Article Text

Abstract
The End TB Strategy envisions a world free of tuberculosis—zero deaths, disease and suffering due to tuberculosis by 2035. This requires reducing the global tuberculosis incidence from >1250 cases per million people to <100 cases per million people within the next two decades. Expanding testing and treatment of tuberculosis infection is critical to achieving this goal. In high-burden countries, like India, the implementation of tuberculosis preventive treatment (TPT) remains a low priority. In this analysis article, we explore potential challenges and solutions of implementing TPT in India. The next chapter in tuberculosis elimination in India will require cost-effective and sustainable interventions aimed at tuberculosis infection. This will require constant innovation, locally driven solutions to address the diverse and dynamic tuberculosis epidemiology and persistent programme monitoring and evaluation. As new tools, regimens and approaches emerge, midcourse adjustments to policy and practice must be adopted. The development and implementation of new tools and strategies will call for close collaboration between local, national and international partners—both public and private—national health authorities, non-governmental organisations, research community and the diagnostic and pharmaceutical industry. Leading by example, India can contribute to global knowledge through operational research and programmatic implementation for combating tuberculosis infection.
- Tuberculosis
- Chemoprophylaxis
- Prevention strategies
- Public Health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
An estimated 354 million people are latently infected with tuberculosis in India and form the next generation of future tuberculosis cases.
TB preventive treatment (TPT) can reduce rates of progression from infection to active TB disease by 90%. Yet in many high-burden countries, like India, the implementation of TPT remains a low priority, is underused and often avoided in practice.
TPT will play a major role in bending the epidemiologic curve in India and will require constant innovation, locally-driven solutions, and persistent programme monitoring and evaluation.
Leading by example, India can contribute to global knowledge of TPT through research and programmatic implementation.
Introduction
In 2014, the World Health Assembly set global targets for tuberculosis (TB) prevention, care and control,1 serving as the impetus for the End TB Strategy.2 This ambitious strategy envisions ‘a world free of tuberculosis—zero deaths, disease, and suffering due to tuberculosis’ by 2035.2 TB elimination requires reducing the global TB incidence from >1250 cases per million people to <100 cases per million people within the next two decades.3 The WHO developed a framework for low-incidence countries for achieving tuberculosis elimination.4 This framework focused on several key tenets: systems strengthening (eg, political commitment, funding, surveillance, programme monitoring and evaluation), accelerating case detection and ensuring efficacious treatment (eg, relapse-free cure and preventing the acquisition of drug resistance) and preventing future cases (eg, reducing transmission, infection control, contact tracing, testing and treatment of tuberculosis infection and vaccination).4 It was hoped that the lessons learnt in low-incidence countries could be translated to high-burden countries.5 This may not be effective, as experiences in Australia, Europe and North America are likely different, given the epidemiology of tuberculosis is driven by immigration and large number of cases attributed to reactivation of tuberculosis infection.6–8 Moreover, some key interventions being planned in high-resource areas may not be practical to implement elsewhere without substantial investment and additional human resources.
Bending the epidemiological curve
The path to global tuberculosis elimination is based on mathematical modelling.9 The WHO predicts that optimising current tools (eg, rapid molecular diagnostics, modifying current treatment regimens to increase adherence) and improvements in universal access to health coverage will reduce the annual incidence rate of TB by 10% per year by 2025.9 However, the steepest rate of decline is expected with introduction of new drugs and treatment regimens for active TB, tuberculosis preventive treatment (TPT) and ultimately—an effective vaccine to prevent TB infection or activation to TB disease.9 Until then, it is up to TB control programmes to design interventions to best identify and treat the estimated 1.7 billion people worldwide that are latently infected with TB and form the next generation of future tuberculosis cases.10 Planning for this next era of tuberculosis prevention in high-burden countries—that is, increased focus on diagnosis and treatment of tuberculosis infection—needs to happen now, rather than later, if we are to achieve our global targets.
Rationale for targeted testing and treatment of tuberculosis infection
The concept of TPT began more than half a century ago.11–13 During 1957–1977, aggressive community-wide implementation of TPT in the Yukon-Kuskowim River delta of Alaska reduced TB incidence by 17% per annum14 15—a rate similar to the targeted declines needed today to reach global elimination. Several well-designed clinical trials have since validated several regimens as an effective and safe way to prevent future TB disease.16 17 The benefit of preventing individuals from progressing to active TB, especially persons at high risk of reactivation, is widely accepted.18 Available treatment, when taken appropriately, can reduce rates of progression from infection to active disease by 90%.18 Yet in many high-burden countries, like India, the implementation of TPT remains a low priority, is underused, and often avoided in practice.19
Challenge 1—Burden
India has an estimated annual tuberculosis incidence of 2170 cases per million people.20 The top priority for the Revised National Tuberculosis Programme, India (RNTCP) is to detect, treat and monitor people with active TB disease. This is an enormous task. In 2016, 1.7 million TB cases reported to the government,20 an estimated 2.2 million cases were presumed to have received care in the largely unregulated private sector.21 ,22 Several key strategies have been outlined in the RNTCP National Strategic Plan 2017–2025 (NSP) to address this burden.23 If this plan is funded and executed appropriately,22 India is poised to make substantial progress towards finding missing cases more quickly, ensuring universal drug susceptibility testing, implementing the most efficacious regimen, ensuring treatment adherence and monitoring relapse through surveillance. However, recent models suggest that focus on TB disease alone has a limited impact on the reduction in future incidence without the additive effect of TPT.24 Assuming a conservative average of four household contacts per case and 50% tuberculosis infection rate among them,25–31 an estimated 4 million new tuberculosis household infections occur in India every year. Without further action and investment, 28 million new tuberculosis household infections will occur by 2025 (table 1). Many millions more will also emerge from the huge reservoir of an estimated 354 million people previously infected with tuberculosis in India.10
Potential burden of latent tuberculosis infection among household members by antituberculosis drug resistance profile, India—2016
Challenge 2—Identifying persons for tuberculosis preventive treatment
In practice, TPT in India is based on ruling out active disease (as opposed to detecting infection) and then offering prophylaxis to those without active disease among high-risk populations, such as children aged <6 years and persons living with HIV. Expanding TPT in India will require a frameshift in the design and implementation of contact tracing activities and also the more regular use of diagnostic tests for tuberculosis infection. It is worth noting that the positive predictive value of all current diagnostic tests for tuberculosis infection are dependent on the pretest probability of progressing to disease.32 33 It is neither practical nor appropriate to conduct wholesale testing in the general population. The vast majority of persons with tuberculosis infection will never progress to active tuberculosis disease.18 33 Testing for tuberculosis infection with the current tools, among persons who are otherwise healthy and have low risk of progressing to disease, would be low yield, and incur a high implementation cost. Therefore, rational, evidence-based, targeted testing would be a more appropriate and cost-effective strategy.
Accordingly, the NSP calls for prioritising screening for tuberculosis infection among people living with HIV, paediatric contacts of sputum-smear positive index cases, and persons with clinically indicated risk (eg, persons receiving long-term immune-suppressants, corticosteroid use, diabetes mellitus, silicosis, and the undernourished).23 Indeed these groups are at high-risk of progressing to disease, but two additional important groups should also be considered: all household contacts (regardless of age) and healthcare workers at greatest risk of exposure to patients with infectious TB. India must transition from ruling out active disease to detecting tuberculosis infection, from passive screening that places responsibility on the patient and household member to present for care, to actively screening contacts at places and times convenient to them.34 In addition, the current strategy for screening healthcare workers focuses on finding active disease. Preventing tuberculosis infection among healthcare workers will require two important components—improved airborne infection control in all health facilities as well as actively screening and treating tuberculosis infection—including periodic surveillance for new tuberculosis infection (suggesting recent transmission) among healthcare workers. It should be emphasised that while TPT will offer some reduction in risk of progression to disease, the risk of repeat exposure and subsequent reinfection will remain high, lowering the yield of preventive efforts, unless all aspects of airborne infection control (ie, administrative measures, environmental controls and the routine use of personal respiratory-protection equipment)35 36 and contact tracing are implemented effectively.37 The recently endorsed F-A-S-T strategy (Finding TB cases Actively, Separating safely and Treating effectively) may prove useful in implementing TB airborne infection control throughout the Indian healthcare system.38
Challenge 3—Development and adoption of new diagnostic tools
India has been slow to adopt recent technologies to diagnose tuberculosis infection. As a national policy, RNTCP relies on the tuberculin skin test (TST) to detect infection.39 The TST has several limitations. Poor reproducibility, with inter-reader and intrareader variability in measurement, the requirement of two patient visits separated by 48 to 72 hours, and high false-positive rate among persons who received bacillis Calmette-Guérin (BCG) vaccination have been reported.40 Interferon-gamma release assays (IGRAs) offer some advantages over the TST, but these are also imperfect tests.41 IGRAs appear to have greater specificity than TST in BCG-vaccinated populations.42 Despite the in vitro design and standardisation protocols for IGRA, substantial variability in test reproducibility has been reported.41 43–47 Product cost, technical complexity and limited commercial availability of IGRA cast doubt to whether IGRA-based screening strategies are more cost effective than TST-based strategies in high-burden settings.48 49 To further complicate matters, WHO and the RNCTP banned the use of serological testing (eg, tests for antibodies IgA, IgG, IgM) as diagnostic tools for tuberculosis disease.50 51 This ban may have caused confusion in the utility of blood-based IGRAs for detecting tuberculosis infection, especially in the private sector.52 Also, there is a persistent shortage of quality-assured purified protein derivative (PPD), the substance used during TST.53 The unstable supply of quality-assured PPD has likely resulted in fewer persons tested and increased use of alternative diagnostic products of dubious quality. Further operational research is needed to optimise the diagnosis of tuberculosis infection. Establishing which test, if any, is the most appropriate test to use in India is a top priority. There is an urgent need for a reliable, cost-effective test to rapidly detect tuberculosis infection and identify those most likely to benefit from preventive treatment.
Challenge 4—Tuberculosis preventive treatment acceptance, adherence and completion
The initiation and adherence to TPT has been historically poor.54–61 This may be a result of lack of general awareness and perceived risk,56 60 61 non-availability of standard tuberculin product,56 59 drug stock-outs (including pyridoxine),57 58 limited access to radiography (to exclude TB disease),56–59 long duration of therapy (in absence of symptoms) and poor programmatic monitoring.54 56–60 Moreover, in India, the practice of TPT is predominately for children.39 55–59 In the few studies that enrolled adult participants, TPT acceptance rates were exceptionally low (17%)61 or treatment was not offered because of perceived high background tuberculosis infection prevalence, risk of repeated exposure and reinfection, risk of drug toxicity and concerns of widespread isoniazid monoresistance in India.60 61 All of these concerns are relevant. The risk of drug intolerance and severe toxicity, although worrisome, were infrequent in other settings, and appear to be age-associated, or found among persons with other risk factors for hepatotoxicity (eg, excessive alcohol use).16 62–64 In some high-prevalence TB settings, where the risk of reinfection is high, studies have demonstrated benefit of preventive treatment with longer durations.65 66 A study from Chennai found that both 6-month and 36-month isoniazid preventive treatment regimens among HIV-infected persons was equivalent in safety, tolerance and effectiveness.67 The optimal length of TPT in India remains unknown (eg, extended duration regimens to cover reinfection vs shorter adherence-friendly regimens) and is likely subject to feasibility and other logistical considerations. High rates of treatment completion (87%) were recently reported in routine practice using a 12-dose weekly isoniazid and rifapentine regimen (3HP) in a low-prevalence country.68 This treatment holds promise to improve acceptance and adherence to TPT worldwide;69 however, the efficacy of 3HP among populations with a high prevalence of drug resistance remains unknown. Indeed, drug resistance in India is also a concern. The recent nationally representative antituberculosis drug resistance survey found that 11% of new and 25% previously treated patients had a form of isoniazid-resistant tuberculosis.70 These results, when extrapolated to estimated number of new household contacts with tuberculosis infection, suggest that millions of persons every year may not benefit from the various regimens designed to halt the progression from infection to active forms of drug-resistant tuberculosis (table 1). Unfortunately, there is no diagnostic test that can assess the drug susceptibility profile of any given infection (non-active TB), and there are no published randomised clinical trials for the treatment of tuberculosis infection caused by isoniazid-resistant or multidrug-resistant (MDR) forms of tuberculosis.16 However, several alternative preventive regimens are available.16 71 Contacts of patients with isoniazid-monoresistant TB have been successfully treated with rifampicin-based regimens72 73 and support the current recommendations to use 4 months of daily rifampicin under certain conditions.16 71 Among MDR TB contacts, fluoroquinolone-based preventive treatment may be considered,74 global treatment guidelines are forthcoming,75 but further research is needed prior to wide-scale use,76—especially in India where overconsumption77 and uncontrolled use of fluoroquinolones has been reported.78–80 It is unclear which TPT regimen would be most effective in India. We must establish which TPT regimens are most effective in India, with careful consideration of posology and duration for children and adults. Notwithstanding, all persons offered TPT must be thoroughly evaluated to rule out active disease, assessed to select an appropriate treatment course (including careful review of potential exclusion conditions) and closely monitored for the development of treatment-related adverse events and poor adherence.
Way forward
Given the above burden and challenges, expanding the identification and treatment of tuberculosis infection in India might seem overwhelming and unachievable. However, incremental progress towards elimination is possible with careful evidence-guided policy development, planning and implementation.81 Table 2 describes the major challenges to implementing treatment of tuberculosis infection in India, and highlight potential solutions.
Potential challenges and solutions to tuberculosis preventive treatment implementation, India
Multinational political will and leadership is warranted to finance our ambitious global TB elimination efforts. The identification, testing and monitoring of TPT will require substantial increases in the number of programme personnel, training and education for healthcare providers and patients, diagnostic and drug procurement (ie, TST, IGRA, pyridoxine, rifapentine), resources to build and expand diagnostic and laboratory capacity and surveillance mechanisms. It is critical to ensure that TPT initiatives do not divert resources from essential and expanding commitments devoted to persons with TB disease. Wide-scale implementation is not advisable without sufficient resources to ensure that most patients complete the full cascade of TPT.
Tuberculosis in India is very heterogeneous, both from an epidemiological perspective and in terms of programmatic performance. Results from subnational tuberculosis prevalence surveys (ie, active disease),82–87 subnational and district-level annual rate of tuberculosis infection surveys88 and analysis of routinely collected programme surveillance data54 89 90 reveal substantial local variation in tuberculosis incidence, tuberculosis prevalence, rates of HIV coinfection, drug-resistant forms of TB and utilisation of TB services in the private sector. There are enormous epidemiological and programmatic differences between urban and rural areas. For example, urban areas are characterised by lower tuberculosis prevalence but higher annual risk of tuberculosis infection, while rural areas are characterised by higher tuberculosis prevalence and lower annual risk of tuberculosis infection.88 89 91 Thus, the design of effective, targeted, TPT interventions cannot be ‘one-size-fits-all’, but rather tailored to local epidemiology and programme performance. For example, ruling out active tuberculosis disease, an essential component of TPT, is particularly challenging in remote areas that do not have access to radiography or qualified personnel for interpreting radiography and experience logistic issues with transporting sputa over long distances (ie, non-viable and contaminated specimens). Initiating single-drug TPT for patients with active tuberculosis could result in acquired resistance and further prolong infectiousness.92 Simple, easy-to-use algorithms for determining TPT eligibility, appropriate regimen and length of treatment should be developed based on individual risk, local epidemiology and programmatic performance.
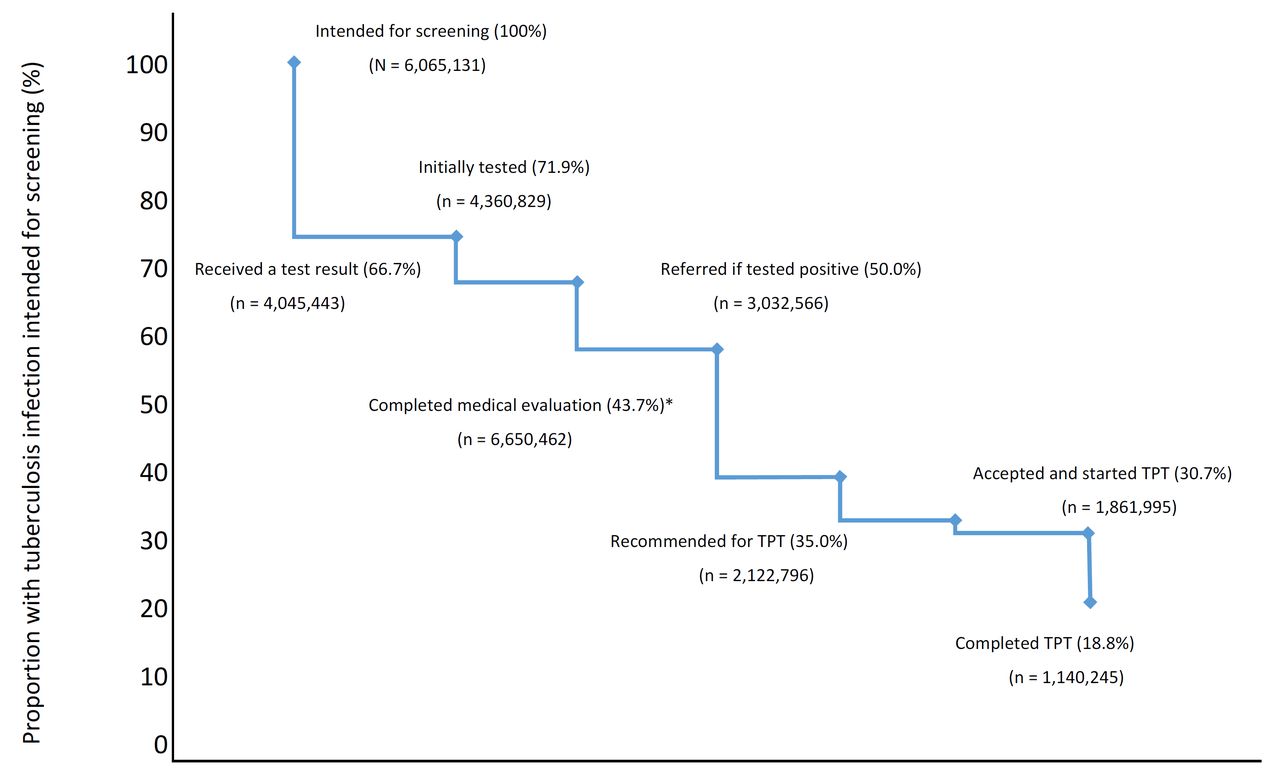
There remains a paucity of data for several programmatically relevant research questions within the Indian context. The Government of India, implementing partners, and stakeholders should consider addressing several, key operational research questions to inform policy and practice table 3.93 Implementation research focused on improved diagnostics to identify tuberculosis infection and effectively predict progression from infection to active disease; the performance and tolerability of shorter, adherence-friendly preventive regimens; optimal length of treatment (given potential risk of re-exposure); accurate estimates of local tuberculosis infection burden; improved mechanisms for monitoring programme performance and assessing cost effectiveness are top priorities. Research alone cannot stimulate change, however. Findings from these studies must be translated into sustainable policies that are adequately funded and effectively implemented in practice. The adoption of a standardised method of monitoring, such as the use of a tuberculosis prevention cascade (figure 1), may prove useful to objectively assess progress of the programmatic implementation of tuberculosis infection treatment.94 95 There are many opportunities for losses in the continuum of care for tuberculosis infection diagnosis and treatment.94 95 People with tuberculosis infection might not be identified for screening, and even if they are, many are not tested, or a test might be placed but results are not received by treating clinicians. Patients who test positive of tuberculosis infection may not be able to complete the required medical evaluation (eg, symptom review, chest radiograph), clinicians might opt not to initiate treatment (eg, lack of knowledge, drug intolerance, clinical contraindications) and patients may be unable to complete a full course of treatment. Prevention cascades can objectively identify these gaps, help develop strategies for effective interventions and offer opportunities to improve success.95 Cascades can also shift programme goals away from estimating coverage in the population served to making direct quantitative measurements of patient retention at each step of tuberculosis service delivery.96 Recent upgrades to the RNTCP web-based reporting system, NIKSHAY,97 may be a viable platform to develop and monitor district-level tuberculosis prevention cascades throughout India.
Guidelines for implementing a national tuberculosis preventive treatment programme in India

{kind=link}
Potential losses at each stage of the TPT cascade. *Includes ruling out active tuberculosis. The values were based on the estimated number of household contacts exposed to pansensitive M. tuberculosis per year in India (table 1). Percentage lost at each stage was based on the meta-analysis of Alsdurf et al.95 TPT, tuberculosis preventive treatment.
India must address the major gaps previously identified in the cascade of care for TB disease98 and improve access and the quality of TB service delivery in the public, private and informal sectors99–101 prior to nationwide implementation of TPT. To achieve elimination, the national TB programme must take a phased multipronged approach to TB prevention and care. The first priority is continued progress to ensure early, accurate, tuberculosis diagnosis for all persons suffering from tuberculosis. All patients with tuberculosis must also be evaluated for antituberculosis drug resistance, placed on the most appropriate treatment regimen and properly managed and followed to treatment completion. In addition, simultaneous improvements to airborne infection control measures, contact tracing and targeted TPT for children and persons living with HIV must continue. The cascade of TPT among these groups should be thoroughly assessed. These data can inform a more effective implementation at each step of care. As access to quality TB diagnosis and care improves, antituberculosis treatment success rates increase, and TB incidence and prevalence decline and targeted TPT may be expanded to other high-risk groups.
Conclusion
Over the past decade, India has accomplished numerous impressive achievements in tuberculosis prevention, care and control. The RNTCP has screened more than 80 million people for tuberculosis, successfully treated 15 million patients and saved millions of lives.102 Leading by example, India can contribute to the global knowledge of TPT through research and programmatic implementation. The next chapter in tuberculosis elimination in India will require evidence-based, cost-effective and sustainable interventions. TPT will play a major role in bending the epidemiological curve in India. This will require constant innovation, locally driven solutions, and persistent programme monitoring and evaluation to address the diverse and dynamic tuberculosis epidemiology. As new tools, regimens and approaches emerge, midcourse adjustments to policy and practice must be quickly adopted and sufficiently resourced. The development and implementation of new tools and strategies will call for close collaboration between local, national and international partners—both public and private—national health authorities, non-governmental organisations, research community and the diagnostic and pharmaceutical industry. Together our collective effort will end tuberculosis in our lifetime.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
Footnotes
PKM and SAN contributed equally.
Handling editor Alberto L Garcia-Basteiro
Contributors PKM and SAN conceived, designed and drafted the initial manuscript. PKM, VKC, JEO acquired and analysed the data. RA, CH, THH and DS provided technical support to interpreting the results. RA, VKC, PD, UDG, CH, THH, AK, NK, PK, SAM, SRM, JEO, CNP, MMP, KKR, RR, RR, VSS, RS, SS, KSS, SS, RS, DS, JT, SPT and SDK revised the initial draft and provided critically important intellectual content. PKM and SAN integrated all feedback and investigated and resolved any questions from internal and required clearance at CDC and WHO prior to publication. SDK provided overall leadership and oversight. All authors attest to the accuracy and integrity of final version.
Funding This study was funded in part by U.S. President’s Emergency Plan for AIDS Relief.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unless otherwised stated, all data presented are in the public domain and freely avaialble for use.