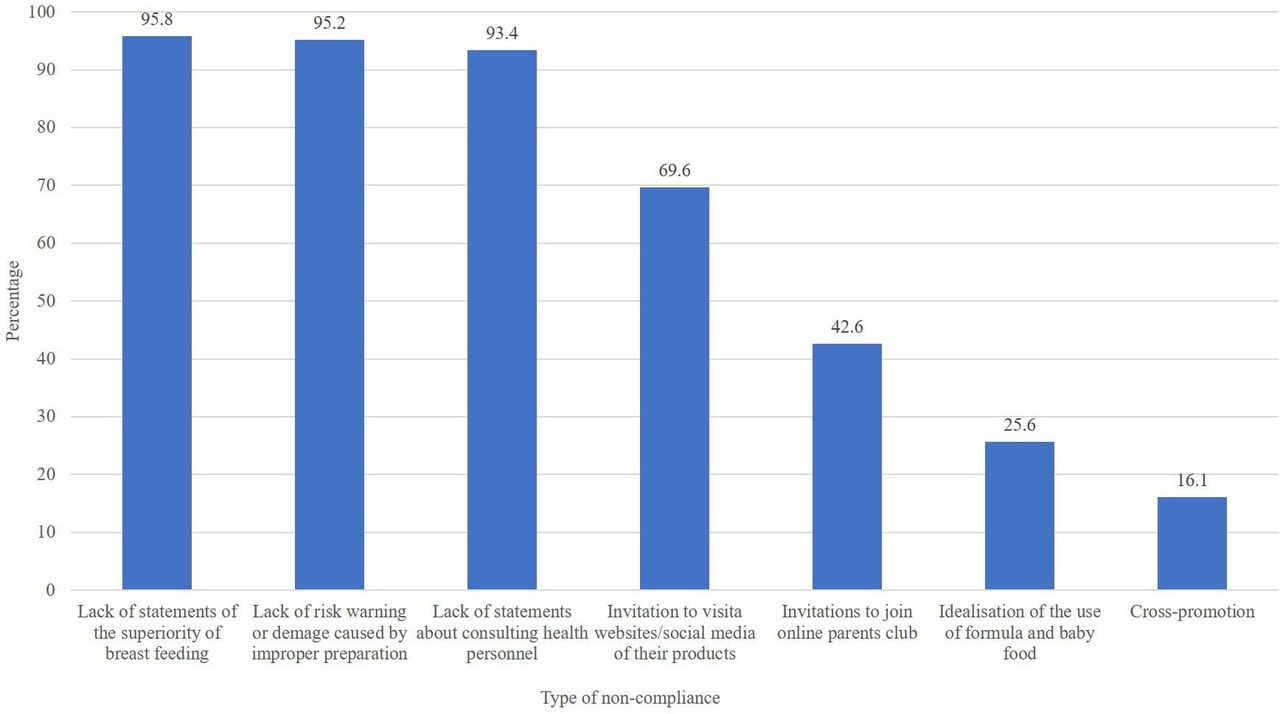
Non-compliance with the International Code on digital marketing in Mexico. Capture-on-screen of parent’s devices with formula and baby food ads (n=168 recordings).
Association analyses
A higher frequency of exposure to formula and baby foods in digital media (self-reported by parents) was associated with greater odds of purchasing these products motivated by nutritional content and organic product claims (figure 2), and also higher chances of changing children’s feeding practices influenced by marketing, giving mixed feeds (0–5 months), giving formula, but also continued breastfeeding children after 1 year, compared with parents that did not observe digital marketing (table 3).
{kind=link}
{kind=link}
Association between frequency of exposure (self-report) of parents to digital marketing of formula and baby food, and motivation of purchase.1 Online survey (n=1074). *p<0.10, **p<0.05. Estimations were made with a logistic regression model adjusted for: the age of the baby (in months), age and sex of the survey participant, socioeconomic level, number of children, marital status, occupation, schooling and region of the country.1 Purchase of formula and/or baby foods (commercial foods for children under 2 years of age) in the last month in physical or online stores.
Association between exposure (self-report) of parents to digital marketing of formula and baby food, with the purchase of products, and breastfeeding and child feeding practices
Reporting a higher (tertile 3) versus lower (tertile 1) number of formula and baby food products in digital media was associated with a lower possibility of exclusive breast feeding (OR=0.38; 95% CI: 0.19 to 0.78), and a greater possibility of mixed feeding (OR=2.59; 95% CI: 1.28 to 5.21), and child’s consumption of formula (OR=1.84; 95% CI: 1.34 to 2.53), processed foods (OR=2.31; 95% CI: 1.59 to 3.32) and sugary drinks (OR=1.66; 95% CI: 1.09 to 2.54) (table 3). Sensitivity analyses, stratifying by intention to exclusively breast feed before birth, show that a higher versus lower exposure to digital marketing was also positively associated with purchase and consumption of formula and sugary drinks, changes in child feeding and giving mixed feeds (online supplemental table 4). Digital marketing of formula and baby food observed in the capture-on-screen subsample was not associated with breastfeeding and complementary feeding practices (results not shown).
Discussion
A high percentage of parents with children under 2 years of age with access to the internet, and with different sociodemographic profiles, reported being exposed to digital marketing of formula and baby food. Capture-on-screen showed that this type of marketing breaches many provisions of the Code and that most parents were exposed to digital marketing, which was consistent with self-reporting. Parents with a high versus low reported exposure to digital marketing were 61% less likely to exclusive breast feed their children during the first 6 months of life, and more likely to give mixed feeds, and formula, sugary drinks, and processed foods to their children. They were more likely to indicate that their formula purchase was motivated by nutrition content claims.
Few studies have examined the relationship between the exposure to digital marketing of formula and baby food and its association with IYCF practices. In the USA, one study showed that pregnant women exposed to infant formula advertising on websites were less likely to intend and initiate breast feeding.23 A study in Mexico showed that 18.2% of mothers with children <18 months reported seeing infant formula advertising on social media in the previous year; however, they did not include baby foods and other digital platforms such as blogs, or companies’ websites, and not all participants had access to the internet, which may explain the low prevalence compared with our results.29
No study has to date adapted the CLICK methodology, proposed by WHO, to investigate the exposure of parents to digital marketing of formula and baby food using both an online survey and capture-on-screen (recordings of mobile devices), to observe what parents see on the internet.22 Another study by the same authors used the CLICK methodology to comprehend the ecosystem of digital marketing with interviews with key social actors and found widespread unregulated marketing methods that violate the Code,40 which is consistent with the results of this study.
In both, the report of the parent’s in the online survey and the capture-on-screen, violations of the Code were identified, which included the advertising of products such as formulas and growing-up milk to direct contact of companies with mothers and fathers through parent’s online clubs. User-shared advertising of formula or baby foods on their social media was reported in the survey and observed in capture-on-screen. This form of marketing is more difficult to monitor and easily goes viral, contributing to a greater reach in the promotion of products and their acceptance by their peers,41 a dynamic that allows the industry to expand advertising of the brand for free, or with very few resources, on social networks and platforms.42 43
The formula and baby food brands that parents reported seeing most frequently on the internet and those observed in capture-on-screen, that is, Nestle, Mead Johnson and Danone are the companies with the highest sales in this product category according to Euromonitor.44 These companies have accumulated assets such as trademarks, copyrights and patents, and economic and human resources that have become forms of instrumental and structural forms of power,45 with which they execute campaigns with the most effective advertising methods, prioritising the generation of profits before compliance with national and international guidelines.
Studies have evidenced the use of nutritional, technical and health claims on formulas and foods and beverages for young children.7 28 46–50 Technical and scientific terms persuade mothers about the safety of these products and cast doubt on the best way to feed their children.47 48 A study conducted with Latino parents in the USA indicated that 72% declared the provision of nutrients in formula as one of the reasons why they would feed their children with this product.51 Evidence indicates that consumers consider a formula healthy if it contains nutrition or health claims,49 which could explain the purchase of the product for reasons related to nutritional content and symptom relief. A recent experiment showed that parents randomly assigned to nutrition claims in fruit drinks such as ‘no artificial sweeteners’, ‘100% vitamin C’ and ‘100% all natural’, versus a control groups with no claims were more likely to choose fruit drinks instead of water for their children 1–5 years old, mistakenly believing these drinks were healthier.52 Other types of claims have no scientific evidence, for example, those referring to the relief of gastrointestinal symptoms or claiming that the product is better for the baby’s satiety.53 The WHO and UNICEF recommend banning claims from formulas,8 and from foods and beverages for young children that do not meet an adequate nutrition profile.54
This study has some limitations. There could be a residual confounding problem due to unmeasured variables that could be associated both with exposure to digital marketing and with infant and child feeding practices. However, we adjusted for the main potential confounders, such as age, parity, education, socioeconomic level, civil status, region and occupation of participants that are related to breastfeeding practices.39 Also, an association between breastfeeding and IYCF practices and self-report of digital marketing was found. Nevertheless, no association with observed digital marketing from the subsample of parents with capture-on-screen was found, possibly due to the small sample size.
The cross-sectional nature of this methodology does not allow us to attribute causality, since exposure to digital marketing does not precede the child’s feeding practices described here. Reverse causation could also be a problem if those who purchase formula and baby food were more likely to take notice of the marketing. However, we found that exposure to digital marketing was associated with a higher chance of purchasing formula and giving mixed feeds among parents whose initial intention was to exclusively breast feed their child before birth, suggesting that marketing interferes with the decisions of parents to breast feed. Since exposure and outcomes are self-reported measures, information obtained could be memory biased. However, the use of validated survey measures for IYCF practices based on the recall on the previous day is less prone to memory bias compared with the recall of a longer period. Similarly, capture-on-screen could be biased since parents were asked to record on their devices when searching for IYCF or childcare.
Additionally, people who participated in this survey were of a higher socioeconomic level and higher education, so the results of this study are not generalisable to the entire population. Nonetheless, the number of internet users with medium and low socioeconomic status is increasing and the effect of inappropriate marketing of breast-milk substitutes may be even greater among vulnerable population groups.
Among the strengths, this is probably the first study to investigate the exposure of parents to digital marketing of formula and baby food using parents’ self-report and device recordings. Findings showed that there is a negative dose–response association between the number of products parents reported seeing in digital media and breastfeeding and complementary feeding practices in young children. Evidencing the urgent need of developing and implementing regulations to monitor and ban inappropriate marketing of breast-milk substitutes in digital media, and the use of health and nutrition claims for formulas and baby foods that motivate their purchase, displacing breastfeeding and adequate feeding practices.
Although the Code recommends broadly banning the promotion of breast-milk substitutes to the general public, countries’ legislation should explicitly mention the prohibition of product placement, influencers, user-generated content, contact of companies with parents through baby clubs, online groups and other strategies used in digital marketing.9 Legislation should also ban companies from disseminating IYCF information and educational materials for parents including digital media, which is considered in subsequent resolutions from the World Health Assembly (WHA69.9). These strategies are used by companies to have direct contact with parents and caregivers, positioning as child feeding and care experts, confusing and misleading parents on their decision to optimally breastfeed and complementary feed their children.55
A digital approach should be used to monitor and prevent infractions in digital media. In this sense, only artificial intelligence and machine learning systems can cope with the velocity and dynamism of digital marketing.56 The feasibility of different strategies such as a digital app that can be used by the general public, health professionals and civil society organisations to report infractions should also be analysed.
Conclusions
Marketing of formula and baby food in digital media was negatively associated with optimal breastfeeding and complementary feeding practices for children under 2 years of age. To limit the company’s influence on IYCF practices, regulations should be implemented, strengthened and monitored regularly. A ban on all forms of marketing of breast-milk substitutes should include digital media and restrict the use of claims for formula and baby foods. This call for action is urgent to safeguard the health and right of children to breast feeding and natural, nutritious, sufficient and quality food.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The study was approved by the ethics and research committees of the National Institute of Public Health (Project CI: 1708). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors are grateful the people who participated in the study for giving us their time and sharing their experiences. The authors are grateful to the internship students: Ana Isabel Rodríguez and Paloma Estrada. And to the anonymous readers and reviewers of the work for their valuable comments on previous versions of the paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @mishaunar, @marena_ceballos, @SBarquera, @abonvecchioa
Contributors MUM is the principal investigator on the grant from United Nations International Children's Emergency Fund. MUM, MS, FCA, MC, LT, SB and ABA conceptualized the project and contributed to the study design. All authors informed the study protocol. MUM, ASG, PJMC, MC, MS and FCA were involved in instrument design. MUM led the study, and ASG and PJMC participated in different subcomponents of the study. Data collection was mainly managed by MUM, ASG and PJMC. MS and FCA supervised the study. MUM contributed to the conceptual design of the analysis and the interpretation of the results. ASG conducted the statistical analyses and presentation of results. MUM and ASG developed the first draft of the manuscript. PJMC, MS, FCA, MC, LT, SB and ABA provided important intellectual content, interpretation of results and policy recommendations. All authors reviewed, revised, and approved the final manuscript. MUM is responsible for the overall content of the manuscript as guarantor.
Funding This study is supported by UNICEF, Mexico.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.