Article Text

Abstract
In 2010 the US-Affiliated Pacific Islands (USAPI) declared a regional state of health emergency due to the epidemic of non-communicable disease (NCD) and an NCD monitoring and surveillance framework was developed that includes adult NCD risk factor and disease prevalence indicators to be collected every 5 years using a population-based survey. On evaluation of existing data from adult population-based NCD surveys, it was found that there was a lack of valid, available and consistently collected data. Therefore, a new model was developed to combine various indicators and survey tools from different partner agencies into one survey. After the report was endorsed by local health leadership, a dissemination workshop was conducted. In 2015 (baseline for Hybrid Survey implementation), three out of nine jurisdictions (33.3%) had completed a population-based survey in the past 5 years. Four (44.4%) had no adult prevalence data at all, two (22.2%) had data sets from their surveys and four (44.4%) had at least two surveys ever collected that could be used for comparison. As of 2020, all nine jurisdictions have, or are in the process of completing an adult population-based survey. Eight (88.9%) have data sets from their surveys, and five (55.6%) have at least two surveys collected that can be used for comparison. This Hybrid Survey model has helped to improve adult NCD surveillance in the USAPI by more efficiently using limited resources. This model could be considered in other small island nations, or rural areas where adult NCD surveillance is challenging.
- community-based survey
- epidemiology
Data availability statement
There are no data in this work.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Non-communicable disease (NCD) surveillance among adults can be challenging in small island jurisdictions (such as the US-Affiliated Pacific Islands (USAPI) with limited epidemiological capacity, and historically there has been a lack of valid, available and consistently collected adult NCD data, and supporting multiple adult population-based surveys has not generally been successful.
The Hybrid Survey model combines various NCD indicators and survey tools from different partner agencies into one survey that can be owned and operated by the jurisdiction and supported by multiple partners agencies, thus making it a more effective use of limited resources.
The Hybrid Survey model has proven to be an effective way to improve adult NCD surveillance in the USAPI to collect more consistent and timely data while building epidemiological capacity.
The development of NCD monitoring and surveillance plans and buy-in from health leadership are important components that make this model a success.
Introduction
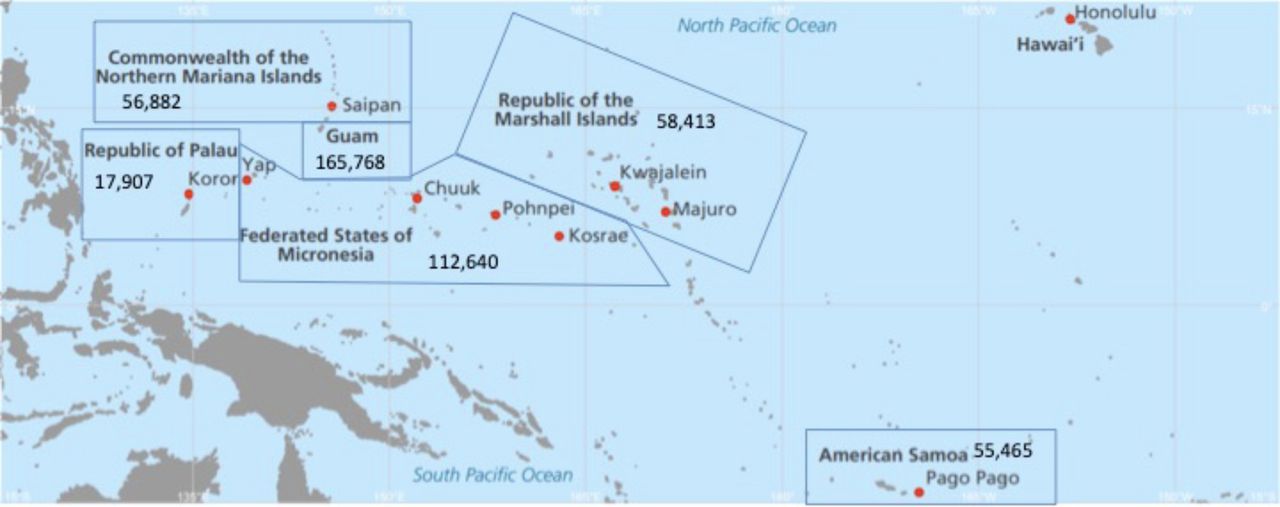
The US-Affiliated Pacific Islands (USAPI) are made up of three US territories (American Samoa, Commonwealth of the Northern Mariana Islands (CNMI) and Guam) and three freely associated states that are independent nations with compacts of free association with the US (Federated States of Micronesia (FSM), Republic of the Marshall Islands (RMI) and Republic of Palau). FSM has four culturally unique, geographically separated states (Chuuk, Kosrae, Pohnpei and Yap). The USAPI have a combined population of almost 500 000, ranging from 165 768 in Guam to 17 907 in Palau, and span about 1.5 million square miles in the Pacific Ocean1 (figure 1). The USAPI are eligible for certain US federal health support and funding, as well as international donor health support and funds and are therefore responsible for reporting certain health indicators to these support partners.
{kind=link}
Map of the US-Affiliated Pacific Islands with population sizes.
The Pacific Island Health Officers’ Association (PIHOA) is a non-profit organisation that is comprised of and is governed by USAPI health leadership. PIHOA’s mission is to improve the health and well-being of the USAPI by providing, through consensus, a unified credible voice on health issues of regional significance.2 In 2010, PIHOA Board Resolution #48–01 declared a regional state of health emergency due to the epidemic of non-communicable diseases (NCDs) in the USAPI.3 This is due to the high burden of NCDs throughout the USAPI.4–12 In 2012, an NCD Surveillance Framework was developed and endorsed by USAPI health leadership to identify core NCD indicators to be collected consistently across the USAPI for monitoring of NCDs in the region and evaluation of the NCD response.13
The PIHOA NCD Surveillance Framework requires routine collection of core NCD indicators from youth through high school surveys, from adults through population-based surveys, premature mortality rates due to NCDs from vital statistics and NCD core policy uptake monitoring.14 Core indicators from adults include use of tobacco, binge drinking, overweight/obesity (through physical measure), hypertension (through self-report and/or high measured blood pressure), diabetes (through self-report and/or measured high fasting blood glucose) and high cholesterol (through biochemical measure).13 These adult population-based surveys are to be conducted every 5 years.
The establishment of the NCD Surveillance Framework brought to light the lack of available valid adult NCD data in the USAPI. Many of the USAPI did not have any baseline data on adult NCD risk factors and disease prevalence, and those that did had outdated data.15 Additionally, adult NCD data were not consistently collected across the USAPI, or even collected consistently from survey to survey within each individual jurisdiction. Similar to the other countries within the Oceania region, the USAPI consistently struggle with health data availability which inhibit accurate reporting and modelling, such as that used with the Global Burden of Diseases, Injuries and Risk Factors Study.16
The USAPI face significant health disparities, have much lower health spending per capita compared with the USA and have limited financial and health resources and service delivery infrastructure.17 18 Accordingly, these island jurisdictions have limited qualified and specialty-trained human resources and low epidemiological capacity.19 20 Additionally, the USAPI face unique health issues and risk factors such as betel nut chewing,21–23 and other lifestyle-oriented risk behaviours compounded by food insecurity, poor economic development and insufficient built environments to encourage healthier lifestyle behaviours. These reasons make fitting the US model of multiple adult population-based surveys (such as Centers for Disease Control and Prevention (CDC) Behavioural Risk Factor Surveillance System (BRFSS), CDC National Health and Nutrition Examination Survey (NHANES), Substance Use and Mental Health Services Administration National Survey on Drug Use and Health, etc) along with global NCD surveys (such as WHO STEPS) challenging. Additionally, there have been ethical issues around data ownership/sharing and long turnaround times for analysis and reporting with some of these surveys.24 Therefore, there was a need to develop a new, collaborative model for adult NCD surveillance that could pool resources from various support agencies to produce necessary NCD and other health indicators for US federal grants and global framework reporting using a single survey that produced locally owned data. These indicators are also critical to inform and fulfil wider Pacific commitments such as the Pacific NCD Roadmap, Pacific Islands Forum Leaders commitments in addressing the Pacific NCD Crisis and Healthy Islands Vision, as well as global commitments such as the Sustainable Development Goals.14 25–27
In an effort to improve and streamline adult NCD data collection in the USAPI, the Hybrid Survey model was developed, which combines questions and measurements from various existing surveys with similar sampling and data collection methodologies and brings together multiple partners to implement one single survey. This model includes a set of core indicators that are collected through standardised questions and measurements in each site’s implementation which allow for comparable data across the USAPI.
Hybrid Survey methodology
As a first step, NCD Monitoring and Surveillance plans were developed and endorsed in each USAPI to outline local NCD surveillance. In order to select NCD indicators for monitoring, existing NCD surveillance frameworks were reviewed.13 28
A 1 day NCD Hybrid Survey planning workshop was conducted in-country that involved local stakeholders interested in collecting and using NCD data. The goal of this workshop was to develop a Hybrid Survey project plan, project budget and survey instrument.
To develop a survey instrument, standard instruments with validated questions were reviewed such as BRFSS, NHANES and STEPS. Questions and measurements were selected that would fulfil local data needs and external reporting requirements. Core questions and measurements based on the PIHOA NCD surveillance framework were also maintained throughout the region to allow for regional comparisons. As needed, questions were adapted to be made more culturally appropriate, and some indicators were modified from global reporting standard to make them more practical for the region. These instruments were eventually piloted by staff, revised as needed and translated into native languages by a team of health and non-health community members and underwent rigorous review.
After the planning workshop, the project plan was presented to local partners and external support partners such as PIHOA, CDC, the Pacific Community (SPC) and WHO to determine how all budget items and technical support could be covered, thus further refining the project plan. The final project plan covered items such as sample size, sampling procedures, data collection methods, consent, surveyor recruitment, surveyor training, surveyor supervision, data processing, data cleaning, data analysis and dissemination.
To determine samples in each jurisdiction, households were first randomly selected from best available household listings. In some USAPI, remote outer islands had to be excluded due to small population size and lack of accessibility. After the household sample was selected, one adult (18 and older) from each household was randomly selected using Kish methodology.29
Approximately 6 months after the planning workshop, a required 4–5 day training workshop was held in-country for all surveyors. This workshop covered items such as sampling procedures, interview techniques, question-by-question review, physical and biochemical measurement protocols, electronic data collection and management skills on a tablet and participant health feedback. All items covered during the training were included in a comprehensive training guide used during the training workshop that was given to all surveyors. These training guides were adapted for each USAPI, but the core components remained the same for consistency across the region. External support partners and health staff from other jurisdictions who had already conducted a Hybrid Survey led the training workshop. This peer-to-peer training was an effort to further build capacity in the region.
An additional part of the survey preparation involved promotion of the survey and community education. To successfully get messages into the community, it was critical to involve local partners such as local, traditional and religious leaders in this process to ensure community buy-in.
Data collection began immediately following the training workshop and typically took about 6 months. Approximately 30 local surveyors were used in each USAPI, and generally two local survey coordinators provided leadership and oversight. All USAPI but CNMI (who used paper forms) used tablets to electronically collect and upload survey data. All surveys were conducted using a face-to-face survey questionnaire along with physical and biochemical measurements. Physical measurements conducted included height, weight and three blood pressure measurements. Biochemical measurements conducted included fasting blood glucose (in all USAPI except CNMI that used a random blood sugar) and total cholesterol measured on a point-of-care device.
All data collected were uploaded to a secure server, then downloaded and cleaned to develop a final data set and data dictionary. About 6 months after data collection was completed, a final report was produced with technical support from PIHOA. This report was then provided to local health departments for review and endorsement by local health leadership. Then, approximately 1 month after report endorsement, a 2-day dissemination workshop was held in-country with local stakeholders to present the data and train these individuals on how the data can be used to set health priorities and select certain strategies.
Strengths, weaknesses and lessons learnt were documented after each survey based on qualitative evaluations with the survey team and shared within the USAPI to modify methodology in other jurisdictions. Additionally, these evaluations will be considered when planning for the second round of data collection in all USAPI.
It should be noted that methodology differed slightly in Guam due to the fact that Guam already had a functional BRFSS. Therefore, in Guam, state-added questions were included at the end of the phone survey that asked participants to provide contact information in order to be called back for a follow-up survey. These individuals were then contacted, and an appointment was made to collect the participant’s height, weight, blood pressure, fasting blood glucose and cholesterol. These data were merged with the BRFSS phone survey data in order to estimate prevalence of chronic conditions and disease.
Impacts of the Hybrid Survey model on surveillance
In 2015 (baseline for the development of the Hybrid Survey model), three USAPI jurisdictions (Guam, Palau and Yap) out of nine (counting FSM states individually) (33.3%) had completed an adult population-based survey in the past 5 years. This includes Guam, whose survey relied only on self-report and lacked physical and biochemical measurements. Four (44.4%) of the USAPI jurisdictions (Chuuk, CNMI, Kosrae and RMI) had no adult NCD prevalence data at all in 2015. Additionally, only two (22.2%) USAPI jurisdictions (Guam and Yap) had data sets that they were able to access for their own analysis and only four (44.4%) USAPI jurisdictions (Guam, Palau, Pohnpei and Yap) had at least two comparable surveys to be able to assess trends over time (table 1).
Most recent adult population-based NCD surveys and selected characteristics in each USAPI in 2015 and 2020
In 2020, all nine USAPI jurisdictions had, or were in the process of collecting current adult NCD prevalence data. On completion of the Hybrid Survey in Yap, all USAPI jurisdictions will have objective NCD prevalence data based on physical and biochemical measurement rather than self-report of height/weight and hypertension/diabetes status that can under-report chronic disease. Additionally, eight out of the nine USAPI jurisdictions (all but Chuuk) (88.9%) now have data sets that they can access for local analysis, and five (American Samoa, Guam, Palau, Pohnpei and Yap) (55.6%) have at least two comparable surveys to evaluate trends (table 1). Additionally, turnaround times for results were greatly improved, though not quantified in this report.
Lessons Learnt
After 5 years of adopting the Hybrid Survey model, more USAPI have current adult NCD data with physical and biochemical measurements, are able to access their survey data sets for local analysis, have the ability to analyse trends and have faster turnaround times for data reporting after survey completion. This model has proved to be an effective and potentially sustainable way to collect adult NCD risk factor and disease prevalence data by allowing the USAPI jurisdictions to take control of their own NCD surveillance by first developing an NCD monitoring and surveillance plan, then designing their own adult population-based survey that works best given available resources. By using existing survey instruments and validated questions from multiple support partners, the USAPI can collect data that meets reporting requirements from various external partners, as well as meet local data needs using one survey.
In addition to the Hybrid Survey model being an effective method for improving NCD surveillance, it has also been an effective strategy for building epidemiological capacity which has been previously identified as a weakness in the region.20 Although support partners provide technical support, local staff members coordinate the survey and collect their own data. The staff members involved in these surveys have developed valuable skillsets to include sampling, interview techniques, data collection and management using tablets, physical and biochemical measurement techniques and increased overall health knowledge that have been used in other surveys within their own jurisdiction. Additionally, survey coordinators who have completed their own jurisdiction’s survey are then used as trainers in other locations during the survey training workshop. This model has developed a cadre of experienced survey coordinators in the region who are able to share resources and provide peer-to-peer training and support. This type of peer-to-peer education has proven to be effective within Pacific Islander communities when it comes to other issues such as diabetes management.30
Another important feature of this model is the timeliness of data availability and reporting, and data ownership and access to data sets for local analysis. Past adult population-based surveys were collected using paper forms, and the data entry process was often delayed. Additionally, when outside partners collected data previously, there was often long lag times in data reporting where a report was generally developed five or more years after data were collected, making the data outdated by the time that they could be used. The Hybrid Survey collected data using tablets, so the data could be uploaded and viewed in real-time, therefore eliminating the lengthy process of data entry. After data collection was complete, a survey report was developed in 3–6 months. Additionally, the cleaned data set and dictionary were given to the jurisdictions for use locally. Through timely data processing and report development, as well as local data ownership, local health departments were able to have tangible reward after the long, resource-intensive process of data collection.
After the Hybrid reports were prepared, 2 day data dissemination workshops were held to share the findings and train stakeholders and community members on how to use these data to identify priorities and inform public health action. These dissemination workshops were a critical part of this model, as oftentimes data reports from the region were previously never brought to the community, and if they were, most community members are intimidated by using data, or had never used data to set priorities and drive action. After these dissemination workshops, the Hybrid Survey data were used to review and revise national NCD strategic plans, monitor and evaluate progress on NCD action items and advocate for certain programmes or policies within the community. These dissemination workshops could potentially be useful after other large surveys in the region.
The biggest strength of the Hybrid Survey model is the collaboration, both within the jurisdiction and between the support partners. In small, resource-limited settings, population-based surveys can be challenging and consume many human and financial resources.31 Therefore, it makes sense to integrate various NCD-related and other health indicators from different departments locally and from multiple external partners into one comprehensive survey. This allows these small island jurisdictions to maximise available resources and drive their own NCD surveillance efforts. Changing the model from external partners conducting or recommending surveys locally, to local health departments modifying their own survey and reaching out to external partners for support has proven to be an effective model in the USAPI and has the potential to be used in other small, resource-limited areas such as other Pacific Island jurisdictions, as well as rural areas that often lack local data.
There are of course limitations to this Hybrid Survey model. Success may depend on a jurisdiction’s need and ability to reshape the NCD surveillance system. It is critical that an NCD surveillance plan be developed and agreed on for an NCD Hybrid Survey to be successful. Additionally, health department leadership support for this model is critical to ensure appropriate resources can be allocated.
There were also unforeseen challenges when implementing these surveys such as outbreaks and natural disasters that are common in the region. Therefore, the Hybrid Survey planning and implementation needed to be flexible. Also, there were issues of surveyor integrity that arose in some jurisdictions including falsification of data and taking convenient participants instead of the randomly selected individual. These were issues that needed to be carefully monitored by survey coordinators, and rigorous checks were put in place in some locations. These issues were closely monitored and limited as much as possible.
NCD surveillance data have been found to be limited in most low-income and middle-income countries largely due to lack of capacity to collect these data, despite increasing NCD burdens in these nations.32 In higher income countries, there are challenges around collecting and reporting data from rural and remote areas. Oftentimes NCD data from rural and remote areas are not accessible due to small samples, or estimates need to be used for these areas.33 34 Additionally, the Oceania region commonly gets consolidated with the southeast Asia and east Asia regions in global studies, making it difficult to highlight the specific health concerns of this region.35 Therefore, it is essential to have accurate, locally collected and reported health data in these small island nations. The next step for this work will be to publish the results from these USAPI Hybrid Surveys more widely.
Conclusion
Overall, the Hybrid Survey model has proven to effectively improve adult NCD surveillance in the USAPI by more efficiently using limited resources. Due to the success of the Hybrid Survey model in the USAPI, it could be considered in other small island nations, or rural areas where adult NCD surveillance is challenging.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to acknowledge the health leadership, health staff and survey participants in the US-Affiliated Pacific Islands.
References
Footnotes
Handling editor Seye Abimbola
Contributors All authors have contributed substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; AND Drafting the work or revising it critically for important intellectual content; AND Final approval of the version to be published; AND Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Author HC is the guarantor of this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographical or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.