Article Text

Abstract
Since the first case of COVID-19 in Djibouti in March 2020 up to the end of May 2021, the country experienced two major epidemic waves of confirmed cases and deaths. The first wave in 2020 progressed more slowly in Djibouti compared with other countries in the Eastern Mediterranean Region. The second wave in 2021 appeared to be more aggressive in terms of the number and severity of cases, as well as the overall fatality rate. This study describes and analyses the epidemiology of these two waves of the COVID-19 pandemic in Djibouti and highlights lessons learnt from the National Plan for Introduction and Deployment of COVID-19 vaccines developed and implemented by the Ministry of Health of Djibouti.
From 17 March 2020 up to 31 May 2021, Djibouti officially reported 11 533 confirmed cases of COVID-19 with 154 related deaths (case fatality rate, CFR: 1.3%), with an attack rate of 1.2%. The first epidemic wave began in epidemiological week 16/2020 (12–18 April) and ended in epidemiological week 25/2020 (14–20 June) with 4274 reported cases and 46 deaths (CFR: 1.1%). The second wave began in epidemiological week 11/2021 (14–20 March) and ended in epidemiological week 18/2021 (2–8 May) with 5082 reported cases and 86 deaths (CFR: 1.7%).
A vaccination campaign was launched by the President of the Republic in March 2021; approximately 1.6% of the population were vaccinated in only two months’ time. Early Preparedness, multisectoral and multicoordinated response, and collaboration with WHO are among the major lessons learnt during the pandemic in Djibouti.
- COVID-19
- vaccines
Data availability statement
Data are available in a public, open access repository. All data belongs to the MoH of Djibouti and it is available in the daily pubic communiqué of the ministry.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Previous studies showed that the second wave of COVID-19 was more severe than the first wave in most of the countries globally, this was the case of Djibouti that experienced two epidemic waves of COVID-19 since the emergence of the virus in the country in March 2020.
Djibouti focused on two major pillars for response to the pandemic, the Risk Communication and Community Engagement and the vaccination.
This study describes the epidemiology of the two waves of COVID-19 in Djibouti and highlights lessons learnt from the response to the pandemic in the country.
Our findings show that early preparedness, multisectoral and multicoordinated response, and collaboration with WHO are among the major lessons learnt that helped Djibouti to respond adequately to the pandemic compared with other countries in the region.
Introduction
The COVID-19, caused by the SARS-CoV-2, and declared officially by the WHO as a pandemic in March 2020, has caused an unprecedented global health threat.1 2 In addition to the tragic impact on health systems in different countries, this pandemic caused the collapse of economies and societies around the world.3 As of 31 May 2021, 172 689 060 confirmed cases and 3 723 931 deaths were officially reported with a global case fatality rate (CFR) of 2.2%.4
After more than a year and a half since the emergence of the SARS-CoV-2, nearly all countries have reported several waves of the pandemic, with a higher severity of the virus during the second or third waves, where, for example, in Djibouti, we noticed a remarkable increase in the number of reported severe cases and fatalities, compared with the first wave.5 6 The same pattern occurred across Africa.7 As early as February 2020, African nations, no stranger to epidemic diseases, took robust action to implement lockdowns and non-pharmaceutical interventions to quell the spread of the virus.8 9 As of 31 May 2021, African countries had reported 4 833 730 confirmed cases of COVID-19 and 130 373 deaths, for a CFR of 2.7%.4 Considered as the most vulnerable continent with its weak health systems and infrastructure, Africa somehow reported a lower number of COVID-19 cases compared with other developed continents and countries.10
COVID-19 in Djibouti
From 17 March 2020 up to 31 May 2021, the Republic of Djibouti reported 11 533 confirmed cases of COVID-19 and 154 deaths,11 for a CFR of 1.3% and a test positivity rate of 7.3%. Early preparedness and close collaboration with health partners, especially WHO, to develop the COVID-19 National Preparedness and Response Plan in March 2020,12 helped Djibouti to respond to the first wave of COVID-19 in an optimum way, with a mere 4274 reported cases including 46 deaths, for a CFR of 1.1%.
After the first wave, the country gradually started the de-confinement process from 17 May 2020, with nearly all measures removed by the opening of the airport on 17 July 2020.13 On 28 December 2020, there was the declaration of a presidential decree creating a National Committee in charge of the Introduction and Deployment of the COVID-19 vaccines in the Republic of Djibouti.14 The committee, composed of some vaccination experts in the country with the involved health partners, including WHO and UNICEF, started immediately working to develop and deliver a national plan, that was officially validated by the president of the Republic on 9 February 2021.15
Epidemiological surveillance in Djibouti
The Ministry of Health (MoH) of Djibouti conducted 158 803 COVID-19 tests from 17 March 2020 to 31 May 2021, with epi week 23/2020 (31 May 2020–6 June 2020) having the highest number of performed tests: 8692 (figure 1). During the same period, 11 533 confirmed cases of COVID-19 were officially reported by the MoH, with epi week 13/2021 (28 March 2021–3 April 2021) having the highest number of positive cases; 1260 positive cases (figure 2). The total number of reported deaths was 154, with epi weeks 14 and 15/2021 (4–10 April and 11–17 April 2021) having the highest number of recorded deaths; 21 deaths in each week. The CFR for this period was 1.3% and the attack rate was 1.2%.

COVID-19 positive cases and number of tests conducted per epidemiological week in Djibouti.
Two peaks (waves) of COVID-19 pandemic in Djibouti were observed since the first case was reported in the country on 17 March 2020. The first observed wave started few weeks after the beginning of the pandemic. It started on epidemiological week 16, from 12 April 2020, and lasted up to 20 June 2020 (Wk 25). During this wave, 4274 confirmed cases were reported by MoH Djibouti including 46 deaths (figure 2), for a CFR of 1.1%. The country faced a more severe second wave with a higher number of cases and mortality rate. It began in epidemiological week 11, from 14 March 2021, and continued up to epidemiological week 18, until 8 May 2021. During this wave, 5082 confirmed cases were reported MoH of Djibouti including 86 deaths (figure 2), for a CFR: 1.7%.
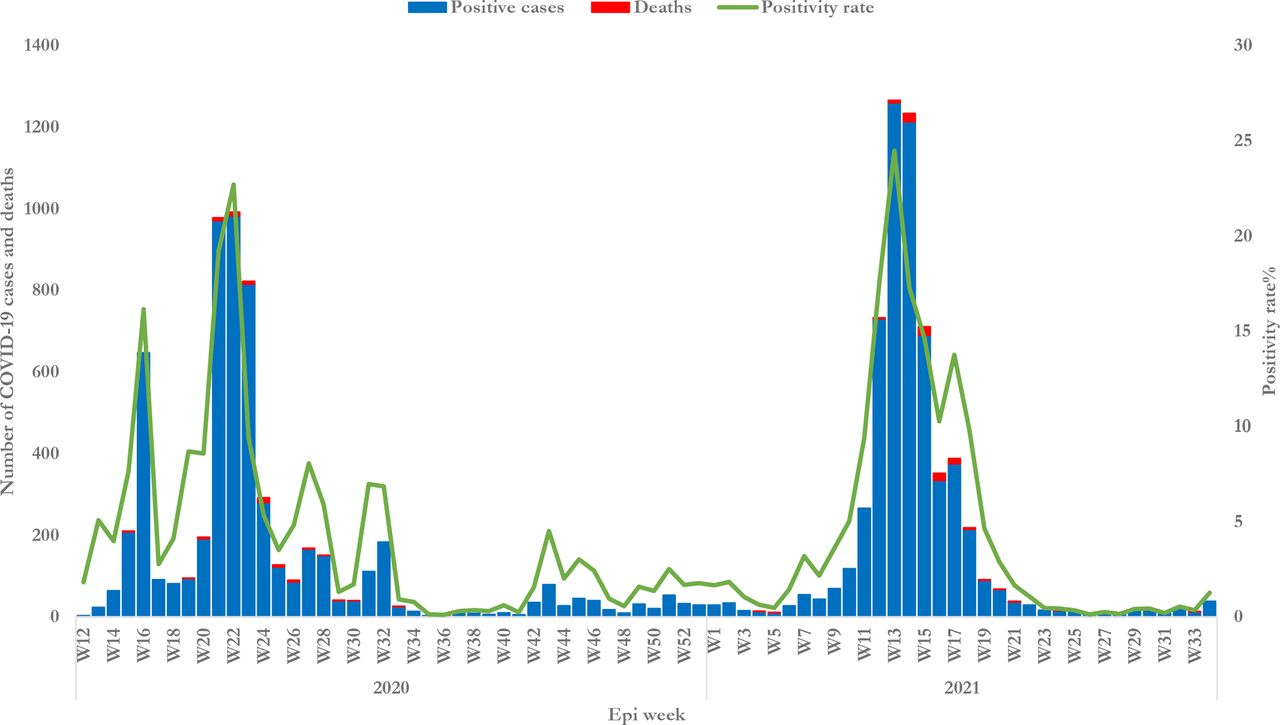
COVID-19 confirmed cases, deaths and the positivity rate per epidemiological week in Djibouti, from 17 March 2020 to 31 May 2021.
The mortality rate during the second wave in Djibouti was higher than the first wave as was true for most of the countries in the region and globally.5 6 The total number of reported deaths during this period reached 154 fatalities, with the highest number of reported fatalities from 4 to 17 April 2021 (from epi week 14 to 15/2021) for a total of 42 deaths. The CFR of COVID-19 pandemic in Djibouti was 1.3% during this period. The test positivity rate varied from 1% during the stable periods, up to 24% during the peak of the second wave, with an overall positivity rate of 7.3%. During the first wave, the highest positivity rate was reported in the epidemiological week 22/2020, at 23% (figure 2).
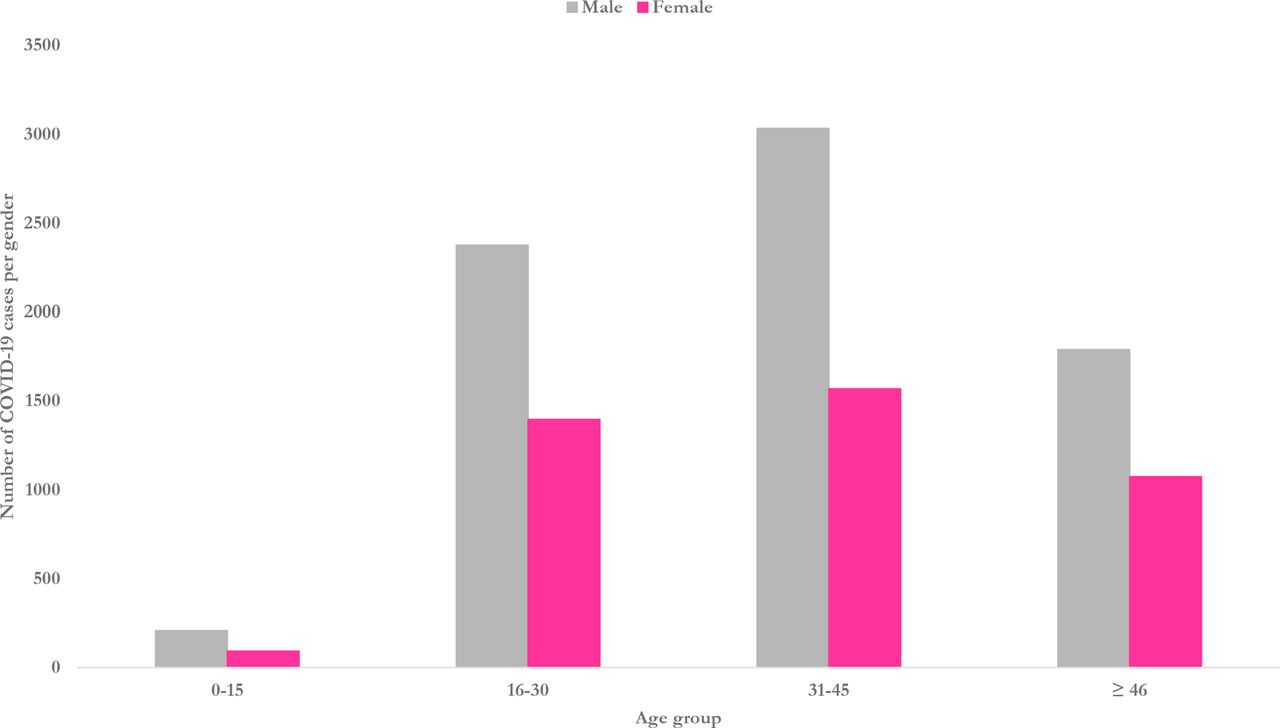
The demographic characteristics of COVID-19 cases in Djibouti showed that male gender dominated the reported cases during both waves with 67.4% (2,881) of the lab-confirmed cases in the first wave and 64.2% (3263) in the second wave. The age group most affected by the emerging zoonotic virus was the age group 31–45 years old with 33.2% (1 419) of the cases during the first wave and 39.9% (2028) during the second wave, followed by the age group 16–30 years old with 32.3% (1 381) of the cases during the first wave and 32.7% (1662) during the second wave (figure 3). With one of the youngest populations of Africa, Djibouti has a demographic pyramid with a median age of 20 years old with more than 85% of the population less than 49 years old.16

COVID-19 positive cases distributed by gender and age group.
During the first wave of the disease, four out of six regions in Djibouti were affected by the COVID-19 pandemic including: Djibouti-Ville, Arta, Ali Sabieh and Dikhil regions. While during the second wave, and due to some mass gatherings, that happened in the north part of the country, Tadjourah and Obock regions also reported clusters of cases of COVID-19. Djibouti-ville, the capital, was the most affected region in the country with COVID-19 cases in both waves. This comes as no surprise considering 70%–75% of the population reside in the capital.16 The positivity rate of COVID-19 cases up to the end of epi week 22/2021 (31 May 2021) varied enormously from 0%–1% during non-peak periods to approximately 23%–24% during the peaks of the waves, for an overall positivity rate of 6% during the entire period.
After the official launching of the COVID-19 mass vaccination campaign in Djibouti on 15 March 2021, 16 063 persons (1.6% of the population) were vaccinated with three different vaccines by 31 May 2021: AstraZeneca (Covishield), Sinovac and Sputnik. Figure 4 shows the accumulative number of doses administrated in Djibouti during this period, around 20 550 doses (2.05% per 100 people) with 4487 persons fully vaccinated with two doses, while 11 576 persons were partially vaccinated with only one dose.

Cumulative number of administrated COVID-19 vaccines in Djibouti per 100 people.
Governmental strategy and laboratory capacities
Since the emergence of the COVID-19 pandemic in the country, the government of Djibouti followed a very strict strategy based on four pillars that conform to the recommendations of the WHO preparedness and response strategy. The pillars of the strategy are: Testing COVID-19 suspected cases according to the case definition, by taking the needed swabs for the PCR test; Isolating all detected positive cases in an isolation centre prepared specifically for this reason by the government in Arta region; Starting early case management for all positive cases even before the development of symptoms; and Conducting a strict contact tracing procedure for all contacts of positive cases, testing them and isolating those who are found positive.17
This strategy was based on collaborative work between different ministries and entities including the MoH, the Ministry of Defence, the Ministry of Interior and other health partners. The government followed this strategy till the end of the first wave in June 2020, when scarcity of human resources in the country did not allow the deployed teams to continue their work. Furthermore, the strategy was updated multiple times based on the epidemiological situation of the virus in the country, the region and globally.
Djibouti conducted 158 803 tests (16.1% of the population) for suspected COVID-19 cases during the designated period as well as for all travellers who needed a negative certificate for travel and contacts detected through the contact tracing procedure during the first phase of the response. Till the end of May 2021, all RT-PCR tests conducted for COVID-19 in Djibouti were centralised in Bouffard hospital, the only accredited laboratory for such tests in the country.
Plan for introduction and deployment of COVID-19 vaccines in Djibouti
Huge and continuous work, for more than 2 months, has been conducted by the National Committee for deployment of COVID-19 vaccines in Djibouti; and because of its demonstrated efforts to develop and validate a national plan for immunisation, Djibouti was the second country in the Middle East and North Africa region to receive COVID-19 vaccines, with 24 000 doses of AstraZeneca (Covishield) at Djibouti International Airport on 6 March 2021.18 The vaccines were delivered through the COVAX facility, which is a coalition co-led by the WHO, UNICEF, GAVI (the Vaccine Alliance) and the Coalition for Epidemic Preparedness Innovations that ensures fair and equitable distribution of COVID-19 vaccines to countries regardless of their income.19 Immediately after the reception of the first batch of the vaccines, the President of the Republic of Djibouti officially launched the country’s first COVID-19 mass vaccination campaign on 15 March 2021.20
The Plan for Introduction and Deployment of COVID-19 vaccines in Djibouti has as objectives: (1) Protect vulnerable groups at high risk of severity of the disease, with the focus on elderly and persons with comorbidities; (2) Reduce the impact on the personnel responsible of case management of the COVID-19 patients and reduce the transmissibility; (3) Ensure vaccine safety and postvaccination follow-up. It focused on a priority target population that should be vaccinated before the rest of the population including: (1) Health personnel at high risk of infection, especially the healthcare personnel in emergency departments, intensive care units and patients managing these comorbidities, and the non-medical personnel in contact with patients; (2) People with comorbidities aged over 50 years; (3) People with comorbidities over 18 years of age suffering from chronic respiratory diseases (due to the high incidence TB in the country), chronic renal insufficiency, hypertension, diabetes, coagulopathies, cancers and other chronic pathologies; (4) Volunteers over the age of 40.
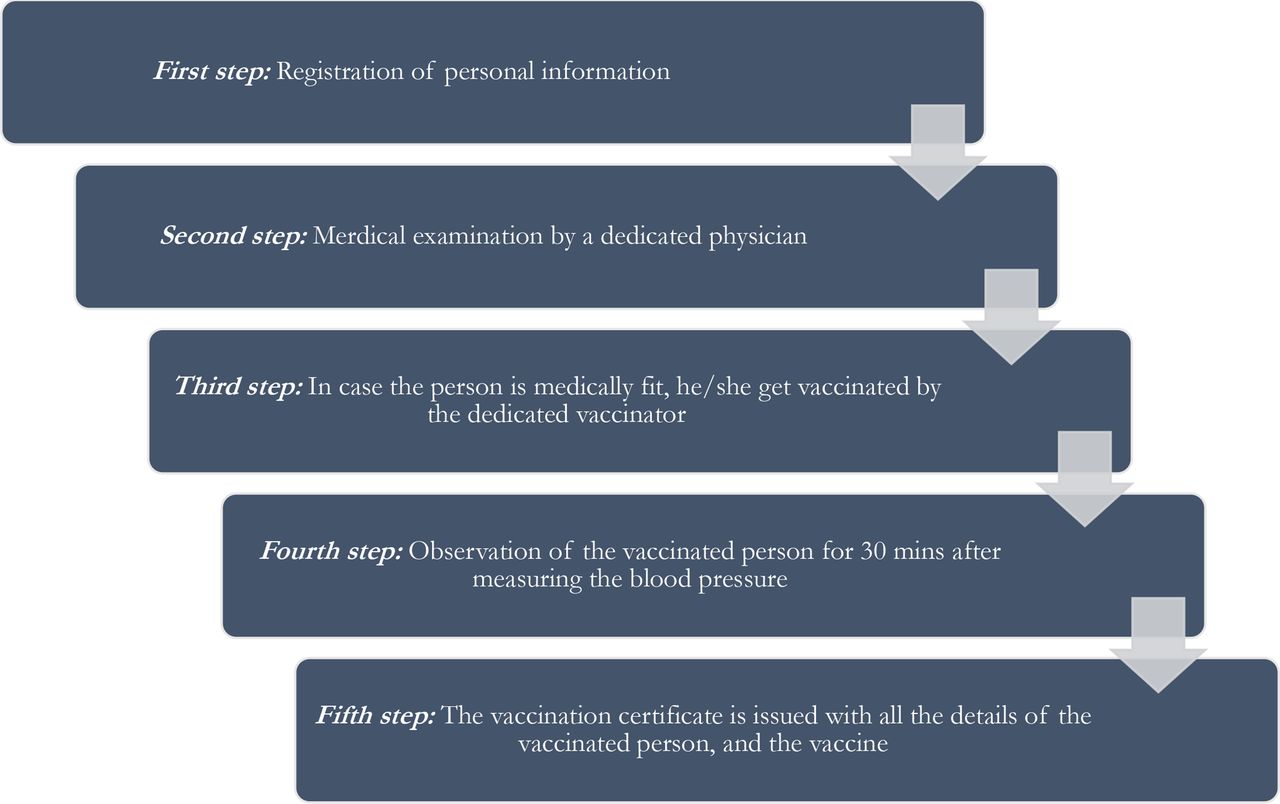
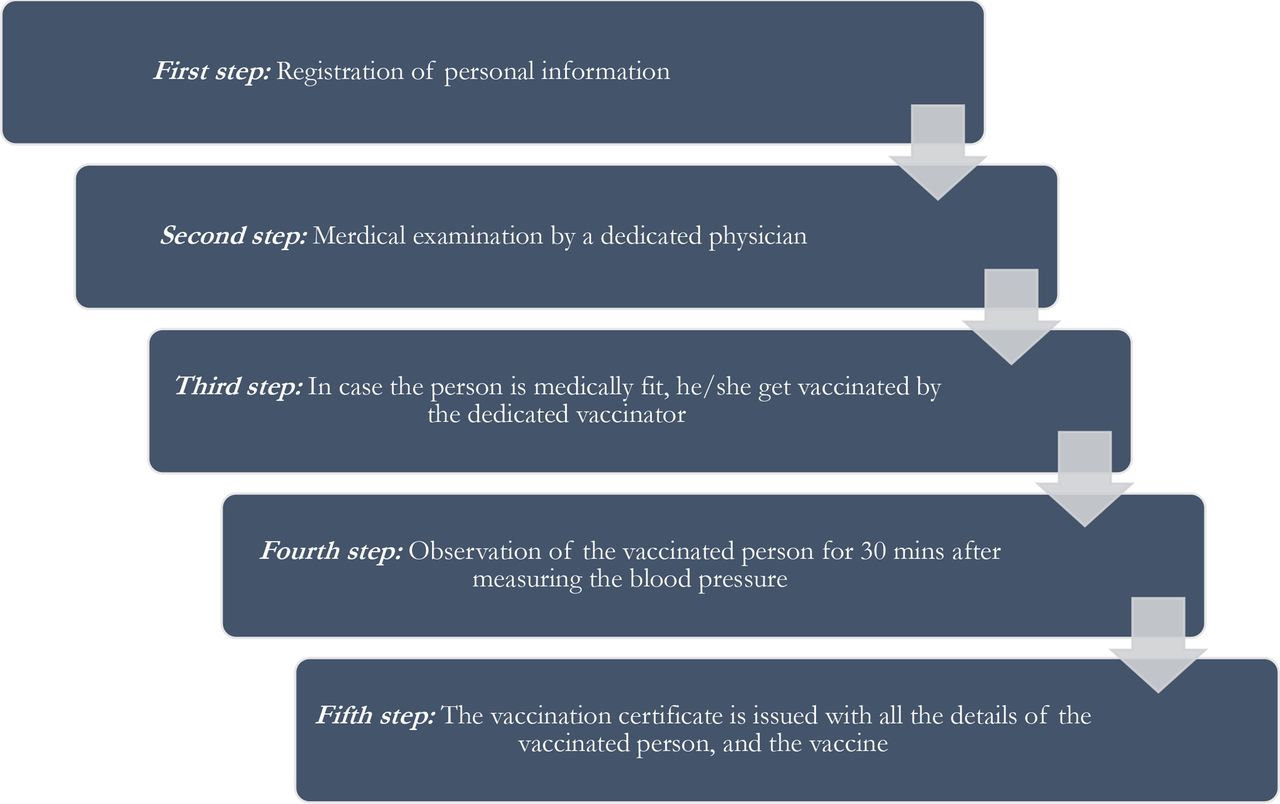
During the first phase of the vaccination campaign, the government installed three major vaccinodromes in the capital, Djibouti-Ville, in three different major districts and these vaccinodromes were equipped with all necessary trained human resources and equipment/materials including the needed cold chain for the vaccine safety. The algorithm (circuit) of the people visiting the vaccinodromes to get vaccinated in Djibouti was planned as shown in figure 5.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The algorithm (circuit) of the persons vaccinated inside the three vaccinodromes set up by the MoH for COVID-19 vaccination in Djibouti. MoH, Ministry of Health.
Risk Communication and Community Engagement
Following WHO COVID-19 pillar number 2, the MoH of Djibouti is developing a Risk Communication and Community Engagement (RCCE) plan for advocating the anti-COVID-19 vaccines in order to accelerate the vaccination process in the country. WHO and UNICEF are supporting the government in their effort to develop this plan and work together preparing a vaccination campaign that will follow the development of the RCCE plan.
The government is using vaccination and risk communication as the most important pillars for preparedness of the country to face the third wave that is expected with the beginning of the autumn season, September–October 2021, due to the return of all expats and nationals who usually spend the summer vacation abroad due to the very high temperature and humidity in Djibouti.
Lessons learnt from the COVID-19 pandemic in Djibouti
COVID-19 pandemic has proven that preparedness to health emergencies pays back. After the start of the pandemic, Djibouti quickly decided to enhance the laboratory capacity at the human and equipment levels in order to respond to get prepared to different respiratory outbreaks in a better way. Collaborations at all levels of society, different sectors and among the health workforce have been remarkable to achieve it.
Access to COVID-19 Tools Accelerator has been established to make vaccines, diagnostics and medicines available at the country level the fastest possible. Djibouti was the second country in EMRO Region to receive vaccines from the COVAX facility.18 COVID-19 pandemic has shown that health is interconnected with politics, economy and society; and that health systems can deteriorate and collapse rapidly.
The SARS-CoV-2 virus revealed the fragilities and vulnerabilities of the health systems globally, in the developed countries, as well as the developing ones. It taught us an important lesson that health is a major key for development, as a determinant of individual and collective growth, social cohesion and resilience. Health has a central position in supporting the achievement of the Sustainable Development Goals, with its seven accelerator themes, especially during times of emergencies and crisis, has proven that stronger intersectoral collaboration contributes to better health.21
In Djibouti, the front-line healthcare workers worked tirelessly, were overwhelmed and risked their lives in responding to the increasing need of the population during the pandemic. Essential health services faced a huge struggle to be continued in the country, especially during the first wave of the pandemic 2020. MoH overcame this struggle by redistributing the medical staff according to the essential health needs and coordinating with other sectors and ministries, as the Ministry of Defence and the Ministry of Interior, to restart most of the essential services during the following year, 2021.
Lives of Djiboutian people, same in the rest of the world, were severely disrupted as the government followed the global direction and took strict decisions to stay physically apart in order to reduce virus transmission.13 The population was asked to stay at home; many people lost their livelihoods and support networks. The Ministry of Solidarity and Social affairs of Djibouti, along with the UN system in the country, played a major role to support these families. The mental health consequences of these disruptions have been severe, and a longer-term impact is expected, as long as the pandemic continues.22
COVID-19 pandemic has also revealed the struggles that public health systems underwent to gain access to and share real-time epidemiological data on prevalence, health system performance, health workforce capacities, public health and social measures, procurement and supply chains of medical countermeasures, and other critical health metrics. It became clear that data, analytics and forecasting are key to informing evidence-based decisions during the pandemic, not only in Djibouti, but globally.23
Early preparedness, multisectoral and multicoordinated response, and the close collaboration with the WHO and other health entities and countries are among the major lessons learnt from Djibouti during the pandemic. The fact that Djibouti government used WHO’s COVID-19 Strategic Preparedness and Response Plan while developing the country’s National Plan for preparedness and response to the pandemic was of great benefit. It is important to take advantage of these lessons learnt in Djibouti and the world from COVID-19 pandemic, in order to embrace new ways of thinking and take actions rapidly to improve resilience in all levels of society, for COVID-19 and for upcoming expected health emergencies.
Conclusion
In this paper, we describe how Djibouti was hit by two waves of the COVID-19 pandemic over two consecutive years, with the second more aggressive wave with higher morbidity and mortality rates. A National Plan for COVID-19 vaccines deployment was developed and the country was one of the first in the region to receive batches of vaccines through the COVAX facility. A vaccination campaign was launched by the President of the Republic in March 2021, when approximately, 1.6% of the population were vaccinated in only 2 months’ time.
The government of Djibouti, specifically the MoH, spent a huge effort to respond to the COVID-19 pandemic and its two waves in the most adequate way, within the available resources in the country. The focus of the MoH is to follow mainly two pillars of the response strategy developed by WHO, 2 (RCCE) and 10 (Vaccination), in order to support the country to face the third expected wave of the pandemic in the country and respond adequately.
Data availability statement
Data are available in a public, open access repository. All data belongs to the MoH of Djibouti and it is available in the daily pubic communiqué of the ministry.
Ethics statements
Patient consent for publication
Footnotes
Handling editor Seye Abimbola
Twitter @DrElhakim
Contributors All authors contributed equally to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.