Article Text

Statistics from Altmetric.com
Summary box
Available evidence indicates that children and adolescents can transmit SARS-CoV-2 infection and are also vulnerable to severe disease and death.
There has been recent acceleration in approvals, initiation and scale-up of COVID-19 vaccination among children under 18 years in high-, low- and middle-income countries around the world.
Current data indicate that children in African countries also experience COVID-19-related morbidity and mortality, which may be worse than that of their counterparts in other regions of the world.
In this article, we outline the global status quo on scale-up of safe and effective COVID-19 vaccines for younger populations, and make an argument for why African children and adolescents should also be targeted for vaccination.
Introduction
Since the onset of the COVID-19 pandemic in December 2019, scientists have worked expediently to develop effective treatments and vaccines for clinical management and prevention of COVID-19. Drugs such as remdesivir, dexamethasone and, more recently, molnupiravir have had modest to impressive results in reducing risk of hospital admission, time to discharge, morbidity and/or mortality.1–3
COVID-19 vaccine development and evaluation in clinical trials has been rapid, with safe, effective vaccines being available within 12 months into the pandemic. There are several RNA, DNA, viral vector, inactivated and protein subunit COVID-19 vaccines approved for use.4 Table 1 shows the most widely used approved vaccines across each vaccine type.5 None of these vaccines are currently manufactured in any African country; however, participants in a few African countries have been enrolled in adult and, more recently, paediatric trials for these vaccines.4 6 7 Global, equitable access to safe and effective vaccines for all age groups is critical to ending the COVID-19 pandemic.
Major COVID-19 vaccines approved by at least one country, and paediatric age indications*
African countries that have approved COVID-19 vaccination for children and adolescents*
Global COVID-19 vaccine approvals for children and adolescents
There is evidence, mostly from high-income countries, to show that children and adolescents under the age of 18 years (hereafter referred to as ‘children’) can acquire and transmit SARS-CoV-2 infection and experience severe COVID-19, including multisystem inflammatory syndrome in children (MIS-C) and Long COVID-19 syndrome.8–10 Globally, children under 5 years of age represent only 2% of reported COVID-19 cases and 0.1% of deaths, whereas 5–14 year-olds represent 7% and 0.1%, and 15–24 year-olds represent 15% and 0.4% of cases and deaths, respectively.8 However, available data indicate that infants under 1 year of age have disproportionately high mortality,10 and adolescents and young people are increasingly representing higher proportions of the COVID-19 case load.11 Currently, six widely used COVID-19 vaccines have received emergency use authorisation or full approval for children under 18 years of age in at least one country12–19 (table 1). These include the USA’s Pfizer-BioNTech and Moderna (approved outside the USA) vaccines for adolescents ≥12 years of age,12 14 Pfizer-BioNTech vaccine for 5–11 year-olds,13 China’s Sinovac and Sinopharm vaccines for 3–17 year-olds16 18 and India’s Covaxin for children as young as 2 years old15 (table 1). At the time of writing, full vaccination is considered as receiving the one (Johnson and Johnson) or two dose (all others) primary series of currently available first generation COVID-19 vaccines.20 To date, 10 vaccines have been approved by the WHO for emergency use listing in adults,21 six of which have approval for paediatric indication in at least one country (tables 1 and 2). Consequently, COVID-19 vaccine coverage for children is rising in some countries; in the USA, for example, 53% of 12–17 year-olds were fully vaccinated and 25% of 5–11 year-olds were partially vaccinated by early January 2022. 22 By that same time point, population-wide full vaccination rates in high-income countries have reached approximately 60%–90%,4 and third dose boosters are being scaled up for adults and more recently, adolescents 12 years and older in some countries.23
The case for COVID-19 vaccination among children in African countries
As has been for adults, the COVID-19 vaccination situation is quite different for children in African countries, vis-à-vis globally. Currently, most of the countries with the highest rates of full COVID-19 vaccination in Africa are island nations or in Northern Africa, for example, the Seychelles (79%), Mauritius (72%), Morocco (62%), Tunisia (50%) and Cabo Verde (46%) .4 In a recent position statement, the WHO acknowledges that the majority of evidence in COVID-19 among children is from high-income countries, and recommends that ‘countries should consider the individual and population benefits of immunizing children and adolescents in their specific epidemiological and social context when developing their COVID-19 immunization policies and programs’.8 This recommendation thus puts the onus on countries to conduct their own local research to guide decision-making on paediatric COVID-19 vaccination policy. Steep inequity in access to vaccines and low rates of vaccination in high-risk adult populations need to be considered vis-à-vis vaccinating overall lower risk paediatric populations in Africa. However, benefits to vaccinating children include minimising school closures, the academic and psychological impacts of disruptions in education and intergenerational transmission.8 24 Moreover, children in African countries also bear high burdens of both communicable (eg, HIV, tuberculosis) and non-communicable diseases (eg, sickle cell disease, asthma), which would render them at risk for higher morbidity and mortality if coinfected with SARS-CoV-2.24 To date, only 11 African countries have approved COVID-19 vaccination among children under 18 years of age25 (table 2 and figure 1).

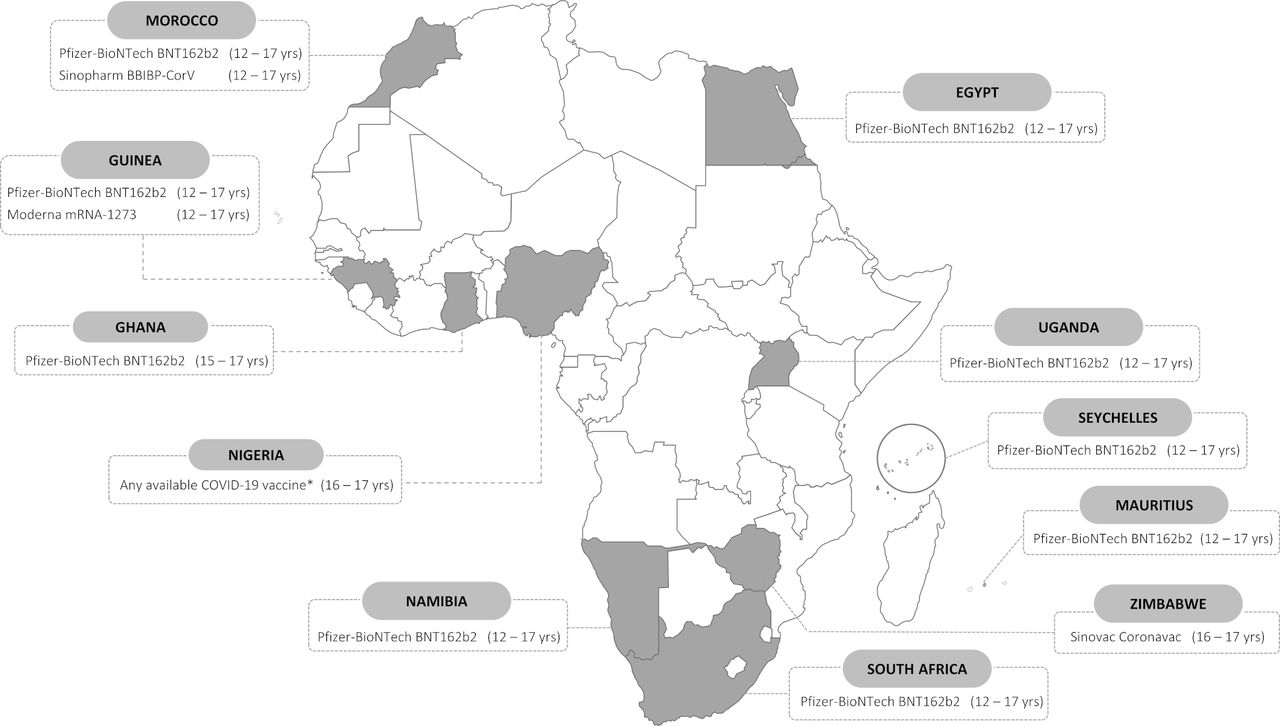{kind=link}
African countries with local approval for paediatric COVID-19 vaccination, age indications and vaccine types approved. Data as of 14 January 2022. * Nigeria has granted waivers for 16 and 17 year olds to receive any COVID-19 vaccines available at vaccination centers, for educational and international travel purposes. See table 2 for details.
The African Forum for Research and Education in Health (AFREhealth) COVID-19 Research Collaboration on Children and Adolescents recently published results of a retrospective study conducted in six African countries. This study included 469 children and adolescents aged 3 months to 19 years hospitalised between March and December 2020 in East (Kenya, Uganda), West (Ghana, Nigeria), Central (Democratic Republic of the Congo) and Southern Africa (South Africa).26 Approximately 25% of children presented with comorbidities; 3.8% were suspected or confirmed to have MIS-C, and 39 (8.3%) died in hospital. Among the children who died were 22 (32%) of the 69 children admitted to the intensive care unit (ICU), and 4 (22%) of the 18 with suspected/confirmed MIS-C.26 In multivariable ordinal logistic regression, factors independently associated with severe outcomes (oxygen requirement, ICU admission, mechanical ventilation and death) were age <1 year, hypertension, chronic lung disease and haematological disorders.26
This new evidence helps to address a pressing need for data to guide policy and practice for COVID-19 in African countries.27 The AFREhealth study provides multicountry, multiregional evidence of relatively high mortality rates among hospitalised children with COVID-19. Mortality in the AFREhealth study was 8.3%,26 severalfold higher than paediatric case fatality rates of 0.24% (in low and middle-income countries) and 0.01% (in high-income countries) reported in a systematic review by Kitano et al,10 and still higher than the global average of 0.1%–0.4% reported by the WHO.8
The wide differences seen in paediatric COVID-19 case fatality rates between lower resource African settings and high-resource settings have also been seen among adults, as demonstrated by the high (~50%) mortality among critically ill adult patients with COVID-19 in the African COVID-19 Critical Care Outcomes Study.28 These findings infer the significant role that health infrastructure—or lack thereof—plays in modulating COVID-19 case fatality rates beyond the pathogenicity of circulating SARS-CoV-2 strains. The emerging evidence supports our call for African countries—especially those with the least resourced health infrastructure—to prioritise disease prevention and galvanise efforts to scale up COVID-19 vaccine supply and uptake, including among children. With its relatively young population, the African continent cannot achieve herd immunity without vaccinating children.
Considerations for inclusion of children and adolescents in vaccine policy across Africa
While a case may be made for children to receive COVID-19 vaccines, policy making for African countries has to be made in consideration of unacceptably low adult vaccination rates in the setting of global inequities in accessing vaccines, poor risk communication and under-resourced health systems. As of 8 January 2022, full COVID-19 vaccine coverage across Africa was 9.6%, with approximately 52% of countries still below 10% coverage.29 Clearly, the WHO’s modest targets of 40% full vaccine coverage for all countries by the end of 2021 was not met, and the 70% target for June 202230 will likely not be attained for much of the continent. The emergence of the SARS-CoV-2 Omicron variant, first reported to WHO by South Africa on 24 November 2021,31 is likely to further delay the achievement of these targets by potentially redefining ‘full coverage’ in necessitating boosters for adequate protection.32 As of 13 January 2022, thirty African countries had detected Omicron, out of 142 countries reporting this new variant globally.33
To date, only a few African countries have approved paediatric COVID-19 vaccination, thus vaccine roll-out for children will continue to lag behind that of adults for much of the continent. For children who may not be targeted for vaccination at the same time as the rest of the population, at a minimum, we propose prioritisation similar to that for adults early in vaccine roll-out: those at highest risk of severe disease and death, and older adolescents (who are more likely to transmit infection)8 living with high-risk adults should also receive vaccines. Thus, high-risk children in African countries should be prioritised for COVID-19 vaccination regardless of their age; this population includes children with hypertension, chronic lung disease and haematological disorders, as reported by the AFREhealth study.26 Paediatric COVID-19 vaccination can be prioritized using risk stratifications according to presence and number of comorbidities, and cohabitation or close contact with high-risk adults. Likewise, healthy adults living with and/or caring for high-risk children should also be encouraged to get vaccinated; this includes healthcare workers. Our recommendations are in line with an analysis from the Africa Centres for Disease Control and Prevention, which indicates that reaching 70% vaccine coverage for nearly all African countries will require inclusion and vaccination of children at least 10 years of age.34
Conclusion
New, locally generated evidence indicates that COVID-19-related morbidity and mortality among children and adolescents in African countries may be much higher than among their counterparts in other regions of the world. The advent of the rapidly spreading Omicron variant and its as-yet unknown impact across Africa and among children is of additional concern. It is important to scale up the generation of rigorous local evidence across Africa through collection and reporting of national-level, age-disaggregated epidemiological data and the design and implementation of observational and interventional studies focused on paediatric COVID-19. Vaccination with currently available vaccines continues to be recommended for the eligible who can access them. Given the emerging evidence of paediatric vulnerability to severe COVID-19, it is imperative that policy makers and public health institutions include African children in their COVID-19 vaccine guidelines and procurement planning, especially for those at highest risk of severe disease and death. While COVID-19 vaccines are a game-changing public health tool, until the pandemic is under epidemic control, basic infection control methods such as mask wearing, hand sanitisation, good indoor ventilation, and physical distancing must be concurrently observed.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
NAS-A acknowledges support from US National Institutes of Health (NIH) National Institute of Child Health and Human Development grant #R01HD089866 (Adolescent to Adult Patient-Centered HIV Transition, Nigeria), and NIH Fogarty International Center (FIC) award through the Adolescent HIV Prevention and Treatment Implementation Science Alliance (AHISA), for the Central and West Africa Implementation Science Alliance (CAWISA). Sir Prof. AZ acknowledges support from the European Union EDCTP-funded PANDORA-ID-NET, the Central African Network on Tuberculosis, HIV/AIDS and Malaria (CANTAM-3); and the East Africa Consortium for Clinical Research (EACCR-3). AZ is a Mahathir Foundation Science Award and Pascoal Mocumbi Prize laureate. JBN is supported by NIH/FIC grants 1R25TW011217-01 (African Association for Health Professions Education and Research); 1R21TW011706-01 (Cardiometabolic Outcomes, Mechanisms, and Approach to Prevention of Dolutegravir Associated Weight Gain in South Africa); and 1D43TW010937-01A1 (University of Pittsburgh HIV Comorbidities Research Training Program in South Africa); as well as NIH/NIAID grant No. U01 AI096299 (Central Africa-International epidemiology to Evaluate AIDS (CA-IeDEA).
Footnotes
Handling editor Seye Abimbola
Twitter @NASAdoc, @nkquakyi, @bronchigirl, @AliZumla
Contributors NAS-A and JBN conceptualised the manuscript. NAS-A and NKQ drafted the manuscript and collated the data. All coauthors provided substantial contributions in terms of critical revision of the draft, and reviewed as well as approved the final version submitted for publication.
Funding US National Institutes of Health/Fogarty International Center Grant No. 1R25TW011217-01 to the African Forum for Research and Education in Health (AFREhealth); Principal Investigators: Prisca Adejumo, Jean B. Nachega, Nelson K. Sewankambo, and Fatima Suleman.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.