Article Text

Abstract
WHO launched the Good Governance for Medicines (GGM) programme in 2004 with the aim of fighting the problem of corruption in the pharmaceutical sector. Zimbabwe adopted the GGM programme in 2015 and developed its own implementation framework (GGM-IF) in 2017 based on the WHO global guidelines and recommendations. Zimbabwe’s GGM-IF emerged from; (1) home-based expertise, (2) extensive local consultations and (3) effective incorporation into existing institutions. The GGM-IF committed to implementing a focused programme over a 5-year period from 2017 to 2022 with the expressed goal of improving transparency and accountability in the pharmaceutical sector as a key enabler to improve access to medicines. Midway through its projected lifespan, some notable achievements materialised attributed to key success drivers, including mutual collaboration with the Ministry of Health and Child Care’s existing Global Fund supported Quality Assurance Programme. Key challenges faced include limited funding for the programme, a shifting policy environment driven by a political transition and reorientation of priorities in the wake of the COVID-19 pandemic. This manuscript articulates 3-year operationalisation of Zimbabwe’s GGM-IF highlighting the success drivers, implementation challenges and lessons learnt.
- health systems
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
In 2015, Zimbabwe adopted the Good Governance for Medicines (GGM) initiative with the aim of improving transparency and accountability in the pharmaceutical sector within the context of access to medicines.
Despite a bold commitment and high level endorsement for the initiative, several milestones contained in a 5-year national implementation framework were missed.
The main challenges faced include limited funding, a shifting political and policy environment and a crisis-laden environment geared towards alleviating urgent health problems including the COVID-19 pandemic.
GGM actors developed innovative coping strategies to address technical challenges in the short-term while lobbying for political attention to sustain a long-term strategy.
As fighting corruption in health systems is increasingly being recognised as an important and attractive investment in the context of Universal Health Coverage and Sustainable Development Goals, an opportunity exists to mobilise and align technical and political resources to bolster the implementation of GGM.
Introduction
Corruption has been associated with bad governance, weak health systems, violation of human rights and singled out as a major threat for attaining Universal Health Coverage (UHC).1 The pharmaceutical system is particularly vulnerable to inefficiencies and losses from corruption, which severely compromises access to safe, effective, good-quality medicines and undermines public interest.2 3 The dimensions associated with health governance include: participation, rule of law, transparency, accountability, equity, efficiency and effectiveness, responsiveness, consensus orientation, health orientation, and decentralisation.4 WHO launched the Good Governance for Medicines (GGM) programme in 2004 as an innovation aimed at curbing the loss of health resources by promoting transparency and accountability.5 GGM specifically seeks to safeguard availability of medicines in participating countries by preventing corrupt practices at various levels of the medicines supply chain. By 2015, 38 countries, including Zimbabwe, had adopted the GGM concept.1 The roadmap towards achieving GGM involves a three-phase process.1 5 Phase I consists of a national assessment process where the level of vulnerability to corruption is determined using a WHO validated method. In phase II, a national GGM implementation framework (GGM-IF) is developed, based on findings and recommendations originating from phase I. A successful phase II then leads to phase III where the country adopts the framework and operationalises the GGM-IF as a component of its major strategic policy thrusts.1 Globally, the GGM has been promoted as an innovative approach to prevent corruption in the pharmaceutical sector within the context of UHC.6 Since its inception the GGM has gone under several evaluations either as a standalone initiative or as part of evaluations that focus on various initiatives aimed at improving governance in the health sector.7 8 A number of lessons have been documented from these evaluations, ranging from the technical prerequisites to the political determinants of its success. In the Africa region, the GGM methodology has been adapted and applied to assess governance for critical cross-cutting issues affecting the pharmaceutical sector including medicines protection and rational use.9 In general, the implementation of good governance initiatives varies despite the presence of internationally recognised principles and approaches hence it is essential for countries to recognise and identify models of good governance within the context of domestic history, culture and values.10
Zimbabwe’s GGM programme approach
Involvement in the GGM programme
In 2015, Zimbabwe’s GGM programme was spearheaded by the Ministry of Health and Child Care’s Directorate of Pharmacy Services (MoHCC-DPS) in partnership with the WHO Country Office. The phase I, national assessment was conducted by research consultants from the University of Zimbabwe Department of Pharmacy and Pharmaceutical Sciences’ Centre of Excellence for Pharmaceutical Innovation (COE-PI).11 Key findings from the widely consultative national assessment resulted in recommendations to proceed to phase II whose goal was to develop the GGM-IF.
Development of the GGM-IF
The same COE-PI team which conducted Phase I was appointed by the WHO Country Office as Consultants to facilitate the development of the country’s GGM-IF. A WHO-funded consultative workshop was organised for key stakeholders from the academic, public and private sectors, thus ensuring as much inclusion of local experts as possible. Held on 22 June 2017, the workshop included a resource expert from the WHO Headquarters in Geneva, Switzerland. The WHO GGM expert shared experiences from other GGM participating countries and assisted in reviewing the findings and recommendations from phase I. The consultative workshop engaged the participants in an exercise to identify Zimbabwe’s GGM goal and priority areas. The COE-PI consultants then took over the process and completed it with a consumer-based study as well as a series of consultations with individual key stakeholders. The GGM-IF was then presented for approval at another stakeholders’ workshop held on 22 September 2017.
Key features of the GGM-IF
The expressed goal of Zimbabwe’s GGM-IF was, ‘to improve public trust and confidence in Zimbabwe’s medicines supply system through transparent, accountable, equitable and sustainable provision of medicines.’ This goal would be met by adopting WHO’s revised GGM approach which emphasised two strategies for improving governance, namely the discipline-based as well as values-based system.
Execution of the GGM-IF
Continuing from Phase I and II, the MoHCC-DPS assigned the University of Zimbabwe’s Department of Pharmacy and Pharmaceutical Sciences to operationalise the GGM-IF through the COE-PI. This ensured retention of local expertise throughout. The Framework committed to executing a focused programme over a 5-year period from 2017 to 2022 with the expectation of receiving dedicated funding as had happened for phases I and II. However, in November 2017, there was a political downturn, which resulted in the change of government and reprioritisation of public sector programmes. Subsequently the GGM-IF did not receive the anticipated dedicated funding support even though commitment to its implementation was already in place.
‘Dual Strategy’ implementation
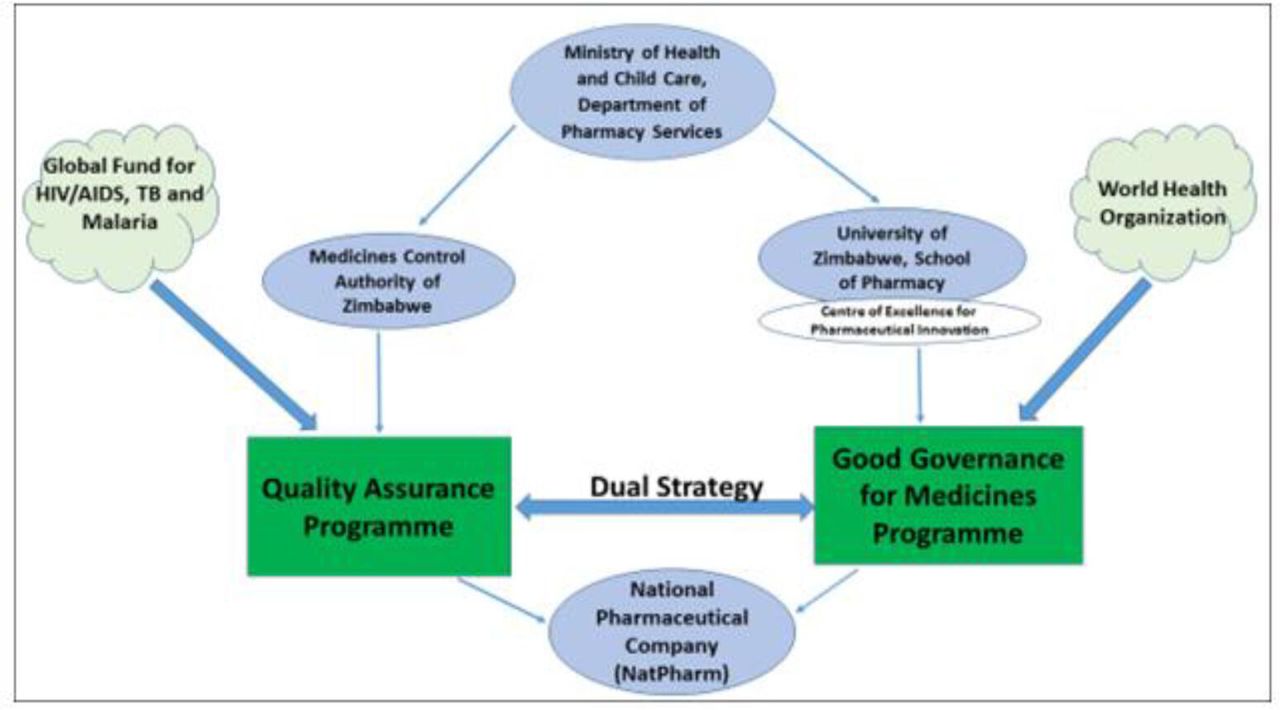
Figure 1 shows how the COE-PI has utilised a ‘dual strategy’ by integrating the GGM programme with the MoHCC existing Global Fund supported Quality Assurance Programme (QAP), which is being coordinated by the Medicines Control Authority of Zimbabwe (MCAZ). The Global Fund for HIV/AIDS, tuberculosis and malaria has supported the QAP since 2017. Its mandate is to improve quality of pharmaceutical service delivery by building the capacities of the MoHCC, MCAZ, the local schools of pharmacy and the National Pharmaceutical Company (NatPharm). Being the national pharmaceutical regulatory agency, the MCAZ is perfectly placed to anchor both the discipline-based and the value-based strategic goals. The schools of pharmacy mostly promoted the value-based system through training and advocacy.
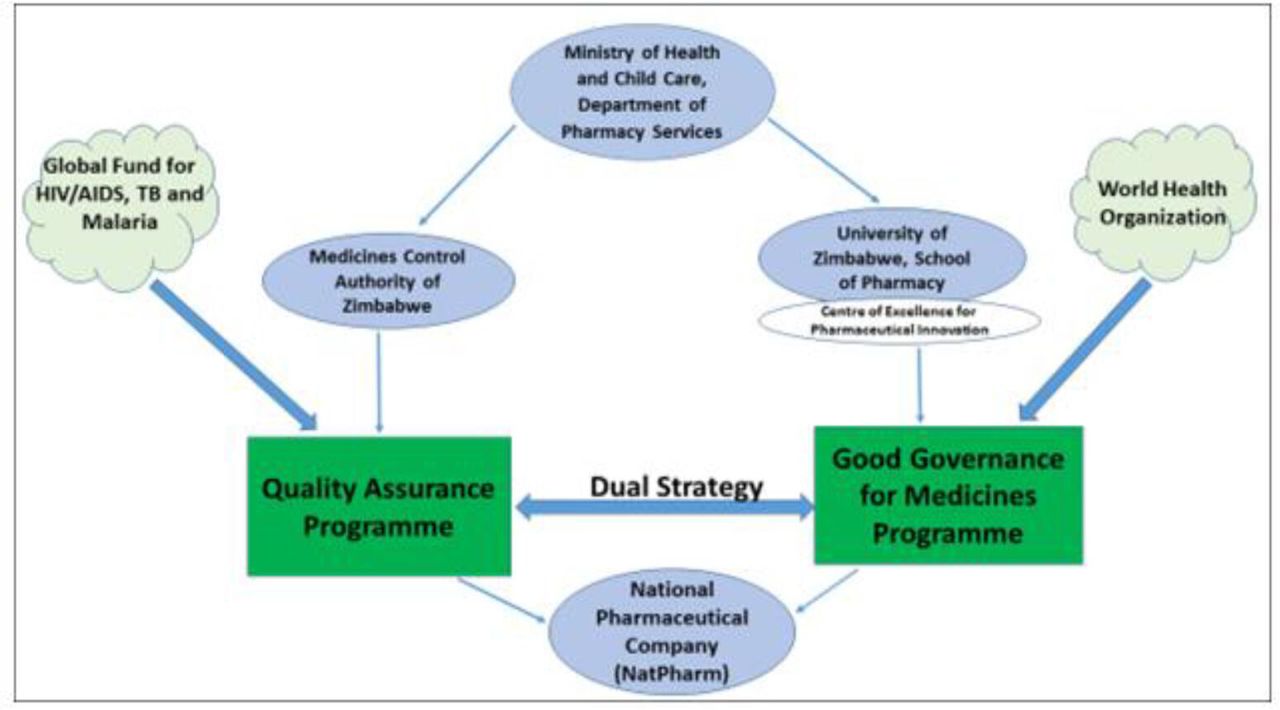
Zimbabwe’s GGM Framework GGM, Good Governance for Medicines; TB, tuberculosis.
Notable outputs from Zimbabwe’s GGM programme and cross cutting innovations to sustain it
Strengthening academic-public-private sector partnerships
The initial 3 years of operationalisation of the GGM-IF, produced key outputs shown in table 1 above.
Notable outputs of Zimbabwe’s Good Governance for Medicines (GGM) programme
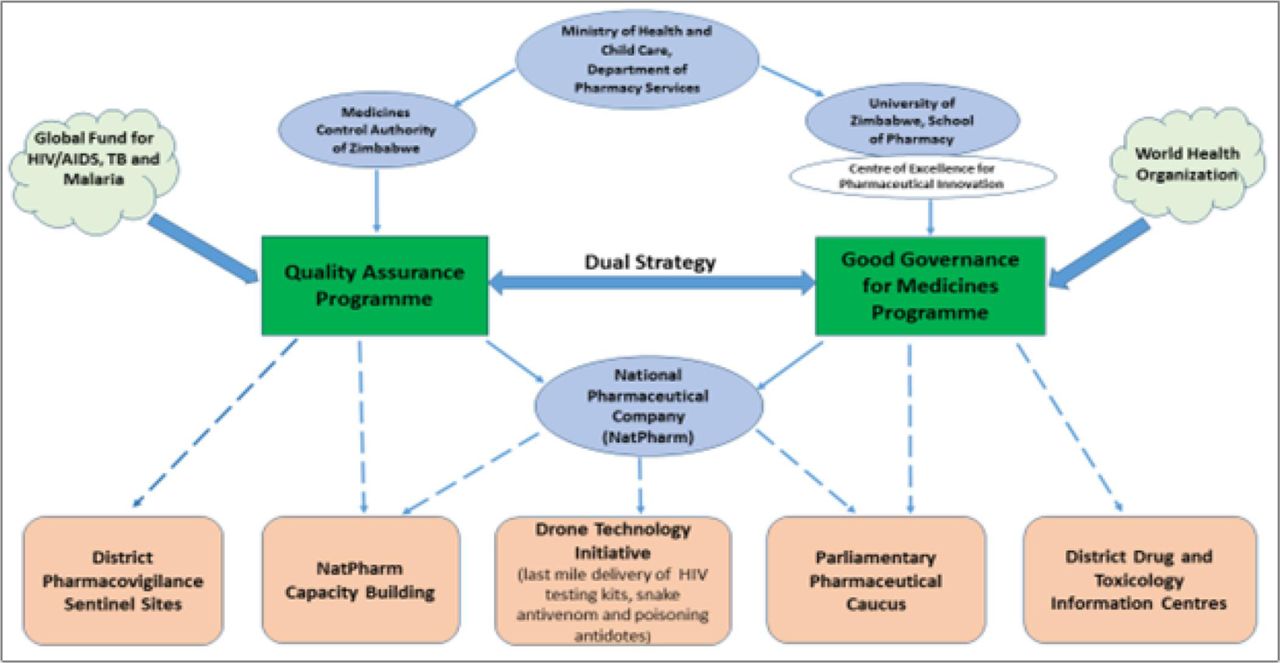
The first output was the catalytic enhancement effect that the programme had on the COE-PI. COE-PI had been designed to strengthen academic-public-private sector partnerships. Its involvement in the GGM programme strategically positioned the contribution of the COE-PI towards ensuring equitable and sustainable access to good quality and effective medicines as shown in figure 2. Operationalisation of the GGM-IF through the dual strategy has achieved several noble outcomes shown in figure 2, although with limited resources. COE-PI also operates the University of Zimbabwe International Pharmacology Specialty Laboratory which carries out pharmacovigilance studies in collaboration with the MCAZ.12 Through its participation in QAP planning and coordination meetings, COE-PI has developed a training programme for traditional health practitioners to improve the quality of complimentary medicines. In collaboration with NatPharm, plans are underway to introduce unmanned aerial vehicles (drone technology) for efficient delivery of antidotes, vaccines, and HIV and COVID-19 test kits to remote areas of the country.

{kind=link}
{kind=link}
Zimbabwe’s GGM framework and notable outputs. GGM, Good Governance for Medicines; TB, tuberculosis.
Incorporation of GGM into pharmacy curricula and motivation for the establishment of district drug information centres
A sustainable value-based programme that incorporates issues of governance and ethical practice has been incorporated into the undergraduate and postgraduate curriculum for pharmaceutical personnel at the University of Zimbabwe. Since 2017, training components incorporated into the Clinical Pharmacy course that is undertaken by undergraduate pharmacy students in their third year. The course equips students with skills in providing cognitive services in addition to regular dispensing duties. The course incorporates, ‘How to set up district drug information centres’, and practical sessions on, ‘Live Query’ answering. Three student streams have been taught and two of them have already graduated. Soon after introducing the course, COE-PI began to motivate for setting up of drug information centres at district level throughout the country. As such, there is a readily available pool of qualified personnel that can run these drug information centres in all districts throughout the country. The postgraduate masters in applied pharmaceutical sciences includes; pharmaceutical formulation, manufacturing, and pharmaceutical regulatory affairs.
Linkages with emerging priorities in the therapeutic and policy environment
With the increasing demand for complementary and alternative medicine, the need for clearer understanding of herbal therapies has increased.13 Advancement of advocacy for herbal therapies thrives through formation of the Natural Therapist Council of Zimbabwe (NTCZ). COE-PI has been a key participant in the NTCZ board. This promotes the progress of GGM implementation while raising awareness on the GGM initiative throughout the health delivery system in the country.
Creation and establishment of the Parliamentary Pharmaceutical Caucus
To facilitate political petitioning, COE-PI conceptualised and advocated for the establishment of a Parliamentary Pharmaceutical Caucus (PPC). Among other aims, the PPC terms of reference include; (1) campaigning for transparency in the medicines supply chain at different levels of healthcare, (2) advocating for equal access to essential medicines as part of health service provision and (3) ensuring a culture of regulatory compliance within the pharmaceutical sector. COE-PI serves as the secretariat which manages the day-to-day affairs of the PPC. So far, the PPC members have led the Parliamentary Portfolio Committee on Health and Child Care in conducting an assessment of the pharmaceutical sector which produced a report. The report was subsequently debated in the National Assembly to come up with a number of resolutions which include; recommendation for the unfreezing of district level pharmacists posts in the MoHCC by the end of 2019.14 Recommendations were also made for comprehensive capacity building at the NatPharm.
GGM challenges and strategies to address them
Among the originally planned activities, there are several missed targets as shown in the Gantt chart presented in table 2, which was prepared as part of the GGM-IF. These include lack of funding, limited engagement of stakeholders and a shifting policy and political environment. The major missed target was the failure to secure development partner funding. This occurred due to the political transition following the change-over of government in 2017 and the subsequent emergence of COVID-19 which resulted in the reprioritisation of MoHCC programmes. Fresh negotiations between the Government and its development partners resulted in the exclusion of funding for the GGM Programme. In response, GGM activities were mapped according to funding needs followed by a stakeholder analysis to identify potential funders outside the government and the traditional developmental funders. Following a strategic analysis of the resource needs and the potential attractiveness of GGM activities among stakeholders, funding was secured from a private pharmaceutical wholesaler to revitalise some key activities. A key factor in promoting GGM is availability of political will. At the macro level, there was a delay in political petitioning between from September 2017 to September 2018. Despite the delay, GGM actors maintained a critical awareness of the sociopolitical environment and its influence on GGM which culminated in the creation of the PPC through collaborative lobbying with newly elected parliamentarians from the pharmacy profession.
GGM Activities Gantt chart showing achieved and missed targets
The WHO recommends using both discipline-based and value-based approaches in implementing GGM. Zimbabwe’s GGM-IF intended to achieve this by combining the efforts of MCAZ and other regulatory agencies such as the Zimbabwe Republic Police, the Department of Customs and Excise and the Zimbabwe Anti-Corruption Commission to provide adequate workforce for inspections and other issues pertaining regulation of medicines. So far, while the MCAZ is closely involved, other agencies such as the Health Professions Authority, and the national law-enforcement agents are still to be included. Advocacy, monitoring and evaluation were also delayed due to policy changes at the MoHCC. These targets are considered as partially achieved since they were only carried out using limited internal COE-PI resources. Incorporation of GGM into research and teaching curricula is considered partially implemented because it has so far only benefited the University of Zimbabwe’s pharmacy students. GGM should ideally be included in pharmacy programmes at other institutions and other health professions.
Lessons learnt
Overall, the key lesson learnt from GGM implementation in Zimbabwe is that it requires a multi-sectoral approach and an appreciation of the critical role that politics plays in public health affairs. As documented elsewhere, clearer understanding of the political dimensions of health policy by public health professionals in government, advocacy groups, and research organisations is necessary for designing more effective policies and programmes.15 GGM in Zimbabwe started with implementation of aspects within the predominant remit and mandate of technocrats such as curriculum design and quality assurance before approaching state level institutions such as parliament to seek audience for wider reforms. Key-specific lessons learnt include (1) the importance of academic-public-private partnerships (PPPs), (2) policy consciousness to generate context-specific innovations to attain quick wins and (3) the importance of political lobbying to generate attention among national leaders.
Regarding PPPs, the dual strategy of combining QAP and GGM programmes strengthened academic-PPPs and collaborations. Such a partnership is not a novel concept, commonly observed in developed countries and has been linked to supporting SDGs, implementation of primary healthcare, effective regulation of medicines and pharmaceutical innovation at global level.16–20 The strengthened PPPs in Zimbabwe facilitated the mobilisation of funding from the private sector when the government and traditional development funders could not commit resource to GGM. Another key lesson learnt is that while GGM requires increasing amounts of funding throughout its lifespan, generation of context-specific innovations facilitates attainment of low-cost quick wins to lay the foundation for long-term implementation. In this vein, Zimbabwe has demonstrated adequate capability to implement its GGM-IF, with success in training, QA and advocacy with limited funding. This was done through leveraging existing relationships within the dual strategy and taking advantage of the COE-PI’s reputation in teaching by incorporating GGM components into the pharmacy curriculum to reinforce the value based strategy. At policy level, advocacy was facilitated by the positioning of GGM within the context of emerging therapeutic developments under the newly established Natural Therapists Council of Zimbabwe (NTCZ) to resonate with the evolving policy landscape. However, financial support is vital for the continuation and further rolling out GGM activities. Another key lesson learnt is the importance of the political dimensions of the GGM to enhance political feasibility and sustainability. Although the process was slow and typical of institutional change, strategic lobbying between the GGM policy community and the newly elected pharmacist parliamentarians culminated in the positioning of GGM within the broader mandate of national pharmaceutical development being championed by the PPC.
Recommendations
The missed targets observed in Zimbabwe’s GGM programme were mostly due to changes in government priorities as well as the disruptive effects of the COVID-19 pandemic. However, the bottom-line issue was the lack of dedicated funding to support the GGM-IF. In this regard, the overall recommendation is that government and its development partners should provide funding to drive the country’s GGM programme. Such dedicated funding would not only ensure equitable and sustainable access to good quality and effective medicines, but also provide medicines in a transparent and accountable manner. Details of the challenges faced in the operationalisation of Zimbabwe’s GGM programme and the respectively suggested solutions are shown in table 3. In addition to securing dedicated funding support for the GGM-IF activity, other key recommendations include involvement of all necessary stakeholders, pursuing partner collaborations, introduction of GGM into the curricula at other health professional training institutions, adoption of digital platforms and GS1 standards to improve efficiency, as well as creating an advocacy team for GGM.
GGM challenges faced and suggested solutions
Given that governance for medicines lies at the interface of politics, public health and pharmaceutical science, further research is needed to understand how an interaction of these factors influenced the implementation of GGM in Zimbabwe.
Conclusion
After 3 years of implementation, the GGM programme has recorded some notable achievements although with limited resources and the changeover of Governments in 2017. In summary, the key success factors of the GGM-IF are that it emerged from home-based expertise, extensive local consultations and effective incorporation into existing institutions which created the unique ‘dual strategy’ feature of the GGM-IF and a platform for strengthened academic-public-private sector collaboration. However, it remains uncertain whether the intended goal and outcomes will be achieved over the set 5-year period particularly in the face of unpredictable funding and possible fluctuations in prioritisation with shifting political and policy priorities. An alignment of technical and political priorities is needed to bolster the much-needed implementation of the GGM initiative in Zimbabwe.
Ethics statements
Patient consent for publication
Footnotes
Handling editor Seye Abimbola
Twitter @nmadzikwa
Contributors CCM led the design, conduct and analyses of the manuscript. TC drafted the initial version of the manuscript. All the authors made a substantial contribution to the structure and content of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.