Article Text

Abstract
Background Rapid diagnostic tests (RDTs) are widely used for diagnosing Plasmodium vivax malaria, especially in resource-limited countries. However, the impact of RDTs on P. vivax malaria incidence and national medical costs has not been evaluated. We assessed the impact of RDT implementation on P. vivax malaria incidence and overall medical expenditures in South Korea and performed a cost–benefit analysis from the payer’s perspective.
Methods We developed a dynamic compartmental model for P. vivax malaria transmission in South Korea using delay differential equations. Long latency and seasonality were incorporated into the model, which was calibrated to civilian malaria incidences during 2014–2018. We then estimated averted malaria cases and total medical costs from two diagnostic scenarios: microscopy only and both microscopy and RDTs. Medical costs were extracted based on data from a hospital in an at-risk area for P. vivax malaria and were validated using Health Insurance Review and Assessment Service data. We conducted a cost–benefit analysis of RDTs using the incremental benefit:cost ratio (IBCR) considering only medical costs and performed a probabilistic sensitivity analysis to reflect the uncertainties of model parameters, costs and benefits.
Results The results showed that 55.3% of new P. vivax malaria cases were averted, and $696 214 in medical costs was saved over 10 years after RDT introduction. The estimated IBCR was 2.5, indicating that RDT implementation was beneficial, compared with microscopy alone. The IBCR was sensitive to the diagnosis time reduction, infectious period and short latency period, and provided beneficial results in a benefit over $10.6 or RDT cost under $39.7.
Conclusions The model simulation suggested that RDTs could significantly reduce P. vivax malaria incidence and medical costs. Moreover, cost–benefit analysis demonstrated that the introduction of RDTs was beneficial over microscopy alone. These results support the need for widespread adoption of RDTs.
- mathematical modelling
- epidemiology
- malaria
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
There are relatively few studies on the modelling of Plasmodium vivax malaria, and the seasonality and long incubation period of P. vivax malaria are not well reflected in available models.
Although rapid diagnostic tests (RDTs) are widely used for diagnosing P. vivax malaria, the impact of RDTs on P. vivax malaria incidence and national medical costs has not been evaluated.
What are the new findings?
Using national surveillance data and climate data, we developed a dynamic model for P. vivax malaria in South Korea, explaining seasonality and long incubation period intuitively.
The introduction of RDT remarkably reduced medical costs as well as malaria cases. Besides, the cost–benefit analysis showed beneficial results.
What do the new findings imply?
The model we developed can be applied for assessing P. vivax malaria transmission in other countries and also can be extended to P. falciparum malaria.
The regimens to analyse the impact of RDT implementation on disease burden and cost provide useful tools to prepare guidelines to achieve the goal of malaria eradication in many areas, including South Korea.
Introduction
Despite the government’s vigorous efforts, Plasmodium vivax malaria has not been eradicated in South Korea since its re-emergence in 1993 from a soldier in military service near the demilitarised zone, as shown in online supplemental figure 1.1 The WHO has recommended that South Korea eradicate malaria by 2023,2 and the Korea Centers for Disease Control and Prevention (KCDC) has launched the ‘Five-Year Action Plan for Malaria Eradication’ (2019–2023), including the introduction and insurance coverage for malaria rapid diagnostic tests (RDTs).
Supplemental material
RDTs were developed in the early 1990s for the simple, rapid and accurate diagnosis of malaria.3 4 The high accuracy of the RDT has been proven in previous studies. According to a Cochrane review, the sensitivity and specificity of RDT are 99% in endemic countries.5 A study conducted in South Korea also showed more than 99% concordance.6 In addition, according to the WHO Malaria Rapid Diagnostic Test Performance report, the false-positive rate is 0 in several tests commercialised for P. vivax.7 RDTs are widely used in countries with poor medical resources, especially where the use of light microscopy is limited; therefore, WHO has recommended the implementation of RDTs for diagnosing malaria, published relevant guidelines and released results of RDT kits annually to ensure quality.7 8
There have been numerous studies on mathematical modelling of malaria. However, most studies have focused on P. falciparum malaria, with few studies focusing on P. vivax malaria. Recently, several studies have been conducted on P. vivax malaria in South Korea.9–11 However, these studies did not provide a reliable evidence for model calibration. Hence, it is crucial to develop an accurate model for P. vivax malaria for the assessment of the RDT introduction in South Korea.
Although previous studies have reported microscopy-based and RDT-based detection of P. vivax malaria, studies to verify the effects of RDTs have been conducted mostly in resource-limited settings.12–14 Most of the studies which have performed cost-effectiveness analyses used decision tree models and concluded that RDT use was more cost-effective than microscopy or clinical-based diagnosis.15–17 Some studies concluded that microscopy is cost-effective or that RDT is effective but costly; however, they also used a decision tree model that could underestimate RDT efficiency.18 19 The introduction of RDTs would incur additional costs for diagnosis but could save unnecessary medical expenses by reducing the diagnostic time in the settings where a microscopy-based diagnosis is readily accessible. This introduction could also contribute to reducing malaria incidence due to reduced chances for secondary malaria infection. Therefore, research on the effects of RDT introduction is important not only from medical but also from health policy perspectives as it is related to medical expenses.
Therefore, we developed a dynamic compartmental mathematical model for P. vivax malaria to assess the impact of RDT initiation on malaria incidence and overall medical expenditures in South Korea, and performed a cost–benefit analysis from the payer’s perspective. This is the first study to assess the influence of RDTs in a country with a highly qualified medical environment and will provide evidence for the inclusion of RDTs in national health insurance coverage.
Methods
Study design and data sources
This study considered two diagnostic scenarios. The base scenario was to diagnose only with microscopy, and the control scenario was to diagnose using both microscopy and RDT at the same time. Since microscopy-based diagnosis has remained the gold standard after the introduction of RDTs in South Korea in 2012, no patient was diagnosed with P. vivax malaria using only an RDT. We predicted future malaria incidences and total medical costs over the next 10 years for both scenarios. We then estimated the incremental benefit:cost ratios (IBCRs) of the introduction of RDTs.
For model calibration, malaria incidence data in malaria-risk areas, including Incheon, Gyeonggi and Gangwon provinces, for the last 5 years (2014–2018) were obtained from the annual report of KCDC. To reflect realistic demographic and climatic conditions in these regions, data from the Korean Statistical Information Service and the Korea Meteorological Administration were obtained and used for model parameter setting.20–22
To estimate the overall medical cost and to perform a cost–benefit analysis of RDT use, data from the National Health Insurance Ilsan Hospital (NHIIH) and the Health Insurance Review and Assessment Service (HIRA) were used. The NHIIH is a general hospital with 822 beds located in an area at risk for P. vivax malaria. We reviewed the medical records of patients diagnosed with P. vivax malaria at NHIIH between January 2009 and December 2018. We also extracted data from the HIRA, which is a nationwide, mandatory insurance database for all enrolled Korean citizens. All citizens are obliged to be enrolled in the National Health Insurance System. Under this system, all costs for medical care on National Health Insurance or Medical Aid are claimed to the HIRA for reimbursement from the National Health Insurance. The data from the HIRA have been shown to be reliable, and many studies have been conducted in this manner in South Korea.23 24
Modelling and interventions
Since malaria is a vector-borne disease, the model was stratified into two species, human and mosquito, as shown in figure 1. We divided the model into susceptible ( ), exposed (
), exposed ( ), infectious (
), infectious ( ) and treated (
) and treated ( ) states for the human population and into aquatic (A), susceptible (
) states for the human population and into aquatic (A), susceptible ( ), exposed (
), exposed ( ) and infectious (
) and infectious ( ) states for the mosquito population.
) states for the mosquito population.

Diagram of the Plasmodium vivax malaria model. The subscripts h and v denote the human and vector, respectively. The flows are  for patients who had a short latency period,
for patients who had a short latency period,  for patients who had a long latency period and
for patients who had a long latency period and  for patients who had relapse. The dashed lines indicate the transmission between humans and mosquitoes.
for patients who had relapse. The dashed lines indicate the transmission between humans and mosquitoes.
Newborn babies enter the susceptible human ( ) state at a rate of
) state at a rate of  and leave the model if they die at a rate of
and leave the model if they die at a rate of  . Once humans are infected by infectious mosquitoes (
. Once humans are infected by infectious mosquitoes ( ) at a rate of
) at a rate of  , they move into the exposed state (
, they move into the exposed state ( ) and can have either short (
) and can have either short ( ) or long (
) or long ( ) latency periods. This is an essential characteristic of P. vivax malaria and is implemented by delay differential equations; the detailed equations are in the online supplemental material 1. If the disease develops sufficiently for the transmission of the parasite to susceptible mosquitoes (
) latency periods. This is an essential characteristic of P. vivax malaria and is implemented by delay differential equations; the detailed equations are in the online supplemental material 1. If the disease develops sufficiently for the transmission of the parasite to susceptible mosquitoes ( ), they progress to the infectious stage (
), they progress to the infectious stage ( ). We assumed that all patients are diagnosed and treated at a rate of
). We assumed that all patients are diagnosed and treated at a rate of  and move to
and move to  as soon as they start treatment. Since the accuracy of the RDT for P. vivax has been proven to be very high, we have not considered a false-negative rate. Treated humans (
as soon as they start treatment. Since the accuracy of the RDT for P. vivax has been proven to be very high, we have not considered a false-negative rate. Treated humans ( ) leave the compartment at a rate of
) leave the compartment at a rate of  , and there is a possibility q of relapse. Otherwise, the patients return to the susceptible group (
, and there is a possibility q of relapse. Otherwise, the patients return to the susceptible group ( ).
).
Supplemental material
Adult mosquitoes ( ) lay eggs at a rate of
) lay eggs at a rate of  ; however, the size of the immature mosquito population is limited to ka because of the capacity of the sites with proper environments for breeding and egg development. Immature mosquitoes (A) can either die at a rate of
; however, the size of the immature mosquito population is limited to ka because of the capacity of the sites with proper environments for breeding and egg development. Immature mosquitoes (A) can either die at a rate of  or grow into susceptible adult mosquitoes (
or grow into susceptible adult mosquitoes ( ) at a rate of
) at a rate of  . By biting infectious humans (
. By biting infectious humans ( ), susceptible mosquitoes can be infected at a rate of
), susceptible mosquitoes can be infected at a rate of  and move into the exposed stage (
and move into the exposed stage ( ) and progress into the infectious stage at a rate of
) and progress into the infectious stage at a rate of  . Adult mosquitoes at all stages can fail to survive and die at a rate of
. Adult mosquitoes at all stages can fail to survive and die at a rate of  .
.
The model parameters were categorised into three types, namely, those for humans, mosquitoes and transmission parameters induced by the contact between humans and mosquitoes. The demographic parameter values for humans were obtained from the statistical data,20 21 and parameters for the latency periods, infectious period and relapse were based on malaria reports from the KCDC1 and previous studies.11 25–29 The treatment start rate, which was estimated as the reciprocal of the average infectious period, was set to 1/4 (1/days) based on reports of malaria-risk areas.1
As the mosquito life cycle depends on the climate, we assumed most of the mosquito-related model parameters depended on temperature and referred to previous laboratory-based studies.25 26 Detailed descriptions of the model parameters and values are included in online supplemental table 1.
Supplemental material
We calibrated the model using civilian malaria incidence data in malaria-risk areas (Incheon, Gyeonggi and Gangwon provinces) in South Korea from 2014 to 2018 obtained from the KCDC. The least-squares method was used to estimate three uncertain parameters: transmission probability from  to
to  (
( ), transmission probability from
), transmission probability from  to
to  (
( ) and probability of having a short latency period (p). The data and model prediction from the estimated parameters are displayed in online supplemental figure 2.
) and probability of having a short latency period (p). The data and model prediction from the estimated parameters are displayed in online supplemental figure 2.
Supplemental material
In South Korea, microscopy-based methods have been continuously used as the gold standard method for malaria diagnosis. In 2012, RDTs were introduced in the NHIIH, which, combined with microscopy, resulted in a reduction in the median of 12 hours required for diagnosis based on the result reporting time. Therefore, in the model, we configured two diagnostic scenarios by setting  for the microscopy scenario (microscopy only) and
for the microscopy scenario (microscopy only) and  for the microscopy+RDT scenario. The sensitivity analysis assumed an infectious period of up to 5 days for the microscopy scenario and a reduction in diagnostic time of up to 1 day for the microscopy+RDT scenario.
for the microscopy+RDT scenario. The sensitivity analysis assumed an infectious period of up to 5 days for the microscopy scenario and a reduction in diagnostic time of up to 1 day for the microscopy+RDT scenario.
Medical costs
We used the microcosting approach to estimate the average medical costs per patient for one episode of malaria from each data source. We included the cost for administering medications, the cost for injection, a fee for procedure or surgery, laboratory tests, imaging studies including CT and ultrasound, medical devices/supplies and blood transfusion. The prices of RDT and microscopy were extracted based on NHIIH data as well. All costs and prices are presented in US dollars based on the 2019 yearly average exchange rate of $1165.65. The estimated average medical costs per patient were $799.02 for microscopy only and $796.56 for both microscopy and RDT.
In HIRA data, patients diagnosed with P. vivax malaria were defined according to the appropriate diagnosis code using the Korean Classification of Disease, which is based on the International Classification of Diseases, 10th Revision, Clinical Modification. The diagnosis codes for P. vivax malaria were B51 and B54. However, it was not possible to clearly distinguish whether P. vivax malaria patients were diagnosed by microscopy alone or by microscopy and RDTs, as RDT use was not subject to reimbursement. Therefore, for 2012, the year of RDT introduction, we defined patients diagnosed by microscopy alone as patients diagnosed with P. vivax malaria in 2011 and patients diagnosed by microscopy and RDT as patients diagnosed with P. vivax malaria in 2013. The estimated costs for HIRA data are shown in online supplemental table 2.
Supplemental material
Cost–benefit analysis
We assumed that the introduction of RDT would incur more costs only for the diagnosis. Based on the assumption that delays in diagnosis can lead to additional medical resource usage and expenditures, we estimated the benefit from the difference between two medical costs excluding each diagnostic cost. From NHIIH data, the costs of microscopy and RDT were estimated at $11.72 and $23.91 each, and the benefit per patient diagnosed with RDT was estimated at $26.38. While RDTs may provide benefits beyond reducing medical expenditures, such as saving time and reducing anxiety and productivity loss, this study focused on medical costs due to its tangible monetary value. We applied the same method to HIRA data to estimate the benefit, which was lower than that from the NHIIH data, as shown in online supplemental table 2. The only difference between the two data was the benefit amount. Therefore, we assessed the results of HIRA data using a sensitivity analysis as described in the online supplemental material 1.
The IBCR is commonly used to compare benefits and costs among multiple interventions. As we estimated the benefits from the difference in medical costs between scenarios, the IBCR was an appropriate measurement for cost–benefit analyses. The formula is shown as follows:
IBCR=incremental benefits/incremental costs
Both benefits and costs are discounted at 3% annually. We also investigated the sensitivity of the model parameters, costs and benefits to the IBCR in 2028. Univariate and bivariate sensitivities were explained by a tornado diagram and heat map, respectively.
Patient and public involvement
There was no patient or public involvement in the study.
Results
Malaria incidence
To estimate the impact of RDTs alone, we assumed no climate changes in the future prediction and a consistent malaria incidence for over 10 years in the microscopy scenario, as shown in figure 2. After the introduction of RDTs in 2019, malaria cases decreased remarkably over 10 years. In the first year, the incidences following a long latency period were identical in both scenarios as these patients were infected in the previous year. However, due to the reduced chances of secondary infection from delayed diagnosis, the incidences after a short latency period started to decline, averting 12 cases in 2019. This impact propagated to the next year through people having a long latency period; consequently, it prevented 42 new incidences in the second year. After 10 years of successive RDT intervention, 84.9% of cases will be averted in 2028, and cumulatively, 1025 (55.3%) of cases will be prevented.
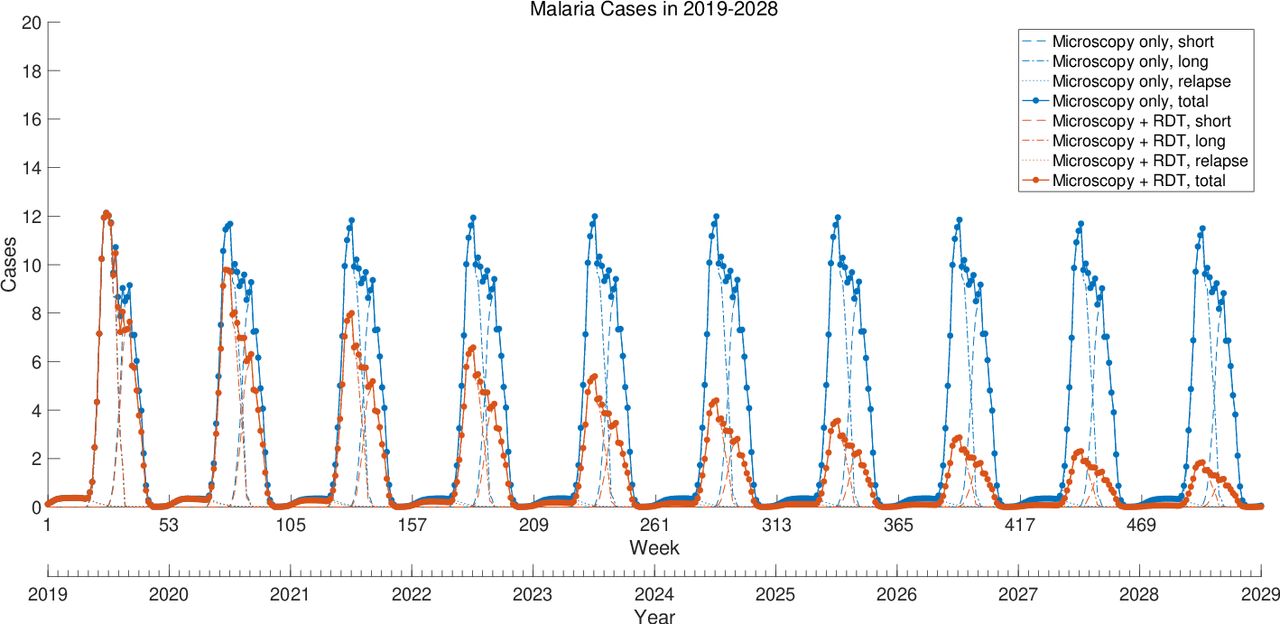
Prediction of weekly Plasmodium vivax malaria cases (2019–2028) and impact of RDT implementation. Total cases are the sum of short, long and relapse cases. RDT, rapid diagnostic test.
Medical costs
The total medical costs were computed by multiplying the cases by the average medical costs per patient. The lower costs and reduced number of cases in the RDT scenario resulted in large expenditure savings every year. The cost gap between the two scenarios increased, with $93 200 in medical cost–savings in 2028 and $696 214 accumulated over 10 years.
Cost–benefit analysis
Compared with the microscopy scenario, RDT was beneficial from the first year of its introduction, with the IBCR exceeding 1, as shown in figure 3. With increasing years, the IBCR increased and the incremental benefits were 2.5 times the incremental costs at the end of time horizon. Incremental benefits increased each year. Meanwhile, the incremental costs increased up to the sixth year and started to decrease thereafter because the reduced number of P. vivax malaria cases in the RDT scenario resulted in slow increases in cumulative costs. Consequently, IBCRs can accelerate to 2.5 in 10 years.
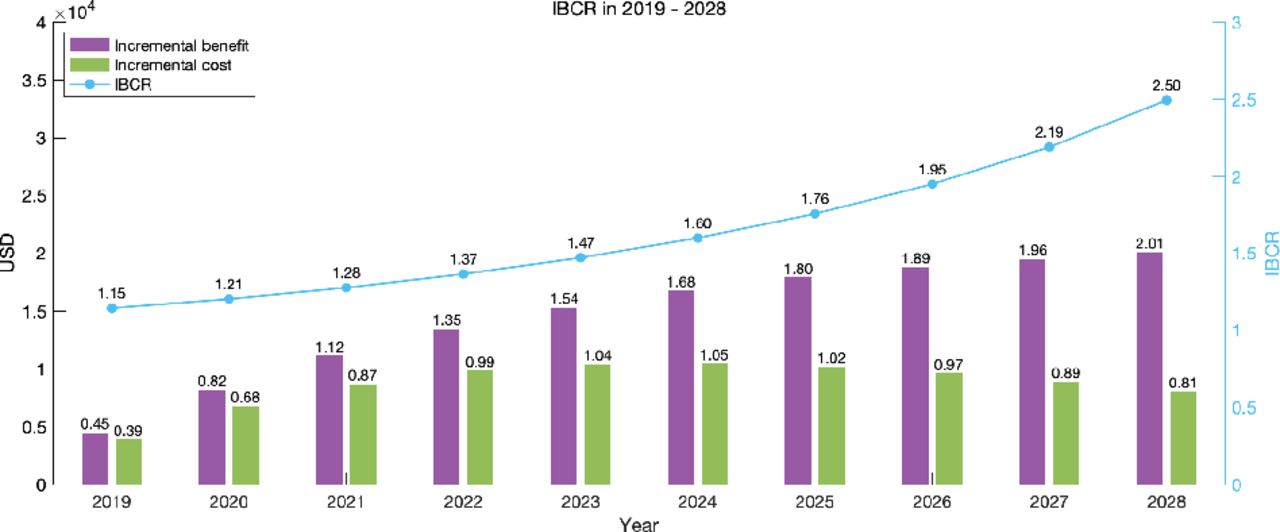
Yearly cumulative incremental benefits and costs, as well as IBCRs, 2019 −2028. IBCR, incremental benefit:cost ratio; USD, US dollar
Probabilistic sensitivity analysis
Univariate sensitivity
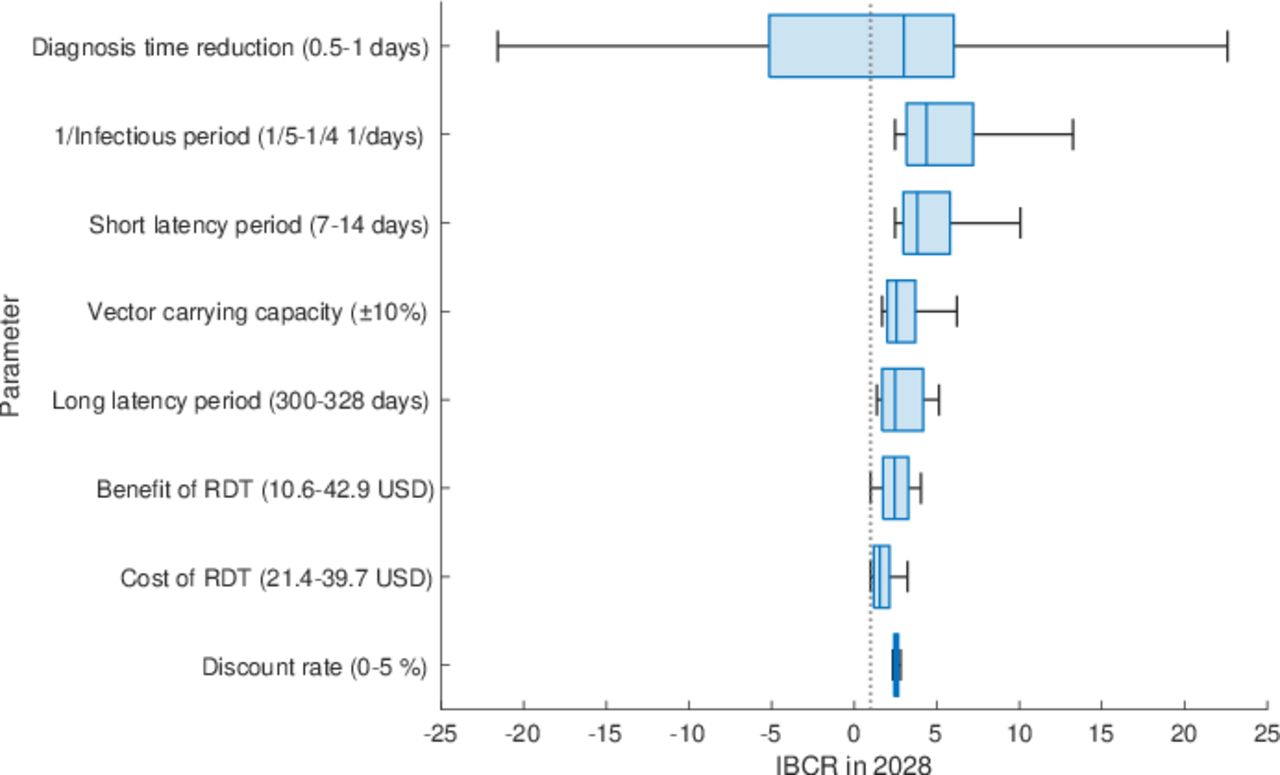
To determine which parameters were most sensitive to the IBCR, we perturbed all parameters by the same percentages of their values and selected the eight most sensitive parameters. Then, with a realistic parameter range, we assumed uniform distribution and re-examined the sensitivity by sampling 1000 values for each parameter. As shown in figure 4, a diagnosis time reduction, infectious period and short latency period were the three most sensitive parameters, followed by the other five parameters. A large reduction in diagnosis time due to RDT use is beneficial and saves costs, with a negative IBCR. If the infectious period is longer than that at present, more outbreaks occur in the baseline scenario, and RDTs become a more beneficial choice. Similarly, a shorter short latency period leads to larger outbreaks in the base scenario, making RDT introduction more beneficial. Especially for the benefit in the RDT scenario and price of RDTs, we estimated the minimum and maximum values reaching the threshold of 1. A benefit under $10.6 or RDT cost over $39.7 cannot achieve beneficial results. Changes in the discount rate did not significantly affect the results.

Box plot of IBCRs in 2028. For each parameter, 1000 samples were drawn from a uniform distribution with a feasible parameter range. Dotted line indicates IBCR=1. IBCR, incremental benefit:cost ratio; RDT, rapid diagnostic test.
Multivariate sensitivity
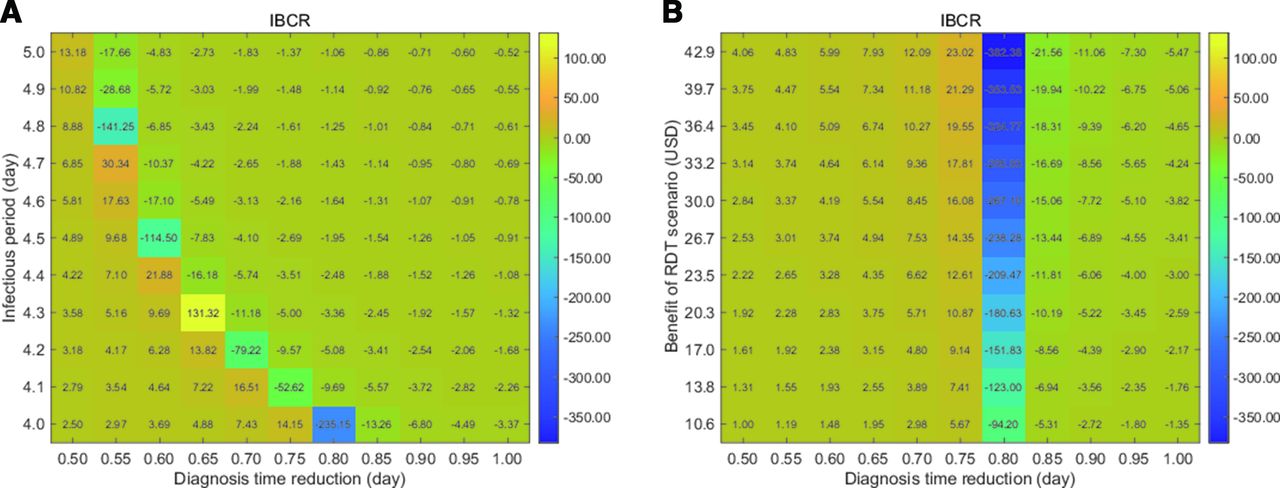
Among the eight most sensitive parameters in the univariate sensitivity analysis, we selected two combinations for bivariate sensitivity analysis. We first chose the infectious period versus diagnosis time reduction, as both parameters were acting on the same model parameter  in different scenarios. As in the univariate sensitivity analysis, diagnosis time reduction had a greater influence on IBCRs than the infectious period, as shown in figure 5A. All tested ranges provided beneficial results and cost–savings for regions with negative IBCR values.
in different scenarios. As in the univariate sensitivity analysis, diagnosis time reduction had a greater influence on IBCRs than the infectious period, as shown in figure 5A. All tested ranges provided beneficial results and cost–savings for regions with negative IBCR values.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Heatmap of IBCRs in 2028. (A) Diagnosis time reduction versus infectious period and (B) diagnosis time reduction versus benefit of RDT. IBCR, incremental benefit:cost ratio; RDT, rapid diagnostic test.
Another combination was the benefit in the RDT scenario versus diagnosis time reduction. The more the time saved in diagnosis, the greater the benefit of RDT. There could be a positive correlation between the two parameters. The results in figure 5B show that the introduction of RDTs is a beneficial choice over continuing the use of microscopy alone and also reflects situations in which diagnostic time and medical costs may vary by region and hospital.
The combined effects of the uncertainty across all the eight parameters were further investigated and are shown in online supplemental figure 4. We generated 1000 sets of the eight parameter values drawn from each distribution and obtained 1000 sets of incremental costs and incremental benefits. The slope of one dot from the origin represents one IBCR. Of all IBCRs, 95.5% were greater than 1 or negative, which means that the RDT introduction is beneficial.
Supplemental material
Discussion
We developed a model for P. vivax malaria and investigated how the implementation of RDTs will affect P. vivax malaria incidence and medical expenses over the next decade. The results verified that RDT introduction was not only effective in suppressing new P. vivax malaria cases but also had excellent benefits and a significant contribution to reducing overall medical expenses.
The key characteristics of P. vivax malaria transmission are a long latency period and seasonality. These two factors are closely related, and their combined implementation in a model is complex. Some studies have addressed this aspect using process models or survival functions.30 31 We adopted a model incorporating seasonality using temperature-dependent parameters for mosquitoes11 and added delay terms for latency periods based on insights from another study9 to fit the incidence of malaria in South Korea. This new model better described the long latency period and seasonality of P. vivax malaria than those used in previous studies; its validity was demonstrated by accurately fitting weekly malaria incidence rates in South Korea.
The median time to report results using RDTs was 1 hour (IQR 0–2 hours), whereas that for microscopy was 13 hours (IQR 2–17 hours), with 13.3% of patients diagnosed with microscopy obtaining results after more than 24 hours. As reducing the infectious period is crucial to prevent malaria transmission, reducing the diagnostic time by using RDTs is of great significance. The NHIIH is a general hospital with extensive experience in malaria treatment; considering that it is relatively early to suspect malaria and conduct tests for diagnosis, the effect of reducing the infectious period can be further maximised in areas where the incidence of P. vivax malaria is low. As the time interval from the symptom onset to P. vivax malaria diagnosis is a median of 9 days in non-risk areas of South Korea, the introduction of RDT helps improve patient prognosis.1 It also prevents the occurrence of unnecessary medical expenses and contributes to the prevention of new P. vivax malaria cases by reducing the infectious period. Furthermore, as shown from the sensitivity analysis, this also contributes to maximising the IBCR.
This study included two data sources (NHIIH and HIRA) for cost–benefit analysis. The average medical costs of a patient with P. vivax malaria diagnosed by microscopy alone and both microscopy and RDT were also compared. Data from the NHIIH guaranteed high reliability by directly calculating the actual medical expenses. The HIRA data had a disadvantage in that it was not possible to accurately specify the use of RDTs. Still, it had the merit of providing the average medical costs across the country because the HIRA reviews claims submitted by all healthcare providers. The results from this dataset showed trends similar to those of the results of the cost–benefit analysis using NHIIH data. Analysis using both data sources showed that the impact of RDTs on the cost–benefit and overall medical expenditures accumulated over time. In South Korea, all citizens are under the National Health Insurance Service funded by contributions, government subsidies and tobacco surcharges. The national government provides 14% of the total amount of funding, and the total expenditure on health insurance has increased annually.32 Since the increase in medical expenses is not just a problem in South Korea, efforts to reduce overall medical expenses are important, and we believe the results of our study can help in this regard.
This study has several strengths. First, we developed a dynamic compartmental mathematical model that could obtain results for more comprehensive impacts of RDT. Through this model, we could implement the transmission dynamics of P. vivax malaria so that we could estimate the impact of RDT introduction on overall future malaria incidences and national medical expenditures. Second, the malaria transmission model was designed through a set of values based on real data and fitting processes according to actual occurrences. The reduction in diagnostic time due to the use of RDTs obtained by analysing the actual hospital data also improved the reliability of the simulation. The cost–benefit analysis estimated the average cost per capita based on actual hospital data, and the reliability increased through the validation process using data from the entire country. Lastly, the sensitivity analysis demonstrated how the IBCR could change in various situations.
Despite the above strengths, this study has some limitations. First, the dynamics of mosquito vectors for P. vivax malaria have been insufficiently studied. Thus, although we referred to foreign papers, these data are not necessarily consistent with Korean mosquito dynamics even after correcting for the Korean environment. Second, relapse incidences were not accurately addressed, as described previously,31 since we mainly focused on the effects of RDTs. Third, this study did not consider future climate change scenarios since we estimated incidences for a relatively short period. Although the results were sensitive to mosquito dynamics that depend on climate changes, the influence of RDTs would be more critical in the global warming scenario. Fourth, we estimated the benefit indirectly from the summed medical cost data as we were unable to directly estimate the benefit from the data. Fifth, in HIRA data, the definitions of P. vivax malaria diagnosis by microscopy alone and both microscopy and RDT were made by researchers based on the time of RDT introduction. Still, it was difficult to completely classify the two test groups.
Conclusions
The introduction of RDTs can prevent new cases of P. vivax malaria by reducing the diagnostic time. RDTs also proved beneficial in the cost–benefit analysis and effects accumulated with increasing years. This not only meets the medical need to reduce the number of new cases but also contributes to the reduction of overall medical expenditures. Therefore, more active efforts are needed for the widespread adoption and use of RDTs.
Supplemental material
Supplemental material
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Lei Si
JHK and JS contributed equally.
JL and JSY contributed equally.
Contributors RK, HK, JL and JSY conceived the study and contributed to project administration. JHK, JS, CK, JL and JSY performed the primary modelling analysis. JHK, JS, JL, and JSY wrote the model supplements. JHK, JS, WJL, HC, and J-DK contributed to data collection. JHK and JS wrote the first draft of the report. JHK, JS, CK, JYC, RK, HK, JL and JSY contributed to the study design. All authors contributed to data interpretation and revision of the report.
Funding This study was supported by the National Evidence-based Collaborating Agency of South Korea (NECA-R-19-005).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study complies with the Declaration of Helsinki and was approved by the institutional review board (IRB) at National Evidence-based Healthcare Collaborating Agency of South Korea (NECAIRB19-012-4). Informed consent from the participants was waived by the IRB because of the pure observational nature of the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. The data analysed during the study are presented in the article and its online supplemental materials.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.