Article Text

Statistics from Altmetric.com
The sex gap in early-age death is one of the most important sources of child inequality in all societies, and it carries negative social consequences in the long run. In the absence of gender discrimination in the allocation of foods and heath resources, mortality rates are higher in boys than in girls.1–3 Recent studies however suggest that in sub-Saharan Africa, the general improvement in state capacity and the quality of political and democratic institutions has had stronger health benefits for boys, reducing the male-female gap in early-age mortality.4 5 Democratic indicators such as political participation, competitiveness in the recruitment of the executive and constraints on executive power substantially improved after 1990. These positive developments led to an improvement in the quality of public health institutions. Mabeu and Pongou’s research implies that the health benefits of these positive institutional changes have mostly accrued to boys, in part because these changes have helped constrain the negative influences of the male biological make-up on mortality.5 But this pattern was likely to be specific to HIV-unexposed children. Among HIV-exposed children, it seems that other forces were at play.
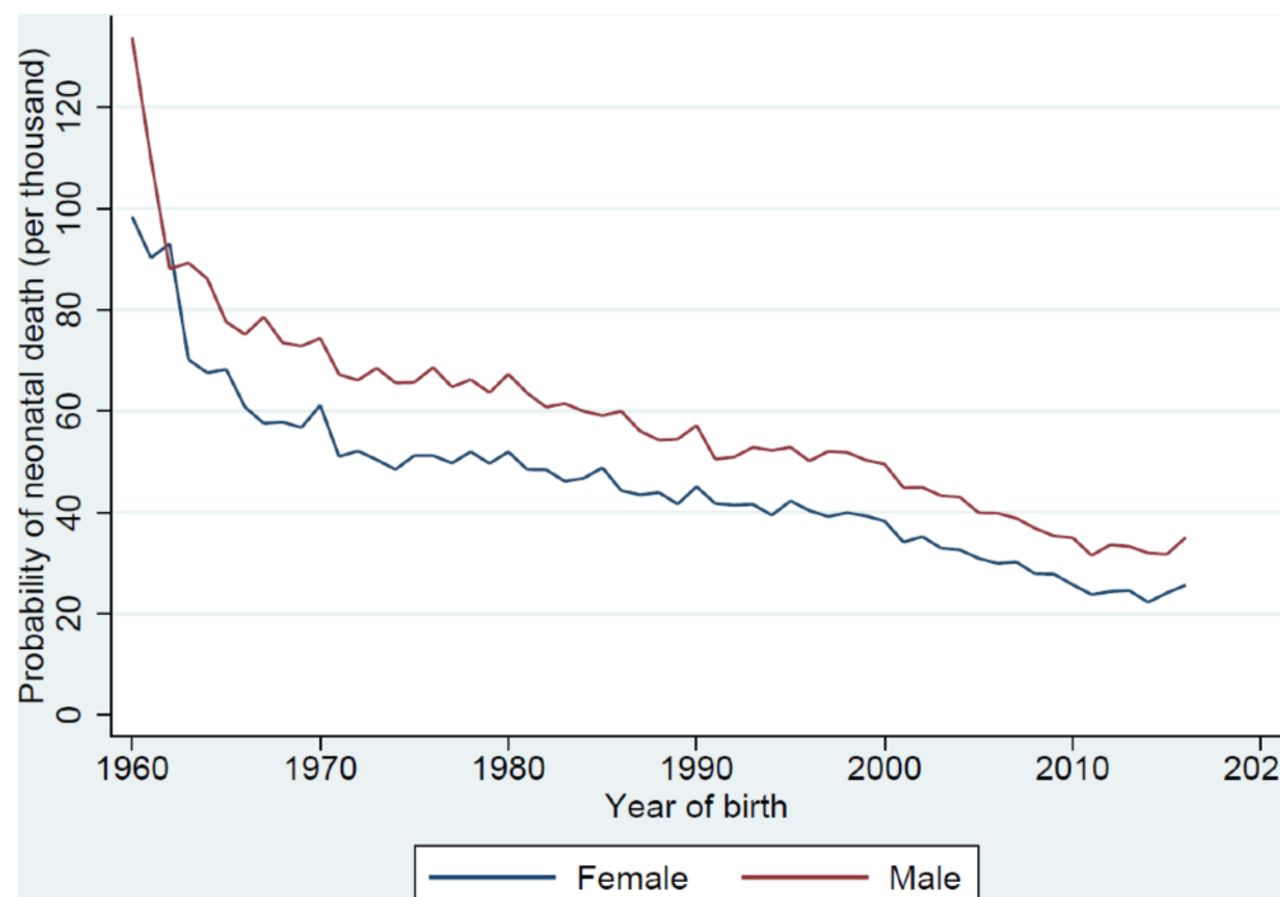
In this editorial, we analyse trends in the sex gap in neonatal death—death occurring within 1 month of birth-during the era of the AIDS epidemic, and argue that they were sensitive to the availability of antiretroviral medicines. Child exposure to HIV (during pregnancy, delivery and breast feeding) reduced the female survival advantage, but this situation was gradually reversed by the availability of antiretroviral treatment. Our argument is partly captured in figure 1, which shows unadjusted trends in the probability of neonatal death over the period 1960–2017 for both boys and girls in sub-Saharan Africa. Neonatal mortality declined substantially over this period for both sexes. However, as figure 2 shows, the decline was more important for male children, especially between 1980 and 2008, a period corresponding to one in which antiretroviral therapy was either non-existent or low.

Unadjusted trends in the probability of neonatal death for male and female children in sub-Saharan African countries, 1960–2017. Note: This figure is based on a sample of 4 134 851 live births from 129 Demographic and Health Surveys collected in 40 sub-Saharan African countries between 1986 and 2017. Children born within 1 month of the survey were withdrawn to allow for full exposure to neonatal death.

Unadjusted trends in the male-female difference in the probability of neonatal death in sub-Saharan African countries, 1960–2017. Note: This figure is based on a sample of 4 134 851 live births from 129 Demographic and Health Surveys collected in 40 sub-Saharan African countries between 1986 and 2017. Children born within 1 month of the survey were withdrawn to allow for full exposure to neonatal death.
In order to understand the patterns described in figure 2, one needs to understand the forces that shape the sex gap in mortality, and how these forces interact with HIV/AIDS exposure and the antiretroviral treatment. Excess male mortality is explained by both preconception and biological factors.3 6 The biological explanation partly draws on the chromosomal XY sex determination system.7 8 It is argued that XY chromosomes are more susceptible to X-linked recessive disorders than are XX chromosomes, which implies a higher incidence of infectious and non-infectious diseases in boys, and hence a greater probability of death.1 2 9 The preconception origins hypothesis extends the biological hypothesis, and holds that some of the preconception environmental factors that determine the sex of a child also explain sex differences in early-age survival.3 6 It provides a broader framework for understanding how sex disparities in morbidity and mortality vary across societies and over time. Testing this hypothesis on twin data from sub-Saharan Africa, Pongou found that preconception differences explain 40%–52% and biological differences explain 48%–60% of the male-female gap in infant mortality.3
If girls are more likely than boys to survive in early ages (figure 1), what explains the fact that their survival advantage decreased in the era of the AIDS epidemic as shown in figure 2? We argue that part of the explanation lies in the greater vulnerability of girls to HIV infection. Indeed, it is now known that the mother-to-child transmission (during pregnancy, delivery and breast feeding) of HIV, which is the leading mode of acquisition of HIV infection among children, is higher in female children than in their male counterparts.10–12 In a case study in Uganda,10 Brahmbhatta et al found that female children were significantly more likely to be infected with HIV perinatally compared with male children, with the probability of mother-to-child transmission being 20.8% for the former and 12.4% for the latter. Similarly, Thorne and Newell found that girls were at a 1.5 times increased risk of mother-to-child transmission of HIV than boys, although their finding was limited to children born by elective caesarean section deliveries.11 Biggar et al also obtained similar results for babies born to HIV-infected and untreated women in Malawi.12 Interestingly, all of these studies found that the sex difference in the risk of mother-to-child transmission of HIV is mainly significant in utero.
The documentation of the theoretical explanation for this phenomenon is still very limited. Two main hypothetical explanations emerge from the literature. The first holds that HIV-infected male fetuses are more likely to die in utero and are therefore missing at birth, which is the main reason why a higher prevalence of HIV infection is observed in female births than in male births.10 12 13 The second explanation holds that hormonal, genetic or environmental factors may make women more susceptible to HIV infection in utero.12 13 For instance, Biggar et al explain that minor histocompatibility reactions between maternal lymphocytes and infant Y chromosome-derived antigens reduce the risk of HIV transmission in boys.12
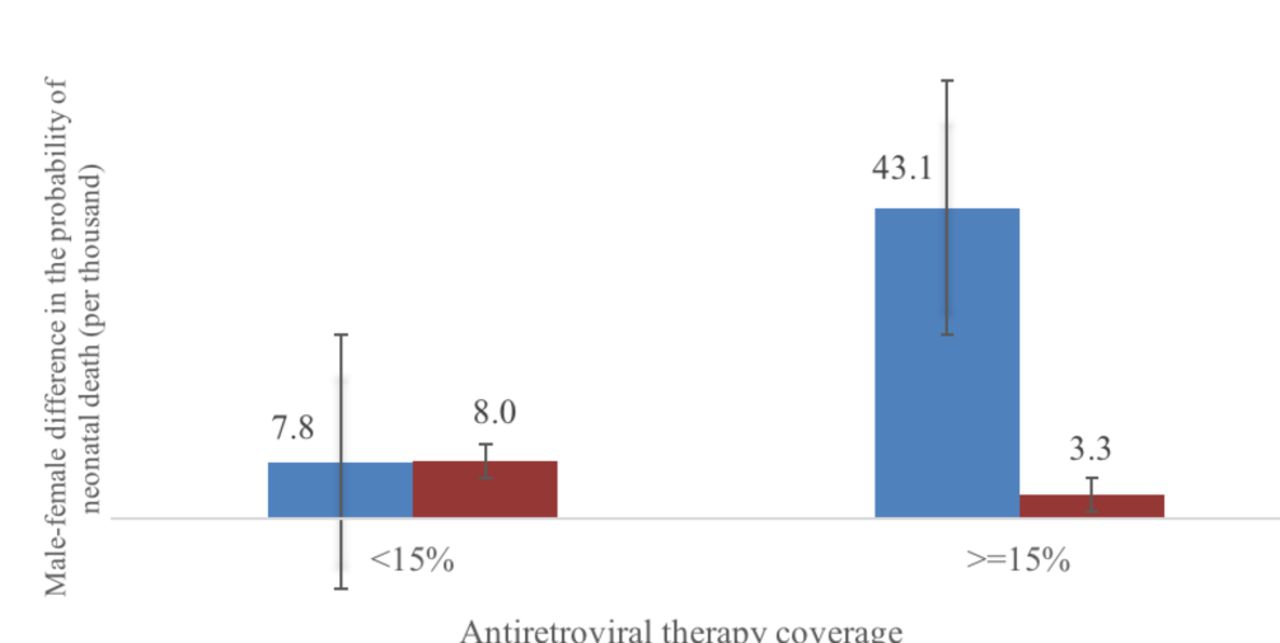
The higher prevalence of HIV in female births than in male births translates into a greater risk of HIV death in girls than in boys, given the positive effect of HIV infection on mortality among children.14 This greater susceptibility of girls to HIV basically diminishes their natural survival advantage over boys, especially in the absence of the antiretroviral therapy. Indeed, it is estimated that the rate of mother-to-child transmission of HIV is between 30% and 45% if the mother is not receiving any antiretroviral medicines. But as antiretroviral treatment becomes available, the mother-to-child transmission of HIV is largely prevented, reducing HIV-related death among children and helping girls to regain their survival advantage over boys. This pattern is captured in figure 3, which shows the male-female difference in the probability of neonatal death for HIV-exposed and HIV-unexposed children by the level of the antiretroviral therapy coverage in a sample of sub-Saharan African countries. Clearly, the male-female difference in the probability of neonatal death that is attributable to in utero HIV exposure is greater when the antiretroviral therapy coverage is higher.

Male-female difference in the probability of neonatal death for HIV-exposed and HIV-unexposed children by level of antiretroviral therapy coverage. Error bars represent 95% CI around the mean. Note: This figure is based on individual-level data on children and maternal HIV status from Demographic and Health Surveys conducted in Cameroon (2004; 2011); Ghana (2003; 2014); Guinea (2005; 2012); Kenya (2003; 2008–2009); Lesotho (2004–2005; 2009–2010; 2014); Malawi (2004–2005; 2010); Rwanda (2005; 2010–2011; 2014–2015); and Zimbabwe (2005–2006; 2010–2011; 2015). These data are combined with country-by-year-level data on the antiretroviral therapy coverage provided by US President’s Emergency Plan for AIDS Relief (PEPFAR). Each of the countries is represented in each of the two groups defined by the level of coverage of the antiretroviral therapy, which enhances the comparability of these groups. In order to identify children exposed in utero to HIV, we restricted the analysis to children born at most 3 months before the survey. Children born within 1 month of the survey were withdrawn to allow for full exposure to neonatal death.
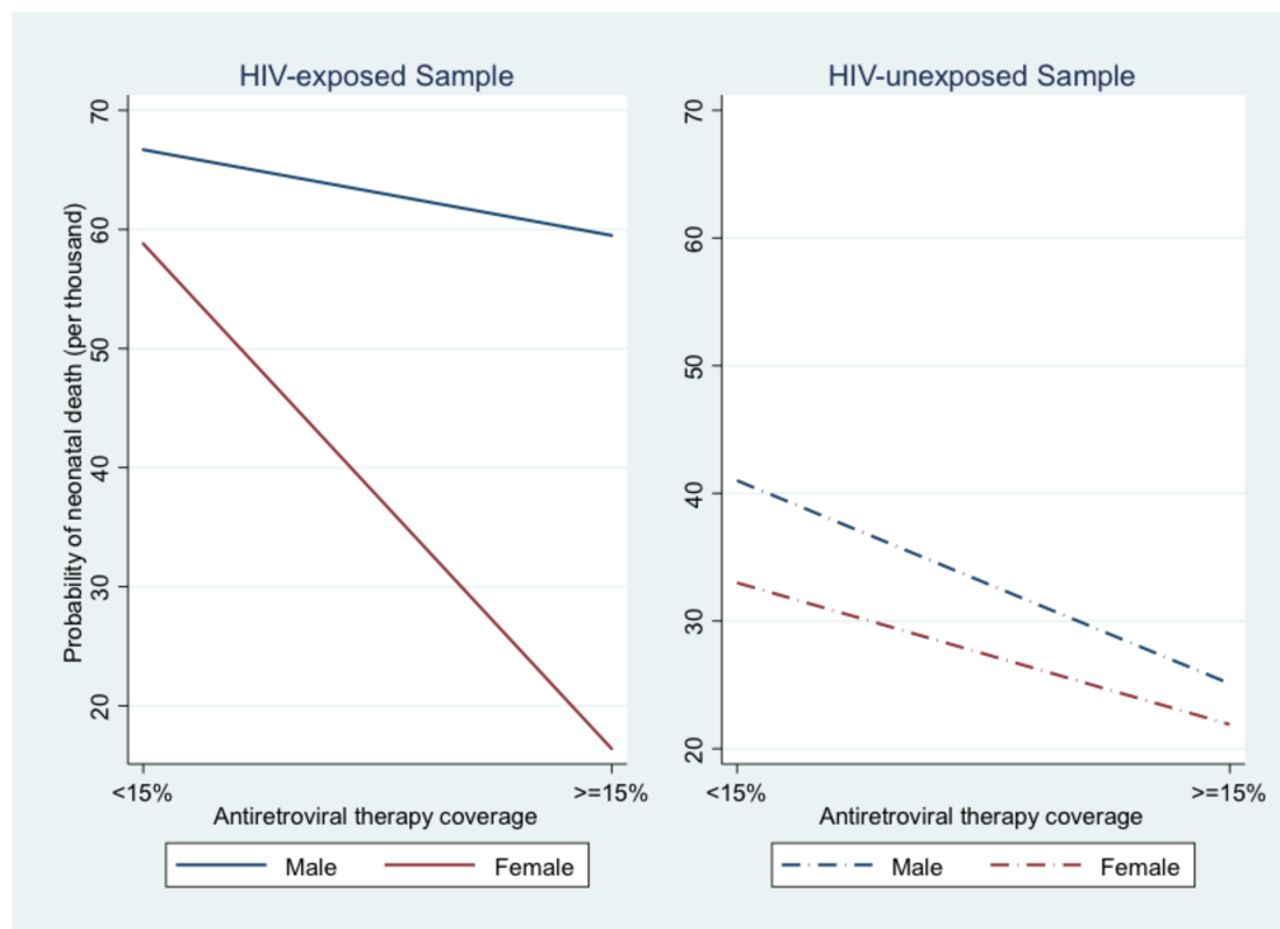
With less than 15% of antiretroviral therapy coverage, the male-female difference in the probability of neonatal death is a bit lower among HIV-exposed children compared with their unexposed counterparts. This might reflect the fact that when treatment is absent or low, the negative effect of HIV exposure is greater for girls than for boys. However, with at least 15% of antiretroviral therapy coverage, the male-female difference in mortality risk is greater for HIV-exposed children compared with unexposed children. In fact, as shown in figure 4, with a greater treatment coverage, the mortality risk of HIV-exposed girls falls from 58.8/1000 to 16.4/1000 (vs 33.0/1000 to 21.9/1000 for HIV-unexposed girls); but that of HIV-exposed boys only falls from 66.7/1000 to 59.5/1000 (compared with a fall from 41.0/1000 to 25.1/1000 among HIV-unexposed boys). It has been shown that antiretroviral treatment increases the likelihood of adverse birth outcomes in HIV-exposed uninfected children,15 and it is possible that this has a greater effect on the mortality of boys than that of girls. This could explain the fact that greater treatment coverage substantially widens the sex difference in mortality (figure 3).

Probability of neonatal death for HIV-exposed and HIV-unexposed male and female children by level of antiretroviral therapy coverage. Note: This figure is based on individual-level data on children and maternal HIV status from Demographic and Health Surveys conducted in Cameroon (2004; 2011); Ghana (2003; 2014); Guinea (2005; 2012); Kenya (2003; 2008–2009); Lesotho (2004–2005; 2009–2010; 2014); Malawi (2004–2005; 2010); Rwanda (2005; 2010–2011; 2014–2015); and Zimbabwe (2005–2006; 2010–2011; 2015). These data are combined with country-by-year-level data on the antiretroviral therapy coverage provided by US President’s Emergency Plan for AIDS Relief (PEPFAR). Each of the countries is represented in each of the two groups defined by the level of coverage of the antiretroviral therapy, which enhances the comparability of these groups. In order to identify children exposed in utero to HIV, we restricted the analysis to children born at most 3 months before the survey. Children born within 1 month of the survey were withdrawn to allow full exposure to neonatal death.
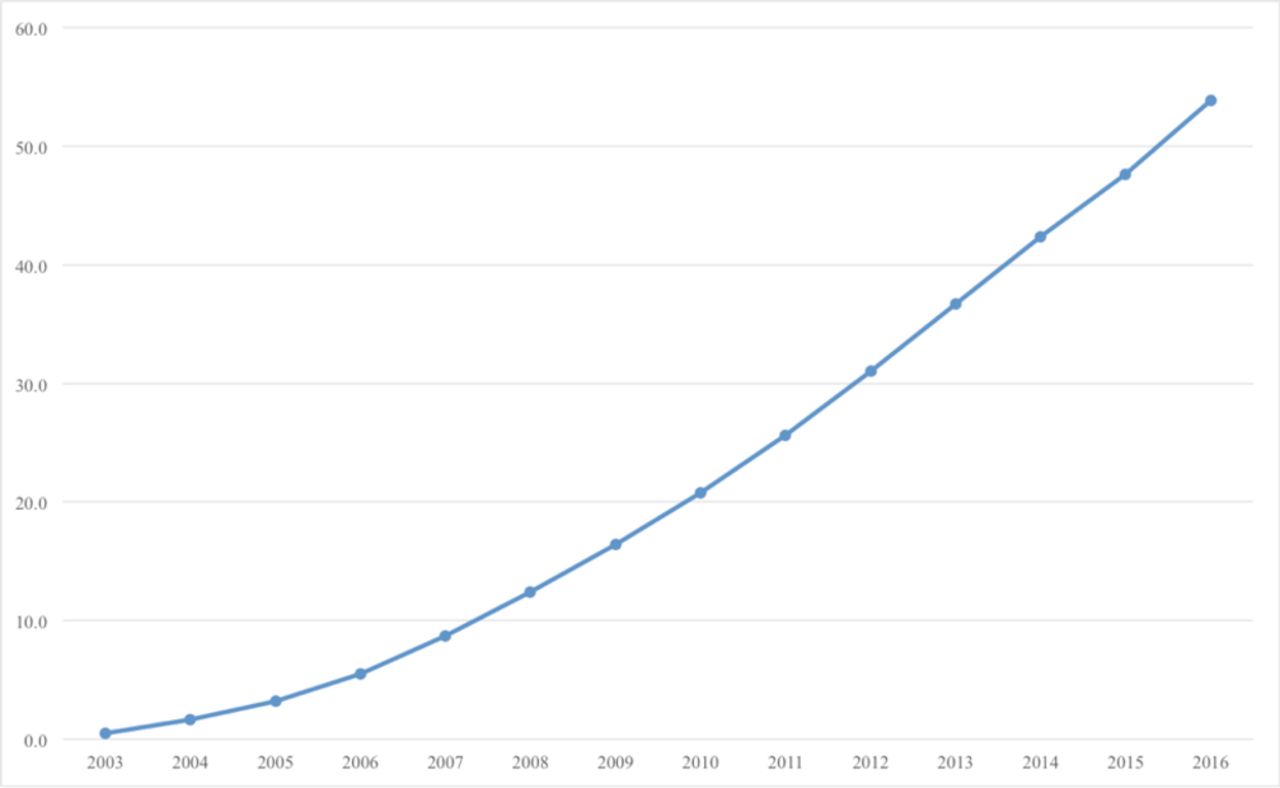
These figures shed some light on why the decline of the female survival advantage slowed after 2008 (figure 2). In fact, while no antiretroviral therapy was available before the year 2003 in sub-Saharan Africa, access to this treatment rapidly increased afterwards, especially after 2008. In 2003, less than 0.5% of the individuals living with HIV received the antiretroviral therapy. In 2009, this percentage rose to 16%, and to approximately 54% in 2016 (figure 5). This important increase in the treatment after 2008 substantially reduced the mother-to-child transmission of HIV, largely benefiting girls due to their higher vulnerability to HIV infection.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trends in the coverage of antiretroviral therapy in sub-Saharan Africa, 2003–2016. Note: This figure is based on data provided by US President’s Emergency Plan for AIDS Relief (PEPFAR).
We have provided two distinct explanations for the declining survival advantage of girls in sub-Saharan Africa. Improved political institutions and child exposure to HIV reduced the female survival advantage in this region. However, this decline has been slowed by the scale-up of antiretroviral therapy, which has benefited girls more than boys among HIV-exposed children. Among HIV-unexposed children, boys have continued to gain over girls, which is consistent with the fact that improved political institutions in many countries have had stronger health benefits for the former.
It should also be noted that the male-female gap in neonatal mortality is possibly narrower if one accounts for the fact that the HIV/AIDS epidemic may have altered the investments in infant health and perinatal care made by the parents or health workers. Fortson16 argues that high male adult mortality in the early phase of the epidemic led parents to invest more in female versus male schooling. If parents also disinvested in the survival of boys, then the relative male gain in survival attributable to improved health institutions is underestimated.
This editorial has important implications for health policymakers, practitioners and researchers interested in the causes of sex and gender differences in health outcomes. Excess male mortality at early ages poses a fundamental gender equity problem. In addition, it results in a numerical deficit of male adults that has negative consequences for women on the marriage market, and lowers their bargaining power within the household. The numerical deficit of men also favours a culture of polygamy, which is shown to lead to sexual network configurations that bias the spread of HIV/AIDS against women.17 It follows, therefore, that scientific and institutional improvements that decrease excess male mortality should be encouraged, as it is clear that such improvements will solve the aforementioned gender equity problem, and it will also benefit women. The fact that the positive health benefits of antiretroviral therapy have mostly accrued to girls invites more research on how HIV-related drugs might affect males and females differently. Also, more studies should be conducted to determine if the link between the emergence of HIV and the narrowing of the gender gap in neonatal mortality documented in this editorial is causal. Research in this direction is likely to inspire policies aimed at closing the gender gap in survival, for the greatest benefit to mankind.
Acknowledgments
We are grateful to the editor and two anonymous referees for useful comments that have helped improve the paper. We also thank Wafaie Fawzi, Christopher Sudfeld and numerous seminar participants at the Department of Global Health and Population at Harvard TH Chan School of Public Health for useful discussions and suggestions. Roland Pongou acknowledges the support of the Takemi Program in International Health at Harvard T.H. Chan School of Public Health, Harvard University.
References
Footnotes
Handling editor Seye Abimbola
Contributors This editorial was written by SY, SD, MCM and RP.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data statement No additional data are available.