Article Text

Abstract
Objective: To examine the public’s knowledge and perception of SARS and the extent to which various precautionary measures have been adopted.
Design: Cross sectional survey.
Setting: General population of Hong Kong at the height of the SARS outbreak (29 March to 6 April 2003).
Participants: 1115 ethnic Chinese adults.
Main results: Forty per cent did not recognise fomites as a possible mode of transmission whereas 55.1% believed that the infection could be transmitted airborne. A large proportion (30.1%) believed they were very or somewhat likely to contract SARS while only one quarter believed they were very likely to survive if they contracted the disease, benchmarked against an actual case fatality ratio of 2.8% at the time of the survey and 15%–20% according to current best estimates. Precautionary measures directed against person to person droplet spread were generally adopted by most while the prevention of transmission through fomites was not practised as frequently. Respondents with higher risk perceptions and a moderate level of anxiety were most likely to take comprehensive precautionary measures against the infection, as were older, female, more educated people as well as those with a positive contact history and SARS-like symptoms.
Conclusions: The findings demonstrate that the promotion of protective personal health practices to interrupt the self sustaining transmission of the SARS virus in the community must take into account background perceptions of risk and anxiety levels of the public at large. Continuing public education about preventive measures should be targeted at the identified groups with low current uptake of precautions.
- SARS
- cross sectional study
- Hong Kong
Statistics from Altmetric.com
The question that has been foremost in the global public consciousness about severe acute respiratory syndrome (SARS), a potentially fatal form of atypical pneumonia first identified in Guangdong in November 2002, is how the epidemic can be curtailed. The worldwide outbreak became apparent in early March 2003 when clusters of cases began to accumulate in Hong Kong, Singapore, Hanoi, Canada, US, UK, and elsewhere.1,2 There has been unprecedented collaboration between local and world health authorities to contain its spread.3 Scientists and clinicians have made impressive progress on characterising the virus responsible for SARS and on achieving good efficacy in treating those who have contracted the disease.1,4
However, what is not known is how the general public views and reacts to many complex issues related to SARS. Previous experience with large outbreaks of serious illnesses has indicated that the potential for panic is often a lot greater than the risk for the disease.5,6 On the other hand, the lack of an appropriate level of anxiety can just as easily bring about public inertia in the adoption of adequate prevention.6,7 Standard data collection and analysis in outbreak control rarely includes information about population psychological responses to the disease and its relevance to the agent, vector, host epidemiological triangle. To aid public health officials and physicians in planning for a possible expansion of the current outbreak in different parts of the world and to gauge public response in their own communities, we conducted a representative, population based survey of Hong Kong residents who are at the centre of the epidemic in southern China to learn their views and beliefs about and psychological responses to SARS.
METHODS
Respondents were recruited using random digit dialling of all land based telephone lines in Hong Kong. A total of 1115 Hong Kong adult residents completed the survey, which was conducted from 29 March to 6 April 2003. The response rate was 76.4% and the sampling error was 3.1 percentage points (fig 1).

SARS epidemic curve and chronology of key events in Hong Kong.
The survey instrument consisted of 60 questions in total, five of which have multiple parts. It was pre-tested for face and content validity, length, and comprehensibility. The questionnaire was administered in Cantonese Chinese, where 95% of the local resident population was ethnic Chinese.
Firstly, respondents were asked about their self perceived general health status, febrile and respiratory symptoms in the past two weeks, and general anxiety levels using the locally validated State-Anxiety Scale of the State Trait Anxiety Inventory (STAI).8 Next, we inquired about the use of health services in the previous two weeks. The third section examined for the presence, intensity, and setting of direct and indirect contacts with diagnosed SARS cases. Fourthly, we evaluated respondents’ risk perception in terms of their self perceived likelihood of contracting SARS and survival if diagnosed with the disease. Respondents were also asked their beliefs about routes of transmission and confidence in physicians’ ability to diagnose the disease. The penultimate section assessed the extent to which various precautionary measures were being adopted and possible changes in lifestyle practices to prevent transmission of the virus. Lastly, sociodemographics of the respondents were recorded.
We determined differences in proportions between baseline demographics in this survey and a general household survey in 2002 (commissioned by the Hong Kong Government Census and Statistics Department) by calculating the effect size, a standard statistical methodology, where a value of 0.1 indicates a small effect size, 0.3 a medium effect size and 0.5 a large effect size.9 To adjust for possible sampling biases due to sociodemographic differences between respondents and non-respondents and to ensure that the sample was representative of the Hong Kong ethnic Chinese population, we weighted the responses on the basis of the latest figures from the Hong Kong Census and Statistics Department for age, sex, and education level. The final dataset included 1018 subjects while the remainder was excluded due to incomplete data on the three key variables for the weighting exercise.
We also sought to identify predictors for greater adoption of the government’s recommended precautionary measures (defined as at least five of the seven specified strategies in figure 2) and health services use (defined as ever attendance of Western or Chinese medical practitioners in any setting during the previous two weeks) using multivariable logistic regression. Potential explanatory variables were anxiety level (STAI mean score), self perceived likelihood of contracting SARS, surviving the illness if infected, the presence of physical symptoms, contact history and sociodemographics. All analyses were conducted using Stata version 8.0. Ethics approval was obtained from the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster, which conformed to the principles embodied in the Declaration of Helsinki.

{kind=link}
{kind=link}
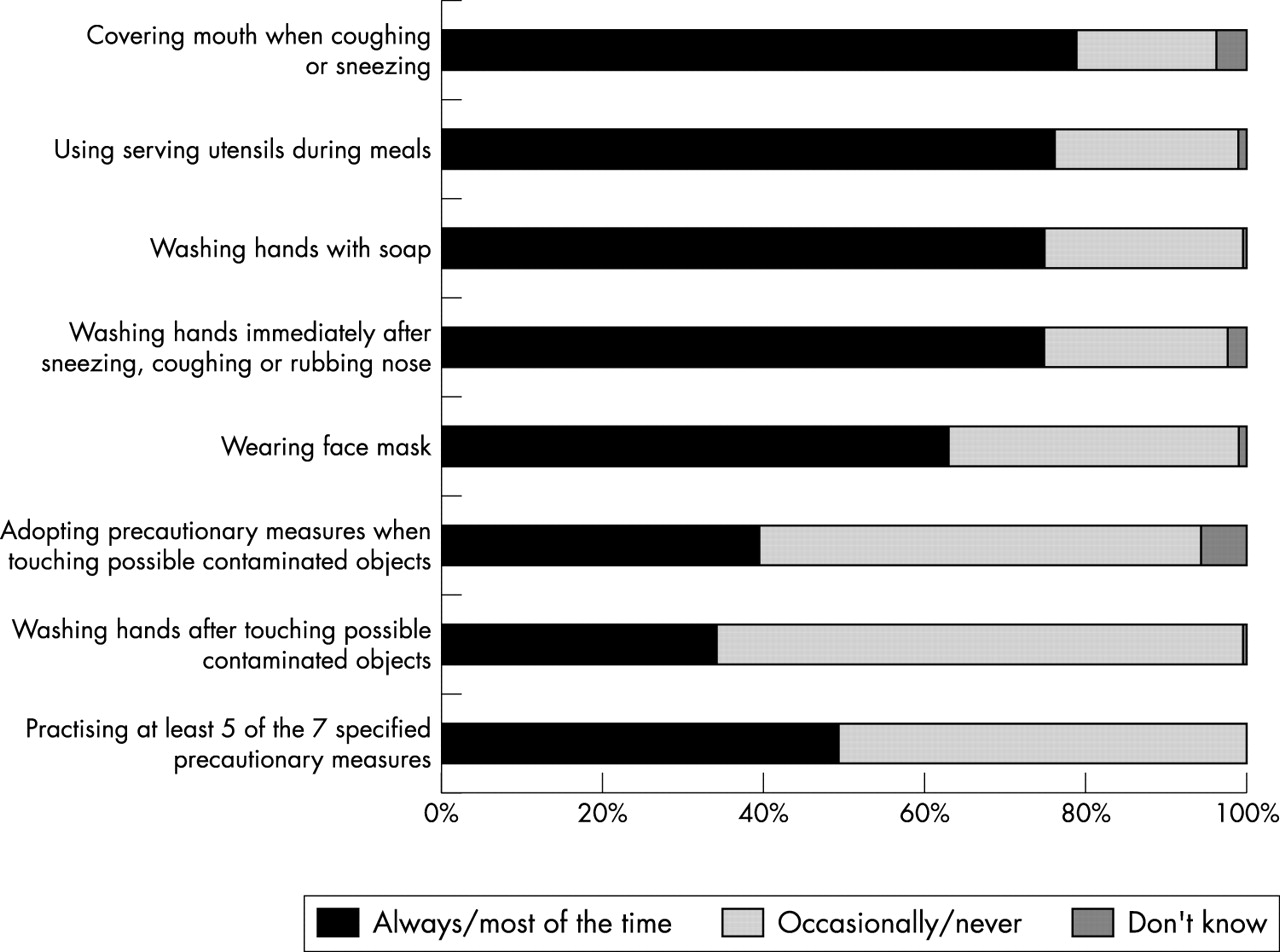
Adoption of precautionary measures to prevent transmission and contracting SARS.
RESULTS
Respondents’ characteristics
Table 1 compares the sample characteristics (in terms of unweighted proportions) with those from the 2002 general household survey. Most of the baseline parameters in this survey were similar to the benchmark statistics, except for educational attainment, which was adjusted for (together with age and gender) in the subsequent weighting exercise.
Respondents’ characteristics
Health and emotional status
Table 2 shows that 1.6% of the sample reported persistent fever of 38°C for at least one day within the previous two weeks, about half of whom (0.9%) also had other respiratory symptoms. This combination of symptomatology would qualify these respondents as possibly “eligible” for an SARS diagnosis (box). Respondents’ anxiety level, measured using the STAI 10-item scale, revealed a sample mean score of 2.24 on a scale of 1 (“not anxious at all”) to 4 (“very anxious”). Although there are no formal normative values for the Hong Kong population, two smaller studies have reported equivalent mean scores of 1.88 in a group of men during the pre-operative period undergoing transurethral resection of the prostate,10 and 2.22 in patients five weeks after stoma surgery for colorectal cancer.11 About one in eight (12.6%) respondents had a mean score of 3 or above indicating that they were either “quite” or “very” anxious.
Symptomatology and anxiety level
Extent of direct and indirect contacts with diagnosed cases
Most (87.3%) respondents reported no contact history, whereas 1.0% had direct contact and 2.7% had indirect contact (“contact of direct contact”) with a confirmed case. The remaining 9.0% of the sample believed they might have been exposed to a possible SARS patient or infected materials (for example, fomites) (table 3).
Extent of direct and indirect contact history
SARS clinical case definition
-
High fever (⩾38°C or 100.5°F)
-
One or more respiratory symptoms (including cough, difficulty breathing, shortness of breath, and hypoxia, etc) OR radiographic findings of either pneumonia or acute respiratory distress syndrome
Knowledge and beliefs about SARS
About four of five respondents knew that SARS was transmitted by person to person droplet nuclei. However, only 62.3% identified that fomites or contact through contaminated objects was also a possible transmission mode. These were the two main routes of transmission confirmed by the Hong Kong Department of Health, US Centers for Disease Control and Prevention and the World Health Organisation. Moreover, more than half of the sample (55.1%) thought that the infection could be transmitted via the airborne route, which does not seem to be the case according to the epidemiological evidence gathered so far (table 4).
Knowledge and beliefs about SARS
Table 4 also shows that about 30% of the respondents believed that they were “very likely” or “somewhat likely” to contract SARS during the current outbreak. This proportion remained the same even after excluding those who reported any contact (direct or indirect) with an SARS case patient. Regarding the likelihood of surviving SARS if they contracted the disease, fewer than 5% believed they were unlikely (4.1% “not very likely” and 0.7% “not likely at all”) to survive but one fifth (20.6%) were uncertain about this. The actual case fatality ratio in Hong Kong as of April 9, 2003 was 2.8% (27 deaths of 970 confirmed cases), whereas current best estimates vary between 15% to 20%.12 Most respondents were confident (23.3% “very confident” and 56.0% “somewhat confident”) that their physician would be able to recognise the symptoms and signs of SARS and properly diagnose the disease.
Precautionary measures
Figure 2 displays the respective proportions of respondents who reported practising each of seven specified precautionary measures as recommended by the Hong Kong Department of Health to prevent the transmission and contracting of SARS, directed against the two main modes of transmission of person to person droplet spread and fomites. Most reported that they would cover their mouths when sneezing or coughing (78.0%) and wash their hands afterwards (74.3%), use soap when washing hands (74.5%), as well as wear a face mask (75.8%). However, only one in three (33.7%) tried to avoid direct contact by touch with possible contaminated objects (that is, fomites) although 65.3% of respondents would wash their hands afterwards. Only a small minority (38.6%) used serving utensils during meals; this is particularly important in Chinese culture where dishes are commonly shared with everyone at the table. Lastly, fewer than half of the respondents (48.7%) practised at least five of the seven specified preventive strategies to improve personal hygiene.
Predictors for the adoption of precautionary measures and health services use
Table 5 demonstrates that respondents who had a moderate level of anxiety were most likely to adopt more precautionary measures against SARS. Risk perception in terms of a higher self perceived likelihood of contracting SARS was also a significant, positive predictor, whereas the likelihood of surviving SARS was not. Respondents who had respiratory or febrile symptoms, especially persistent high fever and cough or difficulty breathing (compatible with a possible SARS diagnosis), were more likely to adopt precautionary measures to a greater extent. Those with a positive contact history (direct, indirect, or suspected) also made greater efforts in practising preventive strategies. Men were much less likely to adopt comprehensive precautionary measures against SARS. There were strong positive dose-response gradients with increasing age and level of educational attainment (p for linear trend were <0.01 and <0.001 respectively). To assess whether anxiety level was an intermediary in moderating the effects of risk perception on the uptake of precautionary measures, we re-analysed the model while omitting the STAI score as an independent variable and found that the OR estimates for the two self perceived likelihood factors did not change appreciably, thus confirming that anxiety was not a significant moderating factor.
Predictors for greater adoption of precautionary measures against SARS and health services use in the previous two weeks
On the other hand, the presence of symptoms was the only robust predictor for higher health services use. Respondents’ health seeking behaviour did not appear to have been influenced by extraneous factors such as risk perception. Anxiety level and contact history yielded marginally significant results.
Policy implications
-
An evidence based approach to public health policy formulation and evaluation during an infectious disease outbreak deserves equal attention to the identification of the responsible agent, pathophysiology, clinical presentation, diagnosis, and treatment of the disease.
-
Population psychological responses in this Chinese community at the epicentre of the SARS outbreak are shown to be an important potential vector for the transmission of an infectious agent.
-
These findings show that the promotion of protective personal health practices must take into account background perceptions of risk and anxiety levels in the community at large.
DISCUSSION
This survey revealed substantial misinformation and false beliefs among a representative sample of Hong Kong adults at an advanced stage of the SARS epidemic, despite heavy and constant mass media and public service announcements coverage (fig 1). More importantly, the findings demonstrate that effective public health action to curb the transmission of the SARS virus, in this case mainly effected through enhanced personal hygiene and health protective measures, is critically dependent on public psychological responses and the prevailing perceptions and beliefs of the community at large. For instance, we found that respondents with higher risk perceptions and a moderate level of anxiety were the most likely to take comprehensive precautionary measures against the infection. One particular strength of the study is that respondents were interviewed during an actual continuing outbreak, compared with other similar studies of infectious disease epidemics or bioterrorism attacks where hypothetical questions were usually posed.
Our findings have several important, immediate implications for public health professionals and physicians in Hong Kong, the Asia-Pacific rim and worldwide. Firstly, our data highlight the central part that public health messages would play in providing appropriate advice and education during this SARS epidemic. The results revealed that there were significant gaps in the public’s knowledge about SARS and associated issues such as route of transmission, risk perception that were strongly associated with deficits in the adoption of precautionary measures to prevent the spread of SARS. Of note, although the majority of respondents knew about preventive strategies against person to person respiratory droplet spread, a substantial proportion did not realise fomites were an equally, if not more important, transmission mode as suggested by accumulating epidemiological evidence. Associated measures such as adopting precautionary steps when touching possible contaminated objects and washing hands immediately afterwards had comparatively low uptake rates of less than 40%, compared with face mask wearing at 76%. The overall effectiveness of preventive measures is only as good as the weakest link in the entire set of precautionary steps. There are clearly areas where efforts directed towards health education and promotion should be redoubled.
Key points
-
Respondents had numerous misconceptions about the routes of transmission of SARS, over-estimated the likelihood of infection and under-estimated that of survival.
-
Those with higher risk perceptions and a moderate level of anxiety are most likely to take comprehensive precautionary measures against infection.
Secondly, there has been much theoretical consideration of anxiety as either a facilitator or barrier for promoting the optimal adoption of precautionary measures. Empirical findings from this study suggest that a moderate level of anxiety brought about the greatest uptake of preventive measures by respondents, whereas those who were either overanxious or had lower levels of anxiety were less likely to adopt such steps necessary in preventing the spread of the infectious agent. This underlines the importance for public health messages relayed to the community to strike a delicate balance between being overly reassuring or normalising and unnecessarily alarmist in terms of its impact on herd psychology.
As would be anticipated, younger, less educated males, the traditional risk takers, were least likely to adopt appropriate preventive measures in protecting themselves and others against SARS. Perhaps targeting health promotion messages through intermediaries of female significant others (for example, mothers, wives or girlfriends) who are more health conscious and risk averse would be worth exploring in an attempt to raise the level of protective precautions undertaken by this vulnerable subgroup.
Reassuringly, we also noted that only those with symptoms were more likely to seek medical attention and other factors such as risk perception and anxiety level did not significantly influence health services use, indicating there was little detectable panic associated with health seeking behaviour, a phenomenon not uncommonly seen in large outbreaks.
In summary, we have identified knowledge deficits, areas of irrational risk perception, and issues that may require attitudinal adjustment in order to optimise self protection against SARS infection and community spread of the causative agent. Complementary to health promotion campaigns in the mass media, we suggest that specially designed target strategies using social marketing and health communication techniques need to be developed and rigorously evaluated for their effectiveness in reaching vulnerable groups (for example, young males and other “risk taking” individuals) and ultimately in changing behaviour for SARS. International experiences, mostly from the HIV/AIDS literature, indicate that an emphasis on sustained interventions towards changing social norms yield the most effective results.13 There is now a window of opportunity to implement this work before a possible next outbreak in the winter months.
The principal limitation of this rapid survey during the SARS outbreak is that it was administered at a single period in time and the stability of the responses is unknown. However, we are carrying out biweekly follow up of the same respondents to track such possible changes as the epidemic evolves. It would also be desirable to compare the public’s psychological responses in other geographical areas that were similarly affected, such as Singapore, Taiwan, mainland China, Vietnam, and Canada. Such comparative analyses, especially if performed at different stages of the epidemic, would enable policy makers to disentangle generic issues from culture specific concerns and the sharing of best practices that appear to have been important in successfully controlling the outbreak across different communities. In addition, the further exploration of the public’s beliefs and their interplay with folklore, common in the Confucian tradition of East Asia, using qualitative techniques would be a useful adjunct in understanding the population psychological responses as reported here.
During a new epidemic such as the SARS outbreak currently, the focus of research and action in the medical and public health community has often and rightly been on the identification of the responsible agent, pathophysiology, clinical presentation, diagnosis, and treatment of the disease. The policy formulation and implementation of public health control measures deserve equal attention and such recommendations should be grounded in a thorough understanding of the public’s perceptions, beliefs, attitudes, and general psychology. This inquiry demonstrates that the promotion of protective personal health practices must take into account background perceptions of risk and anxiety levels in the community at large. Population psychological responses in this Chinese community at the epicentre of the SARS outbreak are shown to be an important potential vector for the transmission of an infectious agent.
Acknowledgments
We thank all the telephone interviewers for conducting this survey at very short notice and Keith Tin and Marie Chi for expert technical assistance in the preparation of the manuscript. This study was partially funded by the University of Hong Kong SARS Research Fund.
Supplementary materials
. HTML Page - index.htslp
Author Correction
Please note that there is an omission from the Acknowledgements section. The additional acknowledgements are shown here:
Professor Charles D Spielberger and Dr Paul Yung are acknowledged for granting permission to use the original and Chinese version of the State-Trait Anxiety Inventory.
Linked Articles
- In this issue
- Corrections