Article Text

Abstract
Background Community health workers (CHWs) play a critical role in supporting health systems, and in improving accessibility to primary healthcare. In many settings CHW programmes do not have formalised employment models and face issues of high attrition and poor performance. This study aims to determine the employment preferences of CHWs in Malang district, Indonesia, to inform policy interventions.
Methods A discrete choice experiment was conducted with 471 CHWs across 28 villages. Attributes relevant to CHW employment were identified through a multistage process including literature review, focus group discussions and expert consultation. Respondents’ choices were analysed with a mixed multinomial logit model and latent class analyses.
Results Five attributes were identified: (1) supervision; (2) training; (3) monthly financial benefit; (4) recognition; and (5) employment structure. The most important influence on choice of job was a low monthly financial benefit (US$~2) (β=0.53, 95% CI=0.43 to 0.63), followed by recognition in the form of a performance feedback report (β=0.13, 95% CI=0.07 to 0.20). A large monthly financial benefit (US$~20) was most unappealing to respondents (β=−0.13, 95% CI=−0.23 to −0.03). Latent class analysis identified two groups of CHWs who differed in their willingness to accept either job presented and preferences over specific attributes. Preferences diverged based on respondent characteristics including experience, hours’ worked per week and income.
Conclusion CHWs in Malang district, Indonesia, favour a small monthly financial benefit which likely reflects the unique cultural values underpinning the programme and a desire for remuneration that is commensurate with the limited number of hours worked. CHWs also desire enhanced methods of performance feedback and greater structure around training and their rights and responsibilities. Fulfilling these conditions may become increasingly important should CHWs work longer hours.
- community-based survey
- health policy
- health economics
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Effective community health worker (CHW) programmes require adequate training and support, including a mix of financial and non-financial incentives.
The Indonesian CHW programme is one of the largest and longest-standing programmes globally yet has been subject to limited research regarding conditions that support motivation and performance.
WHAT THIS STUDY ADDS
A discrete choice experiment with CHWs in Malang district, Indonesia, found a strong preference for a small monthly financial benefit, increasing levels of dissatisfaction as the amount increased and preference for recognition in the form of a report that shows the results of their work.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Preference for a lower financial benefit suggests that the value placed by CHWs on such remuneration may be symbolic, as recognition of their contribution to the community, reinforcing the cultural values that underpin the programme.
Our findings also suggest that kaders value greater feedback of their work and more structure around training and employment conditions.
Introduction
Community health workers (CHWs) play an integral role in strengthening primary healthcare systems by linking communities to healthcare services.1 They are directly connected to the communities they serve—they live in them and are accountable to them—and, in many cases, receive limited training to provide basic preventive healthcare services.2 Beyond these commonalities, CHW programmes vary widely in terms of training, scope of practice and remuneration.3 Staffing models for CHW programmes range from salaried and relatively well-trained workers to volunteers with minimal training.3 4
Since the 1978 Alma Ata Declaration, a substantial body of evidence has emerged demonstrating the contribution of CHWs to improved population health outcomes to reducing health disparities.5–7 Similarly, the factors that influence the performance and motivation of CHWs are also much better understood.8 9 Recent evidence reviews identify a combination of technical enablers such as training, supervision and remuneration, and contextual factors including sustained political support and funding, community embeddedness and integration with the health system.8–10 Yet despite these advances, CHW programmes continue to face the same challenges that have constrained them for decades: inadequate financing, lack of supplies and commodities, low compensation of CHWs and inadequate supervision.11 12 These factors serve to demotivate CHWs and detrimentally affect retention, thus threatening the sustainability of community-based health programmes.13
Indonesia is home to one of the largest and longest-standing CHW programmes globally yet has been subject to relatively limited research.3 The community health workforce, known as kaders, are village health volunteers whose primary task is to organise monthly village health posts, known as Posyandu, where they assist village midwives to provide activities including health and nutrition counselling, immunisation campaigns, monitoring and screening activities for diabetes and hypertension, and maternal and child healthcare.3
In addition to their usual duties, kaders in Malang district of East Java province play a crucial role in the SMARThealth programme—a mobile health-supported community-based intervention to optimise preventative care and treatment for cardiovascular diseases. Kaders screen community members for cardiovascular risk using a tablet-based application, which provides individual risk information, management plans and decision aids to assist nurses and doctors decide on the appropriate treatment for high-risk patients. Over a 2-year trial period in eight villages of Malang district the SMARThealth programme reduced the number of people at high risk of cardiovascular disease by 14.5% and was found to be cost-effective.14 15 In 2020, the programme was adopted by the Malang District Health Authority to be scaled up to all 390 villages in the district, a targeted population (those aged 40 years and older) of one million residents. Ensuring that kaders are well-supported and motivated to perform at a high level will be critical to the continued impact of the SMARThealth programme at scale.
The development of appropriate strategies to support kaders requires an understanding of their preferences for their working conditions. A discrete choice experiment (DCE) is a quantitative survey-based approach to eliciting individual preferences. Respondents are presented with a series of hypothetical choices between two or more alternatives, each of which is described by a set of attributes of varying levels.16 For instance, for patient preferences, respondents may be asked to choose between treatment options that vary in terms of efficacy, cost and side effects. This method allows the analyst to assess the value placed by patients on each attribute and the trade-offs they are prepared to make between them (eg, how much additional cost would they be willing to bear for more efficacious treatments?) and determine overall treatment configurations that optimise overall patient preferences. Furthermore, heterogeneity in preferences between different types of respondents can be assessed.
DCEs have been widely used in health economics research and, more recently, to inform health workforce policies in low-and-middle-income countries.17 The use of DCEs to assess the preferences of CHWs, particularly volunteer CHWs, has steadily grown since 2014.17–23 Findings often highlight that a mix of financial and non-financial incentives are critical to support the motivation, performance and retention of CHWs. For instance, in Kenya, Abuya and colleagues found that transport was considered the most important incentive attribute for volunteer CHWs, followed by tools of trade and job incentives that offered higher monthly stipends.24 Most of these studies have been conducted in African countries, with relatively few in Asia and none were identified carried out in Indonesia.
In this study we conducted a DCE with kaders in Malang district, Indonesia, to assess their preferences for their employment conditions. Results of the DCE will provide health system planners important information on the working conditions that best promote the motivation, performance and retention of kaders and support the scale up of the SMARThealth programme.
Methods
Study setting and participants
Malang is the second largest district in East Java province with a population of 2 874 204 people distributed across 33 subdistricts and 390 villages: 273 (70%) rural and 117 (30%) urban (2018 Census). Kaders are appointed from within their own village by a village committee, to which they are accountable. Kaders are required to receive 3 days of training on the Posyandu curriculum, but previous research has questioned the efficacy of kader training.3 25 According to Puskesmas law (Indonesian Health Ministry Regulation No. 75 Year 2014), kaders are to be guided and supported at the monthly Posyandu by a staff member from the local health centre (puskesmas).3
There is no formalised employment model for kaders and they do not receive a salary. However, kaders typically receive a monthly financial ‘gift’, the amount of which is set at the discretion of the Village Government and commonly varies between 25 000–50 000 (US$2–4) Indonesian rupiah (IDR). Research on incentives for kaders is very limited and somewhat contradictory. Of two small qualitative studies, one found that programme administrators questioned the necessity of financial incentives for kaders while the other reported that administrators thought that a relatively large monthly financial incentive (500 000 IDR, US$~20) was an appropriate amount for kaders.26 27
Attribute development
Identification and selection of DCE attributes was conducted in a multistage process in accordance with the International Society of Pharmacoeconomics and Outcomes Research checklist for conjoint analysis applications in health.28 First, a literature review was conducted to identify employment characteristics of importance to CHWs across a variety of contexts. Second, the transcripts of two focus group discussions with kaders were analysed to understand enablers and barriers faced while performing duties. These focus group discussions were conducted as part of the SMARThealth programme in Malang district.
Emerging themes from the literature review and focus group discussions were used as the basis for attributes that were iteratively refined by the authors in consultation with an expert panel of clinicians and public health researchers from the University of Brawijaya, Indonesia. From this process, five attributes were included in the pilot DCE (table 1). Following translation of the attributes and levels from English into Bahasa Indonesia language, a ‘think aloud’ process was conducted with CHWs (n=5) in Malang district, to test the cognitive intelligibility of attributes and levels.29
Final set of attributes and levels
Piloting
The DCE was pilot tested using approximately 10% (n=30) of the intended sample size to test comprehension and determine whether adjustments in design, descriptions of the attributes and/or administration were required. Once the final DCE content was decided, it was programmed into an Android-based application for data collection and field-tested for a final check of usability and comprehension.
DCE design
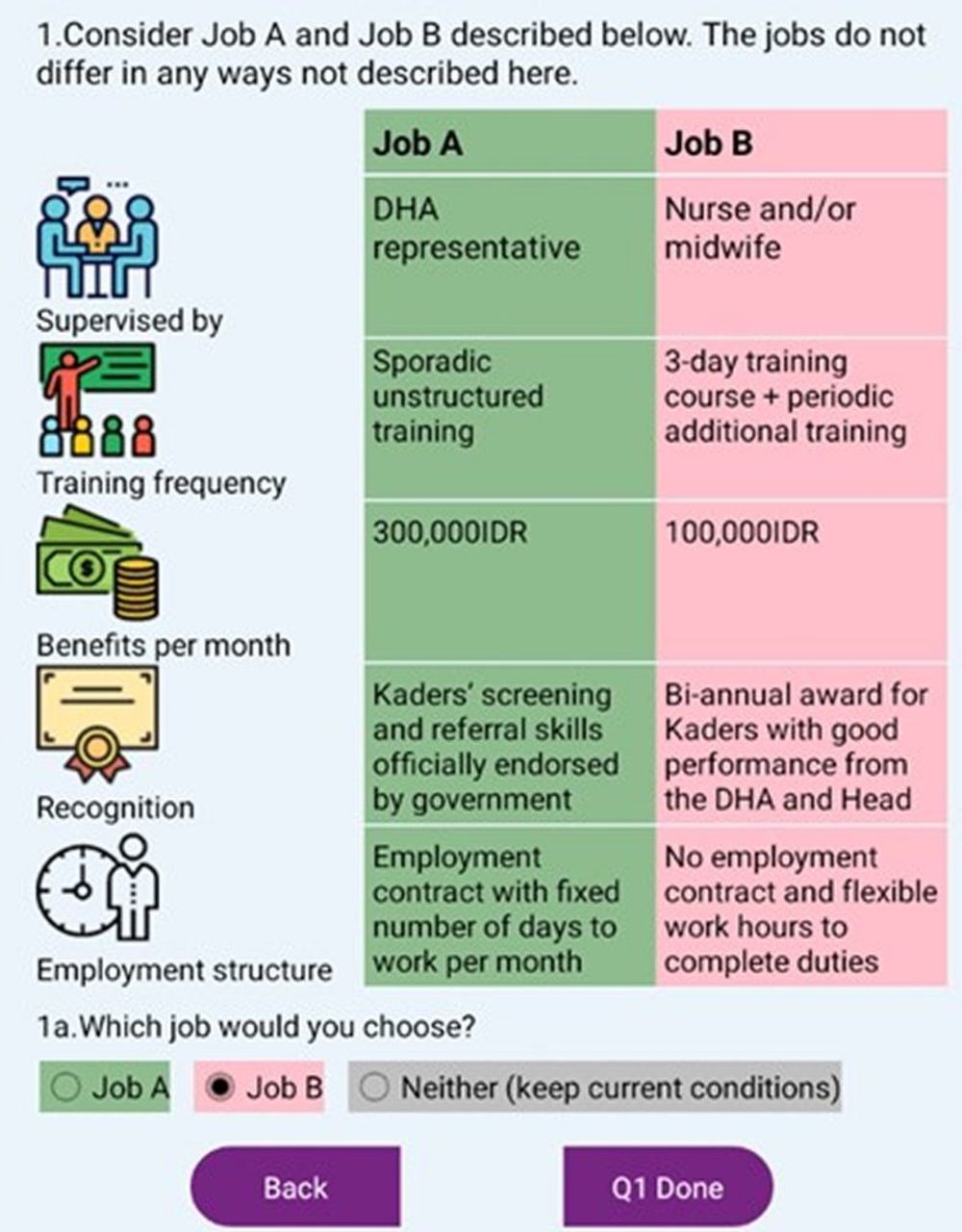
The software Ngene V.1.2.0 was used to design a d-efficient, fractional factorial design using a multinomial logit model. Estimated coefficients for each level were derived from pilot data and used as prior estimates to generate the final survey tool. The final survey consisted of 24 unlabelled choice sets, asking participants to choose between two hypothetical jobs that varied in levels of the attributes. Blocking—whereby the total number of questions is divided equally between two respondent groups—was used to limit respondent fatigue such that each respondent was asked to complete 12 questions. Each choice set included an opt out option; respondents were asked to make an unforced choice (job A, job B or neither job), followed by a forced choice (job A or job B) if ‘neither’ was selected. Figure 1 shows an example choice set in English.

{kind=link}
Example choice set presented to respondents. DHA, District Health Authority; IDR, Indonesian rupiah.
The DCE was preceded by a questionnaire assessing respondent sociodemographic characteristics, years of experience as a kader, hours worked per week and whether they are the main source of income for the household.
Data collection
Data collection was conducted face-to-face in the local language (Bahasa) using an offline Android-based application on computer tablets. The efficiency and feasibility of conducting DCEs through an Android platform has been previously demonstrated.30 In total, 25 villages were visited for data collection. In each village a member of the research team invited all kaders to the village meeting hall and explained the nature of the study to the participants, went through the introductory statement with them, explained the job sets and how to use the tablet device. Kaders completed the questionnaire themselves. Data collection took place between November 2020 and February 2021.
Sample size
Methods for calculating the required sample sizes for DCEs are debated in the literature, with studies commonly relying on ‘rule-of-thumb’ estimates or the use of efficient experimental designs.24 31 32 The sample size calculation for this study was guided by the rule-of-thumb approach, pragmatic considerations around data collection and informed by published DCEs in similar cohorts.19 33 34 According to the rule-of-thumb by Johnson and Orme, the minimum sample size for this study was 84 respondents. However, we aimed to improve statistical precision and allow for examination of subgroups by targeting a sample size of 350–400 respondents.
Statistical analysis
DCEs are based on the random utility theory, which assumes that each respondent will select the alternative that best maximises their individual utility. In this context, utility can best be understood as an indication of the relative preference that respondents attach to each attribute. The sign of each coefficient (β) reflects whether it has a positive or negative influence for respondents, while the magnitude of the coefficient reflects the size of this influence. Descriptive statistics were used to summarise demographic characteristics of the questionnaire preceding the DCE.
Unforced choice data (with options coded as A, B or neither job) were used for all analyses with the respondents’ choices as the dependent variable. All attributes were specified as categorical variables and effects coded. Consistent with current guidance, we first tested the financial attribute as a categorical variable to explore linearity.35 Results suggested a non-linear pattern and better model performance than categorising the attribute as a continuous variable; therefore, we coded the financial attribute as three separate parameters. All analyses were conducted using NLOGIT software V.6.
Three models were estimated to harvest a rich variety of information about respondent preferences. Initial exploratory analysis was undertaken using a multinomial logit model to estimate preferences across all participants (see online supplemental file 1). However, as this model assumes homogeneity of preferences, which is unlikely to be the case, a mixed multinomial logit model was conducted. The mixed model takes preference heterogeneity among participants into account by allowing attribute coefficients to be randomly distributed with a specified probability distribution.36 All parameters were modelled as random with a normal distribution, including the monthly financial benefit since the base multinomial logit model found both positive and negative coefficients for this attribute.
Supplemental material
Next, a latent class model was estimated. This method explores whether there are underlying subgroups (classes) within the sample with similar preferences and can be particularly useful to inform policy recommendations.37 The analyst must stipulate the number of classes and which observed variables to include in the model. A two-class model was assessed by the authors to be the most appropriate to interpret the data as larger class models showed minimal gains in model fit statistics and class sizes became too small for meaningful interpretation (online supplemental file 3). Estimated probabilities of group membership were used to examine the characteristics associated with each group, with the largest probability used to determine the group for each respondent.
Supplemental material
Ethics
The questionnaire was prefaced by an electronic participant information statement in simple Bahasa Indonesia. Participants were required to confirm that they had understood the participant information statement in order to proceed to the questionnaire; completion of the DCE constituted consent.
Patient and public involvement
This research was done without patient involvement due to the subject area and methods chosen. Patients were not invited to comment on the study design, interpret the results or to contribute to the writing or editing of this document for readability or accuracy.
In online supplemental file 2, we present a reflexivity statement on the partnership between high-income and low-income and/or middle-income countries.
Supplemental material
Results
Characteristics of respondents
A total of 480 kaders participated in the DCE and demographic questionnaire, with 471 complete results available (table 2). Nearly all (98.9%) CHWs identified as women, the mean age was 42 years and CHWs had, on average, 11.2 years of work experience. Just under half of the cohort (45.4%) had a senior high school education, 46.9% reported an average weekly household income of more than 500 000 IDR (US$35) and 46.5% reported working less than 2 hours per week as a CHW.
General characteristics of cohort
Preferences
All 471 participants completed all 12 choice tasks, giving 5652 observations. The opt-out option was selected 1181 times (20.9%); thus, we did not analyse the forced choice data as there was sufficient information to run the model with the opt-out option.
Results of the mixed multinominal logit model are presented in table 3. Results show that respondents have a strong preference for the lowest monthly benefit amount (β=0.53, 95% CI=0.43 to 0.63) and found higher amounts unappealing. Regarding forms of recognition, the only option that appealed to respondents was receiving a report to see the results of their work (β=0.13, 95% CI=0.06 to 0.20). While respondents expressed a marginal preference for having an employment contract (β=0.10, 95% CI=0.07 to 0.14), the opt-out option was very unappealing (β=−0.76, 95% CI=−0.86 to −0.67) suggesting the range of hypothetical job scenarios presented were generally not extreme enough to warrant not working under those conditions. Supervision format and training frequency did not have an influence on respondents choices.
Results from mixed multinomial logit model for full sample (R2=0.182, AIC=10 200.1, BIC=10 332.9)
Latent class analyses
The latent class model detect two distinct groups with heterogeneity in preferences, comprising 68.8%, and 31.2% of our cohort, respectively (table 4). The general characteristics of the groups are shown in online supplemental file 4. Kaders in group 1 (68.8% of the sample, n=324) were more likely to be older, have more years’ experience, work less hours per week and have a higher average income. Comparatively, those in group 2 (n=31.2%, n=147) were younger, less experienced, had a lower income and work more hours per week.
Supplemental material
Latent class logit model results (n=471, McFadden pseudo R2=0.269, AIC=9121.6, BIC=9261.1)
The most significant divergence of preferences was in relation to the opt-out option. Group 1 kaders were highly unlikely to reject either of the jobs presented (β=−4.41, 95% CI=−3.89 to −4.92), while those in group 2 preferred not to accept either job (β=1.46, 95% CI=1.35 to 1.57). Reflecting this sentiment, group 1 kaders expressed marginal preference for the current supervision format (β=1.23, 95% CI=0.55 to 1.92), while those in group 2 strongly disliked it (β=1.23, 95% CI=0.55 to 1.92). Preference for a small monthly financial benefit was consistent across both groups.
Discussion
To our knowledge, this is the first DCE to be conducted with the community health workforce, known as kaders, in Indonesia. While we find some level of preference heterogeneity among kaders in Malang district, the majority valued jobs that provide a lower monthly financial benefit, recognition in the form of a report on their performance and more structure around training and contract status. CHWs expressed indifference towards recognition in the form of government endorsement, an award for good performance and higher amounts of the monthly financial benefit. Latent class analysis suggested that the main drivers of preference heterogeneity are age, years’ of experience, the number of hours worked per week and income.
The most salient finding from this study is that the majority of respondents expressed a strong and consistent preference for the lowest monthly financial benefit and opposition to higher amounts. This unexpected result contrasts with findings studies of community health worker employment preferences conducted elsewhere.18 21 22 24 This may be partly explained by the strong prosocial foundation underpinning Indonesia’s kader programme, which emphasises the cultural and religious value of ‘gotong royong’, a concept that promotes communal service and volunteering for one’s neighbourhood.38–40 Recent qualitative research suggests that these values remain relevant to kaders, finding that not only did they not expect a financial incentive for their work, but that it may even weaken their motivation.25 26 Furthermore, the preference for a lower monthly financial benefit found among our study cohort—the majority of whom reported working less than 4 hours per week—may suggest that kaders prefer a financial benefit that is commensurate with their workload: previous research has found that kaders who were engaged in a more time-intensive healthcare intervention were open to receiving a larger monthly financial benefit.27
Recognition is a key motivator of CHWs, yet it can be a challenging concept to capture within a DCE. Similar studies have relied on broad statements indicating a high or low level of support from the community or described forms of recognition that are more akin to incentives such as ‘priority healthcare for family members’ or ‘career progression’.20 22 Our levels for the recognition attribute were informed by the evidence base and highlighted by kaders in our source material, yet only one level influenced respondent choices. Respondent’s preference for recognition in the form of a report on their work suggests that kaders prefer some form of performance feedback and appraisal which provides them the means to improve their work. This is consistent with our finding that kaders favour a more structured approach to training opportunities. Assessments of current support systems for kaders are limited, but these findings ties in with previous research that characterised the support provided by village midwives to kaders as unstructured and ‘not very supportive or motivating’.25 Previous research has shown that enhanced training and supervision of kaders can lead to improved community health outcomes.41–43
Latent class analysis revealed heterogeneity among respondent preferences. Notably, preferences diverged based on respondent characteristics including experience, hours’ worked per week and income. The majority of respondents were more likely to be experienced kaders who worked a small number of hours per week. Results suggest they are satisfied with current working conditions but prefer more structured training, performance feedback and an employment contract. Their dislike of a higher financial benefit may suggest that a small incentive is seen as commensurate with their duties and a higher amount may be perceived to come with the expectation of increased hours and responsibility. Comparatively, around a third of respondents, who are younger and work more per week, expressed dissatisfaction with current conditions. Should the SMARThealth programme require kaders to work longer hours, these differences will need to be considered.
While it is important to acknowledge these discrepancies, from a policy perspective decisions need to be contextualised to the overall preferences of kaders. In terms of policy relevance, there are a few clear take-aways from this study. First, our finding regarding the current monthly financial benefit suggests that the current policy (of approximately 25 000–50 000 IDR per month) is appropriate and acceptable to the majority of kaders in Malang district. Second, kaders’ preference for a report on their work suggests that there may be scope to provide additional forms of appraisal or feedback on their performance suggesting support for the idea of ongoing quality improvement. Previous studies have shown that similar interventions have led to improvements in kader performance.42 44 Third, marginal preferences for the training attribute and an employment contract suggests that kaders favour a more structured approach to their positions and greater certainty about roles, responsibilities and rights.
Limitations
Our study sample was not nationally representative and thus, while the findings can be generalised to the Malang district, they may not be applicable to other areas of Indonesia. Second, we did not perform any tests to ensure internal validity of the DCE among participants. Instead, we used a ‘think aloud’ technique to cognitively test our DCE and blocking of the questionnaire to limit the number of scenarios presented and cognitive burden on respondents. Last, due to time and cost considerations kaders were non-randomly sampled for inclusion in the DCE yet this should be mitigated by the large sample size and large number of diverse villages visited for data collection.
Conclusion
In this DCE kaders in Malang district, Indonesia indicated a strong preference for a small monthly financial benefit, recognition in the form of a report that shows the results of their work and an employment contract with a fixed number of days to work per month. Importantly, kaders expressed a strong dislike for higher levels of financial benefits, perhaps suggesting resistance to the associated expectations this may bring and the undermining of altruistic motives driving their activities. These findings reinforce the cultural values that underpin the kader programme and highlights potential avenues to improve how kaders are supported.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Human Research Ethics Committees of the University of New South Wales (HC190048) and Medical Faculty of University of Brawijaya (Reference: 10/EC/KEPK/04/2018).
Acknowledgments
We would like to acknowledge Nirosha Yeddalapudi and Sridevi Gara from The George Institute for Global Health India for their work in developing the Android discrete choice experiment application. Additionally, we would like to acknowledge the data collection team from the University of Brawijaya.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Lei Si
Twitter @sujarwoto, @DrRetha
Contributors Conception or design of the work: AP, SS, GT, AM, SJ, TG, BA and NP. Data collection: SS and NP. Data analysis and interpretation: TG, BA, GT and AM. Drafting the article: TG, BA and AP. Critical revision of the article: AM, GT, SJ, DO and DP. Guarantor: TG
Funding This study was funded by a programme grant from the Australian National Health and Medical Research Council (NHMRC) (Grant ID: APP1149987). TG is supported by a university postgraduate award from the University of New South Wales. AP is supported by an NHMRC Early Career Fellowship. SJ is supported by an NHMRC Principal Research Fellowship. BA is supported by an NHMRC Emerging Leadership Investigator Grant.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.