Article Text

Abstract
Introduction Industries that produce and market potentially harmful commodities or services (eg, tobacco, alcohol, gambling, less healthy foods and beverages) are a major influence on the drivers of behavioural risk factors for non-communicable diseases. The nature and impact of interactions between public bodies and ‘harmful commodity industries’ (HCIs) has been widely recognised and discussed at national and international levels, but to date little is known about such interactions at local or regional government levels. This study aimed to identify and characterise actual and potential interactions and proposes a typology of interactions between HCIs and English local authorities (LAs).
Methods Five electronic databases covering international literature (PubMed, EBSCO, OVID, Scopus and Web of Science) were searched up to June 2021. We also performed online searches for publicly available, web-based grey literature and documented examples of interactions in an English LA context. We conducted a critical interpretive synthesis of the published and grey literature to integrate and conceptualise the data in the context of English LAs.
Results We included 47 published papers to provide the frame for the typology, which was refined and contextualised for English LAs through the available grey literature. Three categories were developed, describing the medium through which interactions occur: (1) direct involvement with LAs, (2) involvement through intermediaries and (3) involvement through the local knowledge space. Within these, we grouped interactions into 10 themes defining their nature and identified illustrative examples.
Conclusion Our typology identifies complex inter-relationships and characterises interactions between HCIs and LAs, with illustrative examples from English LAs. Drawn from well-established theories and frameworks in combination with contextual information on English LAs, this typology explores the LA perspective and could help local decision-makers to maximise population health while minimising negative impacts of HCIs.
PROSPERO registration number CRD42021257311
- Public Health
- Review
- Health policies and all other topics
- Health policy
- Prevention strategies
Data availability statement
Data are available on reasonable request. No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Increases in preventable non-communicable diseases are largely driven by the consumption and use of tobacco, alcohol, gambling and less healthy foods and drinks, produced by ‘harmful commodity industries’ (HCIs).
Public bodies often have complex and close inter-relationships with HCIs, but the manifestations of these interactions have not been characterised at regional or local government level in England nor elsewhere.
WHAT THIS STUDY ADDS
Our typology of interactions between HCIs and local government, intermediaries and the local knowledge space, acknowledges the perspective of local government in seeking interactions with the private sector for mutual benefit, which does not apply to interactions with HCIs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The typology identifies complex inter-relationships and could help inform commercial policies and further considerations for decision-makers in local government, their intermediaries and the local knowledge space on how to maximise population health and minimise negative impacts of HCI interactions.
Introduction
‘Harmful commodity industries’ (HCIs) are corporations that produce and market products and services such as tobacco, alcohol, gambling and unhealthy foods and beverages. Use of such harmful commodities is a major driver of the burden of preventable non-communicable diseases (NCDs), and HCIs have been identified as important vectors of the growth of NCDs.1–4 Addressing the commercial determinants of health (CDoH) is therefore a pressing public health priority.5 The jobs, revenue, technical and research expertise, and ability to exert corporate power provide HCIs with a powerful voice to shape public perceptions of health, science and policy.2 The power of HCIs in influencing and shaping public health policy at the national and international level is well established6–13 through strategies to engage, and influence the cultural, social, political and knowledge environments.6–8 13 Approaches across HCIs are largely coherent,14 including echoing tactics of lobbying, marketing and corporate social responsibility (CSR) strategies, among others.1 2 7 14 15 These activities all extend and amplify HCI impact and influence, by enhancing the desirability and acceptability of harmful commodities, challenging policy barriers, deflecting attention from harms and whitewashing tarnished reputations of HCIs.6
A tension exists between HCI activities to encourage consumption of their products and maximise profits, and public health measures to reduce the burden of NCDs.7 8 16 17 The controversial nature of interactions between HCIs and public health is well recognised and discussed,1 9 17–19 including tobacco, alcohol and increasingly food industries1 7–11 in a range of contexts; globally and transnationally,20 21 in low-income and middle-income countries (LMICs),22 23 national organisations,24 academic environments,25 social media platforms26 and on explicit policies.27 28 In addition, recent attention also recognises the gambling industry, which is associated with significant harms including suicide, poor mental health and financial harms.29–31 Partnerships with gambling industry-funded bodies raise similar concerns to other HCIs.32–34
There are 333 English local authorities (LAs) split into two tier (county and district councils) and single tier (unitary authorities, metropolitan districts and London boroughs) structures to determine the council responsibilities. Article 5.3 of the WHO Framework Convention on Tobacco Control (FCTC)35 provides a key example of implementation of regulatory safeguards to protect public health policy from the interests of the tobacco industry at different levels of governance, including LAs. LAs have a legal obligation to act according to the FCTC, which sets a defined line for regulatory safeguards and enables local tobacco policy implementation while protecting LAs from legal challenges.35 As per the Health and Social Care Act 2012,’ LAs in England are responsible for all the public services and facilities in a particular area and obligated to improve the health of their population and promote healthy communities (Health and Social Care Act, 2012; national Planning Policy Framework, 2012). The devolution of public services shifting from central to local government, offers LAs the power to be better aligned with, and increase their sensitivity to specific local areas and local community needs.36 Close relationships between LA actors and the private sector are important for many reasons. These include generating revenue for LAs, boosting local investments and developments, providing resources and expertise, and sharing risks in developments, allowing LAs to deliver their key functions and vital services. As such, complex and sometimes close, inter-relationships between LAs and HCIs might not be perceived differently from other business relations, on the assumption that the interactions are equally mutually beneficial.
The complex and close inter-relationships between public bodies and HCIs are well established, but the manifestation of such activities at a regional or local government level, has not been explored. In addition, while previous research mainly focuses on the activities and the influence of HCIs, little is known about interactions between HCI and public bodies, in which LAs seek involvement from HCIs. Little is known about the nature and extent of interactions between LAs and HCIs. Therefore, it is critical to develop a comprehensive conceptualisation of interactions that considers and explores the LA perspective to inform decision-makers and ensure protection of populations from the harmful effects of HCIs. Understanding these interactions is particularly pertinent in the current economic climate as LAs operate under increasing financial constraints, and their investment, efficiency and retrenchment strategies may increasingly involve HCIs in attempts to compensate for reductions in public funding over the past decade.37–39 This study aimed to develop a typology that could encompass all potential interactions between HCIs and English LAs. We had two specific objectives: (1) synthesise the published international literature and develop a typology of the potential ways HCIs and LAs interact and (2) contextualise and refine the typology through the identification of documented examples of such interactions at the LA level in England.
Methods
We adopted principles from critical interpretive synthesis (CIS)40 to guide the study methods. CIS is an approach explicitly oriented towards theory building through a dialectic process combining evidence and theory. Adopting a comprehensive critical narrative allowed us to integrate and interpret a diverse body of evidence into a coherent conceptual framework40 in a dynamic and iterative process. The protocol was registered with PROSPERO (CRD42021257311).
Public involvement
Five members of the public were involved throughout the research process, including methodological planning and contributing to data collection methods. Crucially, they contributed to the appropriateness of the study framing and language, essential for engaging non-public health practitioners and enhancing the practical usability of the research.
Reviewing the published literature
Although this study was not specifically a systematic or scoping review, we adopted a flexible systematic approach to our knowledge synthesis. We tailored and adapted the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (online supplemental table 1) to guide the methodology.41
Supplemental material
Search strategy
The search strategy was guided using previously identified key papers which draw on well-documented HCI activities.1 2 6 11 13 25 42–45 The search strategy was developed for use in PubMed, using existing reviews, which explored for example, conflicts of interest in public health,43 the commercial determinants of obesity44 and corporate-political activity (CPA) of the food industry,46 and combined these with common terminology, Medline Subject Headings (MeSH) terms and free text, including synonyms, substitutes and plurals, to increase the search specificity and sensitivity. The search strategy was pilot tested using previously identified key papers, then independently tested by a second reviewer (EPV) and adapted appropriately for each additional database (online supplemental table 2).
Articles had to fulfil the predefined study eligibility criteria with the inclusion of papers published in a peer-reviewed journal, written in English, referring to humans and designed to collate (review, frame, typify, classify, conceptualise) ways that HCIs engage with public health (table 1 and online supplemental table 3A). We included all settings, countries and contexts, including any level of governance, not restricted to specific actors or stakeholders. We excluded abstract only, non-peer-reviewed studies, opinion pieces and broad discussions surrounding the topic. We searched five electronic databases from their inception to June 2021 (PubMed, EBSCO (CIINAHL, Econ Lit), OVID (MEDLINE, EMBASE, Global Health, PsycINFO, Health Management Information Consortium), Scopus and Web of Science) and handsearched reference sections of key papers.
Study eligibility
Screening and selection
Database searches were managed using Covidence systematic review software (Veritas Health Innovation). Duplicates were removed. Using the study eligibility criteria (table 1), one reviewer (SM) screened all titles and abstracts and a selection of abstracts from this first screen were discussed with a second reviewer (EPV) to determine potential eligibility. Full texts from the agreed list of abstracts from this first screen were retrieved and screened independently, with reasons for exclusion tabulated and subsequently discussed to resolve disagreements (SM and EPV).
Dixon-Woods et al40 describe CIS as ‘interpretive’ because only relevant examples from the literature are synthesised. We included papers that presented additional novelty, presented a new framework, domain(s) or unique interaction(s), rather than including all of the relevant literature. Where multiple papers examined the same initiative and mechanisms, one was selected. We created a hierarchy to guide a systematic and purposive selection (online supplemental table 3B), using preidentified key papers, the emerging typology and principles of theoretical saturation.45
Data extraction
With input from the wider authorship and public and practitioner collaborators, we created a guiding extraction frame40 to direct data extraction, with both inductive and deductive interpretation to capture emergent concepts from the literature. Data extraction included reference details (eg, authors, year, study type, setting, field, industry), framing (terminology, classification, clusters, including figures), interactions/activities (nature, type, actors) and any associated relevant examples or contextual information. Although a formal quality assessment or ‘risk of bias’ assessment did not apply to our research, we maintained an ongoing critical orientation to the material selected.40
Data synthesis (typology development)
Guided by CIS principles,40 we synthesised key theoretical frameworks and taxonomies of previous efforts to describe, monitor and collate corporate interactions of industries, regarding public health. We gathered and coded fragments of text, grouped the codes into themes, used data charting,47 sifting and sorting, to simultaneously create and adapt the typology, organise higher-level categories and themes, and add further details based on the included studies.
Review and analysis of the grey literature
We conducted a review and analysis of the grey literature, to provide contextual information, including what, why, who and how the HCI interactions potentially manifest at the LA level,48 through searching targeted websites, online resources, relevant publicly available grey information and consulting experts. We aimed to find further domains and representative documented case examples of these interactions at English LA level, rather than a comprehensive assessment.
We used the typology developed for the above review to direct our search of grey information in a targeted way and capture examples relating to English LA interactions with HCIs. The typology was reviewed (by SM, EPV and MW), refined in consultation with the wider authorship, public and practitioner collaborators, and translated into a practical list of terms to inform the search and a preliminary list of documents (online supplemental table 4). We applied similar methods to systematic review search strategies and handsearching grey literature.49 50 Potentially relevant records were ‘bookmarked’ in the web browser (Google Chrome), and we then searched within each bookmarked website. Searches continued within an a priori pragmatic time frame of 3 months to the point of informational and document saturation.51
Results of the searches were screened online, and relevant examples were documented in an Excel database, including the information source, industry, LA, interaction and any important contextual commentary. Using a CIS approach facilitated the highly iterative stance, allowing for ‘question modification’40 in response to the emergent findings, which altered and refined the typology.
Results
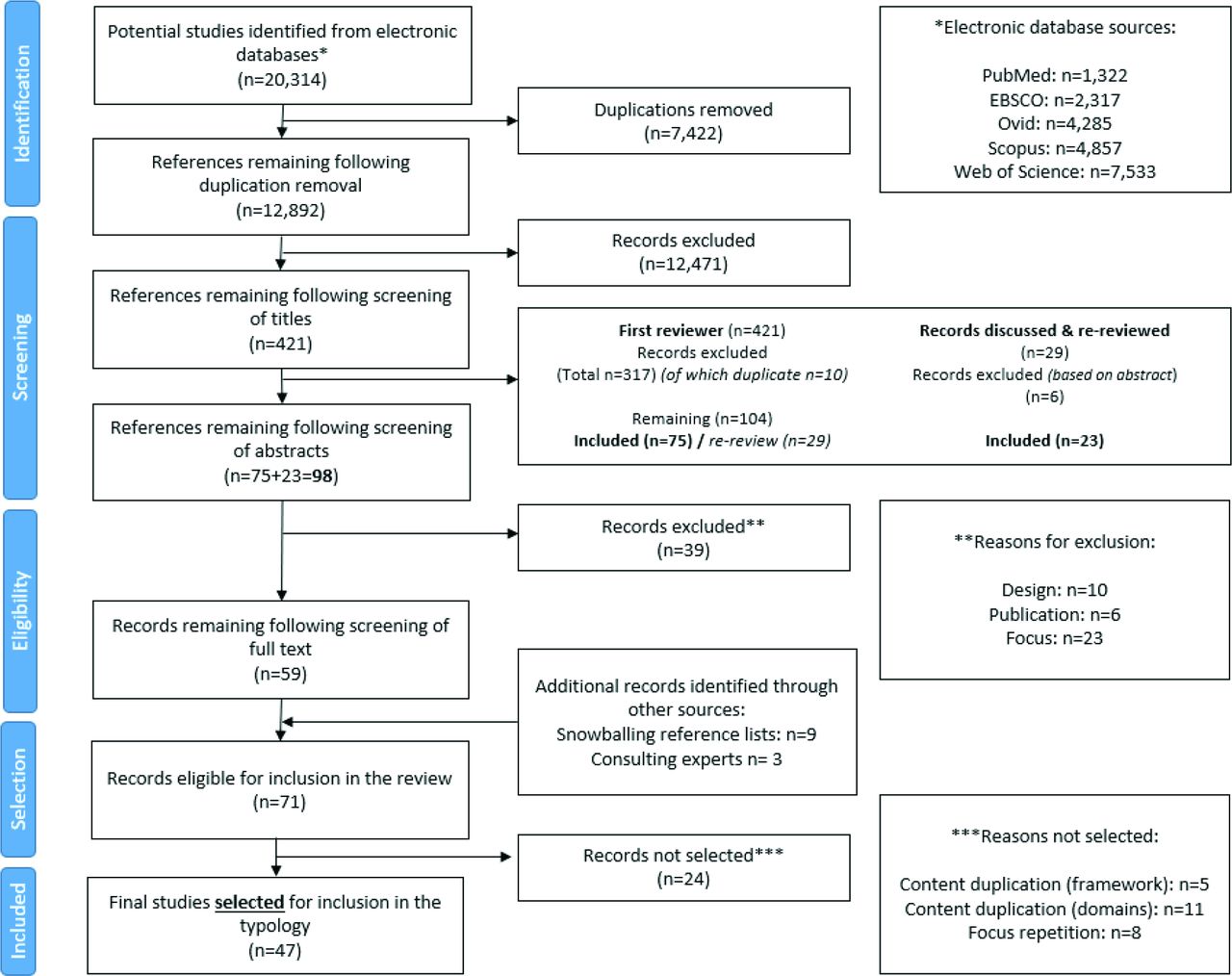
The results of the identification, eligibility and selection process are shown in figure 1. Out of the 71 potentially eligible studies, we did not select 24 due to content duplication of: the framework (n=5); the domains (n=11); or the study focus (n=8) (online supplemental table 5). The retained 47 studies included reviews (n=19; 40%), qualitative analyses (n=8; 17%), essays (n=7; 15%), short pieces (n=5; 11%), case studies (n=4; 9%), concept mapping (n=2; 4%) and theory/tool development (n=2; 4%). HCIs in these papers included tobacco (n=10; 21%), food (n=10; 21%), baby food (n=1; 2%), non-specific ‘unhealthy commodity industries’ or private sector/corporations/industries harmful to health (n=13; 28%), gambling (n=5; 11%), alcohol (n=4; 9%) and a combination of two industry types (n=4; 9%). Full details are described in online supplemental table 6, including the 24 studies not selected (online supplemental table 5). Grey literature evidence included LA websites and reports, non-governmental organisations (NGOs), government documents, news and media reports, among other sources (online supplemental table 7).

Study selection process (PRISMA flow diagram). PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
An overview of the context in the current literature
We did not identify any previous study that analysed interactions between HCIs and LAs. The conceptualisations, framing and language used to describe and understand the ways industry engages with public health was weighted towards the CDoH,2 6 18 44 52–55 corporate and commercial power,1 11 13 56–59 CPA,23 46 60–67 tactics10 68 or strategies69–71 and CSR22 72–79 literature. Studies were mostly in a broad context, such as global or population health settings, focused on international policy and examining transnational corporations. For example, exploring corporations’ commercial involvement in public health policy,80 or a framework and mechanisms of transnational corporations’ macrosocial and corporate tactics regarding population health and policy.13 Some studies focused on specific populations, industries, policies or activities, but remained in a similar lens, focusing on the CPA of industries.
A proposed typology of possible interactions between HCIs and English LAS
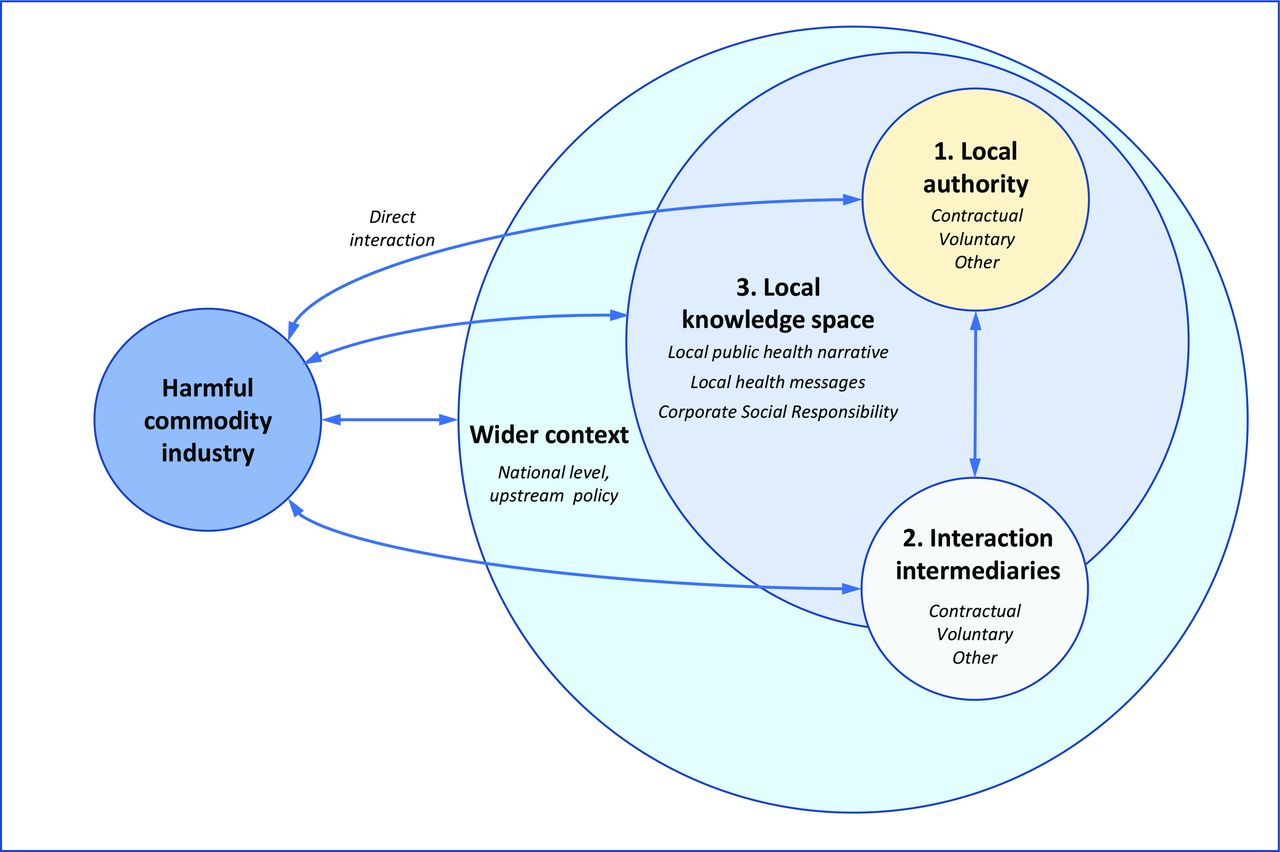
Table 2 presents our proposed typology of the interactions between HCIs and English LAs. Three categories of potential interactions were developed, based on the medium through which the interactions take place: (1) direct involvement with the LA (governmental), (2) involvement through intermediaries (third parties) and (3) involvement through the local knowledge space. The typology expands on these three categories, with 10 themes describing the nature of interactions, encompassing over 50 potential interactions and illustrative examples.
A typology of potential interactions between harmful commodity industries (HCIs) and local authorities (LAs) with illustrative examples in the English context
Due to the complex and multifaceted nature and diverse presentation of potential interactions, the categories are not necessarily mutually exclusive, and some interactions cross multiple themes or categories. Also, other interactions take place within the wider context, at global and national levels, which shape and influence the local interaction landscape. Several interactions may also occur within the LA jurisdiction, but without explicit LA involvement, and some activities may remain within the traditional CPA lens. As a result, while many interactions and examples provided are specific and clear, we acknowledge that other, wider interactions (eg, with International and National bodies, NGOs, research councils) may be less clear, but have a significant presence and implications across multiple LAs. Figure 2 offers a visual representation of the typology and wider components contributing to the interaction landscape.
{kind=link}
{kind=link}
Visual representation of the interaction landscape.
Category 1: involvement with the LA (governmental)
We identified three themes to summarise the ways in which HCIs and LAs directly interact with each other. The first theme includes contractual, legal and regulatory interactions involving formal arrangements between the two parties. These arrangements potentially involve monetary exchange, for example, licensing and registration of alcohol or drinking establishments, food outlets and gambling venues. Other interactions include business links, such as LA investments in industry, and joint endeavours in the LA jurisdiction. Legal interactions include direct litigation against a decision and the use of the legal system to threaten or contend LA policies, organisations, and individuals, stretch local legal boundaries or threaten legal outcomes. The second theme involves voluntary engagements between industry and LAs, and the most prominent examples include public–private partnerships, followed by cooperative arrangements (such as voluntary agreements and pledges). In addition, interactions include joint attendance in meetings and working groups, and voluntary input to policy makers in, for example, writing policies. The third theme includes all other engagement strategies. These interactions include incentivising career movement across public and private posts (‘revolving door’ arrangements), and relationship or network building. In addition, reactive strategies and responses to LA policies and decisions, and creating or emphasising disincentives, when arrangements are disagreeable.
Category 2: involvement through intermediaries (third parties)
The second category of interactions between HCIs and LAs specifically involves intermediaries to which we identified the same three themes. The first theme, contractual interactions, again mostly involve monetary exchange or shared financial interests, such as funding an LA project or services, cobranding in the LA jurisdiction or cause-related marketing. The second theme, voluntary interactions, include industry strategic support of local NGOs such as small-medium enterprises and charities, through partnering, funding and joint projects. These interactions often involve supporting local community ‘worthy causes’, claim to act in the interests of communities and offer solutions for LA priorities and community needs. For example, during the COVID-19 pandemic, larger industries provided funding smaller local businesses struggling with reduced demand.81 The third theme, other engagement strategies, closely aligns HCIs with key stakeholders in the local area, creating HCI support and networks, and broadening the interaction landscape. For example, relationships with local key opinion leaders, business links such as financial ties across industry (eg, investments and shares), or other interlocking features, such as shared directorates, public relations (PR), legal or marketing firms across industry. In addition, the media forms a vital platform as an interface between industry, LA and the wider public, providing a mode of indirect communication, through local media, PR associations, journalists and bloggers, providing access to local councillors, stakeholders or specific communities.
Category 3: involvement through the local knowledge space
Interactions most commonly identified from our searches are those involving the local knowledge space (the local area in which the LA has jurisdiction), through influencing local health messages, challenging the local public health narrative and CSR strategies. It is important to acknowledge that the wider, national-level knowledge space also influences the local knowledge space. First, HCIs interact with public health messages which influence the local knowledge space, for example, funding research activities and securing relationships with key researchers, to undermine, reframe and promote messages reflecting their goals and positionality. Other interactions include undermining key spokespersons, reframing LA intentions and creating or emphasising antagonisms. HCI CSR strategies could serve as an interaction interface through LA promotion of CSR, and CSR aligned with LA goals. Interactions could include the local economy (business rates, taxes, rents), employment opportunities in the locality (eg, suppliers, distribution, construction) or the local community (support, sponsorship, building/developing) among a plethora of other interactions involving local areas, the local working and living environment, extending from local schools to environmental initiatives (eg, sustainability, pollution abatement). These CSR interactions form part of a strategy for HCIs to present themselves as acting within public interests, to shift the blame, whitewash tarnished reputations and enhance the normalisation of products known to be harmful to health.
Discussion
Summary of main findings
To our knowledge, this is the first study to develop a typology of the potential interactions between HCIs and local government, with case examples drawn from England. Drawing on previous published frameworks and conceptualisations, and grey literature, our typology classifies potential interactions according to the medium through which they take place. Interactions occur both directly with the LA and indirectly through intermediaries by contractual, voluntary and influential means, and via the local knowledge space, involving local health messages, the local public health narrative and CSR. Our perspective and findings acknowledge the wider CDoH environment, and upstream contextual factors, which shape the interaction landscape at a local level.
Given the extent of potential interactions, we suggest that the interactions between HCIs and local government may have a significant role in shaping local environments in which people work and live, and thus health behaviours and associated outcomes at a population level. Our conceptualisation of interactions acknowledges the LA perspective, in which working with the private sector generally is often seen as acceptable by LAs to execute functions to enhance local society, in and out of the public health domain (eg, planning, community development, transport). The proposed typology is not definitive, and could be enhanced with further evidence, synthesis and future research.
Strengths and limitations
A major strength of this study is that it proposes a novel and detailed typology with methodological rigour, that identifies ways HCIs and LAs interact, which may be used by LAs to assess their own practices. To the best of our knowledge, this is the first framework to consider HCI interactions at an LA level. Drawn on well-established CDoH theories and frameworks, our typology offers new utility and applicability for research and practice. The provided typology should enable further study of these interactions and develop pragmatic ways in which LAs and HCIs can interact, to maximise population health interests.
This study has some limitations. First, we only used five databases for our literature search, which although in combination offered a diverse range of literature, may not fully depict the business relations documented in the wider literature. Although this paper did not aim to review all the relevant work, some important, related work, may not have been included. The lens, of studying ‘interactions’ with HCIs, has not been previously adopted and previous literature, including the underpinning theory, methods and illustrative cases, is mostly skewed towards a CPA lens. In addition, despite the aim to adopt a lens that reflects the LA viewpoint besides the public health perspective, we acknowledge the potential for bias in our interpretation.
Although we aimed to capture local level interactions, we acknowledge that there are other influences, including at national and international level, which manifest locally but are not captured in detail in this manuscript, due to the specific focus on LA levers. We acknowledge that by applying our typology to the English LA context, our examples may be most aligned with similar political systems in HIC settings. However, transnational harmful commodity organisations operate on global markets and their approaches share commonalities across both HIC and LMIC settings, but this has not been explored at an LA level and warrants further research. The reliance on publicly available information to gain the LA context also has limitations. Some of the interactions lack documented evidence and are dominated by opinion-based and anecdotal evidence, and hidden, invisible, informal and some indirect interactions were not captured.
Situating the typology within the wider literature
While previous efforts to describe and monitor the practices of HCIs have focused on CPA efforts and in a wider context, we focus on interaction, specifically in the English LA context. We have not attempted to describe or define the CDoH or CPA, or the broad dynamics that constitute elements previously comprehensively synthesised.52 82 However, the current typology is derived from this literature, most prominently utilising aspects of CPA formerly identified.46 63 Mialon et al46 developed a step-by-step approach to monitor the CPA of the food industry within countries. In addition, the ‘Corporate Permeation Index’83 quantifies the penetration of corporations in a given country. Similar methods could be developed to examine and monitor interactions between HCIs and LAs, using the current typology.
The lens and typology we present recognises that interactions between HCIs and LAs are fundamental for LA functioning. Overwhelming evidence1 2 6–15 84 opposes HCI involvement, and stresses the significant harm to the health of the public from public health and corporate HCI partnerships, with limited benefits.85 Contrasting arguments suggest that the benefits of commercial influence (eg, economic growth) outweighs adverse health outcomes,86 and private sector interactions more generally are viewed as potentially mutually beneficial to the wider, non-public health stakeholder.18 86 87 While acknowledging that population health improvement may necessitate interaction with the private sector,18 the wider long-term harmful effects of HCI interactions may not be adequately considered and accounted for, necessitating the application of criteria, conditions and safeguards to govern the commercial influences on population health. Further, the significance of the problem is likely to continue as local government financing constrictions prevail (UK and internationally) due to COVID-19 pressure, requiring more local funding activities, including through interactions with HCIs. Thus, our analysis suggests there is the need and opportunity to develop LA guidance to support local decision making that considers the population health impacts and minimises the health and reputational risks of HCI interactions.
In recognising the wider context in which our typology is situated, we echo the importance of wider interconnected elements and need for interventions across whole systems at the LA level.88 LAs hold unique and substantial powers to shape local environments through various mechanisms. Despite LAs having powers to govern HCI interactions and protect public health, we found that the extent to which LAs use their levers varied. For example, while some LAs have enacted commercial policies to restrict interactions such as those mirroring the TFL junk food advertisement ban, other interaction examples specifically demonstrate LAs seeking out commercial opportunities with HCIs, enabling advertisement and sponsorship of their products in the local area. Recent work89 reviewed LAs ability to contribute to the change process for healthy food systems and environments and stressed the need to empower LAs. A lack of LA empowerment or involvement could, in part, explain several of the identified potentially harmful interactions, such as, licensing and planning. A recent census study90 across English LAs explored takeaway food outlet planning and regulation. The authors observed just 56 of 325 LAs had health-specific planning criteria, compared with 80% non-health (eg, litter, anti-social behaviour), owing to the acceptability and probability of challenge.90 It is important that considerations for health should be embedded across all LA functions and decisions, as existing beliefs may dichotomise LA roles and functions into those which are health focused, and those which are not.91
LAs have proven capacity to take effective action, advance population health goals and overcome the CDoH,89 including managing the built environment,90 yet, more often, intervention design prioritises avoiding potential confrontation or dispute (eg, improving the healthfulness of takeaway outlets).92 Recent work by Mialon et al93 identified how Freedom of Information (FoI) disclosure logs, and disclosures of conflicts of interests have been adopted in the UK as mechanisms to monitor and address the influence of corporations on population health. Yet, their findings are at national, regional and global levels, without LA level evidence.93 LAs, through legislative and regulatory powers, can make significant and meaningful changes to business activities, structures, rules, norms and practices.94 Developing guidance and standards for interactions with HCIs could increase transparency and empower LAs to assess potential health impacts to the local population as well as possibilities of associated reputational risks.
Research implications
The proposed typology of interactions presented can now be used to systematically explore further opportunities to add new interactions, and tailor the manifestation of interactions in both similar and distal contexts. The typology is not definitive but is a conceptual starting point to be modified and built on. Future work to supplement missing information could increase the validity, for example, through wider sharing of the typology and surveys to build consensus. Interviews with key stakeholders, such as LA actors, third party organisations and public representatives could describe their positionality, interactions used and outcomes. Involving stakeholders most affected is warranted to incentivise and empower policy makers to act, which otherwise presents a challenge to the acceptability and practical usability of the research. In addition, this would assist in identifying interactions that may not currently be evidenced in the public domain.
The typology was informed by international literature and translated to a local-level context. While we acknowledge the findings may be most aligned with similar political systems in high-income country settings, we suggest that the ‘interaction’ lens, within a local context, has the potential to be applied more generally. Further research is needed which accounts for the wider socioeconomic, and the importance of political economy and governance context, on HCI–LA interactions, to enhance the practical applicability of adopting this Framework.
We do not attempt to quantify the extent to which the interactions are attributed to outcomes, such as local NCD prevalence, health inequalities, commercial and wider public implications. Outcomes of the interactions should be assessed, to understand who benefits and the net consequences, for the industries, LAs and local communities involved. In addition, interactions between LAs and other industries (eg, coal, oil and gas) are also of public health concern and future work could extend the concepts described in this paper, across other HCIs.
Policy and practice implications
To make meaningful improvements in health, future work could build on these findings to develop interventions and practical tools for specific actions that LAs can take. Standards could be adapted and applied to govern local interactions, such as previous work extending and tailoring the use of the ‘MPOWERR’ tool89 covering marketing, advertising, sponsorship and planning provisions. Guidance that incorporates an LA perspective, could ensure that LAs interact with HCIs in a way that optimises business opportunities while protecting population health and avoiding reputational risks.
Conclusion
This study describes the development of a typology, drawn from a synthesis of the well-established academic literature in combination with local-level evidence. Our typology provides an overview of the potential interactions between HCIs and LAs. The typology can facilitate new understanding that explores the LA perspective of interactions with HCIs, to support LA policy and decision-makers, in and outside of public health. Furthermore, the typology should serve as a platform for future research to build on, as a practical approach to curtail the CDoH-NCD pandemic, and further supplement national level NCD policy actions (eg, obesity strategy), by focusing on HCI and LA interactions.
Data availability statement
Data are available on reasonable request. No data are available.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to acknowledge the contributions of Eugene Milne, Karen Lock, Felix Greaves, and Vanessa Er to the development of the research concept and discussions. We thank our public collaborators who assisted as research volunteers throughout the research process, including the methodological planning, and consultation of the research appropriateness and relevance. These were Mike Etkind, Maisie McKenzie, Sandra Jayacodi, Prisha Shah and Deborah Smith.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Eduardo Gómez
Twitter @Eszti_Vamos
Contributors All authors (SM, EPV, MW, MP, CS, MV, EB, SC, AAL, CJ, CM, FDV and EH) contributed to the development of the research concept and methods. SM led data collection, analysis and writing of the manuscript. EPV supported in the review process. All authors contributed to data interpretation. All authors contributed to the editing of the manuscript before publication. SM is responsible for the overall content as guarantor. SM accepts full responsibility for the finished work, the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This study was funded by the National Institute for Health Research (NIHR) School for Public Health Research (SPHR), Grant Reference Number PD-SPH-2015. CJ's salary is partly funded by Public Health at Westminster City Council and the Royal Borough of Kensington and Chelsea and supported in part by the Northwest London NIHR Applied Research Collaborative. Imperial College London is grateful for support from the Northwest London NIHR Applied Research Collaborative and the Imperial NIHR Biomedical Research Centre. MW is supported by the MRC Epidemiology Unit, University of Cambridge (grant number MC/UU/00006/7).
Disclaimer The views expressed in this article are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.