Article Text

Abstract
Background The public health consequences of the Iraq War (2003–2011) have remained difficult to quantify, mainly due to a scarcity of adequate data. This paper is the first to assess whether and to what extent the war affected neonatal polio immunisation coverage.
Method The study relies on retrospective neonatal polio vaccination histories from the 2000, 2006 and 2011 Iraq Multiple Indicator Cluster Surveys (N=64 141). Pooling these surveys makes it possible to reconstruct yearly trends in immunisation coverage from 1996 to 2010. The impact of the war is identified with a difference-in-difference approach contrasting immunisation trends in the autonomous Kurdish provinces, which remained relatively safe during the war, with trends in the central and southern provinces, where violence and disruption were pervasive.
Results After controlling for individual and household characteristics, year of birth and province of residence, children exposed to the war were found to be 21.5 percentage points (95% CI −0.341 to −0.089) less likely to have received neonatal polio immunisation compared with non-exposed children.
Conclusions The decline in neonatal polio immunisation coverage is part of a broader war-induced deterioration of routine maternal and newborn health services. Postwar strategies to promote institutional deliveries and ensure adequate vaccine availability in primary health facilities could increase dramatically the percentage of newborns immunised.
- Child Health
- Immunization
- Access to HLTH Care
Statistics from Altmetric.com
Introduction
The sustained effort of the Global Polio Eradication Initiative has kept Iraq polio-free since 2000. Yet, according to the WHO, Iraq and currently also neighbouring Syria are at high risk of poliovirus outbreak.1 It is well known that the 2003–2011 Iraq War undermined the country's already strained healthcare capacity and disrupted the delivery of basic health services, including routine immunisation.2 However, the public health consequences of the war have remained difficult to quantify, mainly due to a scarcity of adequate data.
This paper assesses whether and to what extent the war affected neonatal polio immunisation coverage. The neonatal dose of oral polio vaccine (OPV) is particularly important for multiple reasons. A recent systematic review has confirmed its protective role for newborns in high-risk countries, where early inducement of polio immunity is imperative. Since most newborns have maternally derived antibody against poliovirus, a neonatal dose of OPV is associated with the lowest risk of serious adverse events, such as vaccine-associated paralytic polio. The priming effect of the neonatal dose can also increase the efficacy of subsequent doses administered later in childhood.3
This study relies on retrospective neonatal polio vaccination histories from the 2000, 2006 and 2011 Iraq Multiple Indicator Cluster Surveys (I-MICS). The impact of the war is identified using a quasi-experimental research design. Specifically, a difference-in-difference approach is adopted to contrast neonatal polio immunisation trends from 1996 to 2010 in the autonomous Kurdish provinces of Iraq, which remained relatively safe during the 2003–2011 Iraq War, with trends in the central and southern provinces, where violence and disruption were pervasive. The research contributes to the assessment of the public health legacies of war, with important implications for the design of postwar maternal and newborn healthcare strategies.
Polio immunisation services in Iraq
The Iraqi healthcare system was developed throughout the 1970s and 1980s and used to be one of the most advanced in the Middle East.4 The system was fully government-subsidised with revenues from the nationalised oil industry and consisted of well-equipped healthcare facilities and adequate number of health service personnel.5 During the 1980–1988 war against Iran, the Iraqi government adopted a set of policies to promote population growth, including a comprehensive child survival programme. As part of this programme, routine polio immunisation was made mandatory in 1985, and coverage increased considerably during the late 1980s.6 Since then, according to the national immunisation schedule, each child should receive a first dose of OPV within 2 weeks from birth. Subsequent doses should be administrated at 2, 4 and 6 months.
The 1990–1991 Gulf War and the following embargo and economic sanctions took a heavy toll on the country's healthcare capacity. During this period, public health budget was cut by 90%, medical education and training were neglected, and buildings and equipment fell into disrepair.7 Routine immunisation services suffered a serious setback due to shortage of vaccine supply, poor maintenance of the cold chain and general health service deterioration.8–10 The consequent decline in immunisation coverage led to a resurgence of vaccine-preventable diseases, including polio.6
To provide essential humanitarian needs and medical supplies, the UN Security Council approved the Oil for Food Programme in 1995. The programme was implemented by the Iraqi government in the central and southern provinces, and directly by the UN in the Kurdish provinces, which after the Gulf War had become a de facto autonomous region. From 1995, at least two national polio immunisation campaigns were held every year. As a result, by 2000, immunisation coverage recovered to the pre-1990s levels.4
In the first few months following the 2003 US-led military invasion, basic health services were paralysed by chaos, looting and destruction.11 More than 30% of primary care clinics, 12% of hospitals and 15% of child care clinics were looted or damaged. Four of the seven central warehouses for the storage of drugs and supplies were partially looted. The two main public health laboratories were destroyed, and the Institute of Vaccine and Sera was stripped of equipment and furniture and lost its vaccine supply.7 The Disaster Assistance Response Team, UNICEF and WHO were able to reactivate immunisation campaigns during the second half of 2003, but major constraints remained. These included inadequate vaccine supply, disruption of the cold chain and the adverse security situation that impeded outreach efforts.7 From 2004 through 2007, the public health situation deteriorated further due to escalating insurgent and sectarian violence.12 In addition to the shortage of drugs and equipment, the violence-induced exodus of thousands of doctors and nurses seriously threatened the strained health system.13 ,14 Even more recently, the Iraqi Ministry of Health has continued to face staggering challenges to the provision of basic health services, including routine immunisation, in the central and southern provinces.15–17
By contrast, the status of health system has improved in the autonomous Kurdish provinces. Unlike the rest of the country, these provinces remained relatively safe and experienced no significant increase in the number of violent deaths as a result of the war.18–21 Over the last decade, the Kurdish Ministry of Health has invested significantly in medical personnel and infrastructure. This has led to a widening gap in healthcare capacity between Kurdistan and central and southern Iraq.2
Methodology
Data
The following analysis is based on retrospective neonatal polio immunisation histories from the 2000, 2006 and 2011 I-MICS. The surveys were organised by the Iraqi Central Organisation for Statistics and Information Technology and the Kurdistan Regional Statistics Office, in cooperation with the Ministry of Health and with financial and technical support from UNICEF.22–24
Figure 1 shows the temporal relationship between these surveys and the 2003–2011 Iraq War. The first survey was carried out less than 3 years before the US-led military invasion. A stratified random sampling procedure was adopted. A number of domains were selected within each district according to linear systematic probability proportionate to size. One cluster was drawn from each of the selected domains by simple random sampling, and 10 households were selected within each cluster by systematic random sampling. Fieldwork took place between October and November 2000, and the survey questionnaires were successfully administrated to 99.2% of selected households (N=13 011).22 The second survey was conducted during the phase of most intense insurgent and sectarian violence. The country was divided into 56 domains, and 54 clusters were drawn from each of them with linear systematic probability proportional to size. A linear systematic sample of six households was selected within each cluster to allow the survey team to complete a full cluster in minimal time given the security concerns. Fieldwork in the central and southern provinces began in February 2006 and concluded in March. In the Kurdish provinces, fieldwork lasted from April until June 2006. Household response rate was 98.6% (N=17 873).23 The third survey was conducted during the final phase of the war. Within each district, 31 clusters were selected with linear systematic probability proportional to size, and 10 households were drawn from each cluster by systematic random sampling. Fieldwork was carried out between February and March 2011 in the Kurdish provinces, and between March and May in central and southern Iraq. Questionnaires were administrated to 99.6% of selected households (N=35 701).24

Timeline of war and retrospective neonatal polio immunisation histories. Note: The war began in March 2003, when US-led military forces invaded Iraq, and officially ended in December 2011, when the last US troops left the country. The 2000 Iraq Multiple Indicator Cluster Surveys (I-MICS) was conducted before the beginning of the war and included retrospective information on neonatal polio immunisation for children born between October 1995 and November 2000. The 2006 I-MICS was carried out during the most intense phase of the war and covered children born between February 2001 and June 2006. The 2011 I-MICS was administered during the final phase of the war and collected information for children born between February 2006 and May 2011.
Immunisation histories were collected for all children under 5 years at the time of the surveys using either vaccination cards or mothers’ recall. Table 1 provides details regarding the number of children included in the analysis for Kurdistan, central and southern Iraq by year of birth (N=64 141). The percentages of children whose immunisation histories were obtained from vaccination cards were 50.69 in 2000, 49.79 in 2006 and 60.94 in 2011. If the card was not available, mothers were asked to recall whether or not children had received each of the routine vaccinations, without however specifying when each vaccine was given. Only for the first dose of OPV did mothers were asked to specify whether children were immunised within 2 weeks from birth. Pooling data from the three surveys make it possible to reconstruct trends in neonatal polio immunisation for 15 years, from 1996 to 2010.
Number of children included in the analysis by region of residence and year of birth
Statistical analysis
The impact of war on neonatal polio immunisation is identified using a difference-in-difference approach. A key component of this quasi-experimental identification strategy is the selection of an appropriate counterfactual, which can be used to estimate what would have happened in the absence of war. This is typically done using a before and after comparison for an affected group of individuals relative to a control group.25 ,26
Children born in the Kurdish provinces, which remained relatively safe during the war, are used as a control group and compared with children born in the central and southern provinces, where violence and disruption were pervasive. The identifying assumption is that, in the absence of war, immunisation coverage in central and southern Iraq would have been affected by other time-varying factors in the same way as immunisation in Kurdistan. As shown in the following section, the validity of this ‘common trend’ assumption is supported by the similar immunisation coverage recorded in Kurdistan and the rest of Iraq from the mid-1990s to the beginning of the war.
The following linear probability model is adopted to estimate the effect of war on immunisation, while controlling for potential confounding factors. This allows for a straightforward interpretation of the difference-in-difference coefficient as the average causal effect of war (a binary response model is also fitted as a robustness check).25
 where Yi is a binary outcome variable referring to neonatal polio immunisation status for child i. The variable is coded 1 if the child received a dose of OPV within 2 weeks from birth, and 0 otherwise. Xi is a vector of key individual and household characteristics available in the datasets that may influence immunisation, including child's sex (0=male; 1=female), mother's education (0=no education; 1=primary; 2=secondary or more) and urban status (0=rural; 1=urban). γt are birth cohort fixed effects that are defined by the year in which the child was born (1996–2010). δj are province fixed effects that capture all time-invariant characteristics of the six central and nine southern provinces, as well as the three Kurdish provinces (see figure 2). Wtj is a binary indicator for war exposure, coded 1 if the child was born during the war in an affected province, and 0 otherwise. The associated coefficient ζ estimates the difference in the probability of being immunised between children exposed to the war and non-exposed children. εi is a random, idiosyncratic error term. To account for possible correlations among error terms of children living in the same province, the CIs of regression coefficients are derived from robust SEs clustered at the province level.27
where Yi is a binary outcome variable referring to neonatal polio immunisation status for child i. The variable is coded 1 if the child received a dose of OPV within 2 weeks from birth, and 0 otherwise. Xi is a vector of key individual and household characteristics available in the datasets that may influence immunisation, including child's sex (0=male; 1=female), mother's education (0=no education; 1=primary; 2=secondary or more) and urban status (0=rural; 1=urban). γt are birth cohort fixed effects that are defined by the year in which the child was born (1996–2010). δj are province fixed effects that capture all time-invariant characteristics of the six central and nine southern provinces, as well as the three Kurdish provinces (see figure 2). Wtj is a binary indicator for war exposure, coded 1 if the child was born during the war in an affected province, and 0 otherwise. The associated coefficient ζ estimates the difference in the probability of being immunised between children exposed to the war and non-exposed children. εi is a random, idiosyncratic error term. To account for possible correlations among error terms of children living in the same province, the CIs of regression coefficients are derived from robust SEs clustered at the province level.27
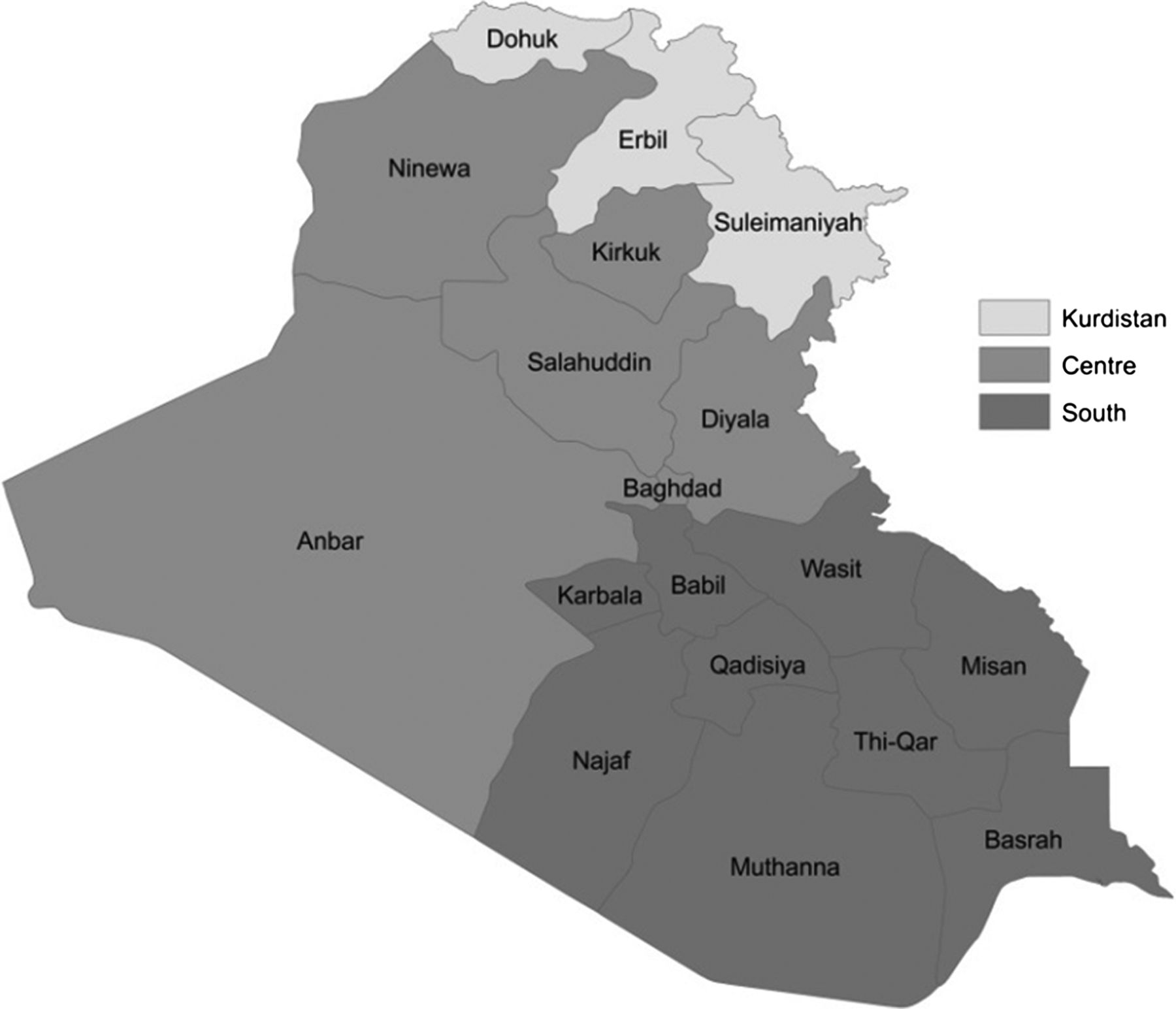
Iraq's 18 provinces and their regional classification. Note: Following the UN classification, Iraq's 18 provinces are grouped into three regions: (1) Iraqi Kurdistan, including the provinces of Dohuk, Erbil and Suleimaniyah; (2) Central Iraq, including the provinces of Anbar, Baghdad, Diyala, Kirkuk, Ninewa and Salahuddin; and (3) Southern Iraq, including the provinces of Babil, Basrah, Karbala, Misan, Muthanna, Najaf, Qadisya, Thi-Qar and Wasit.
Results
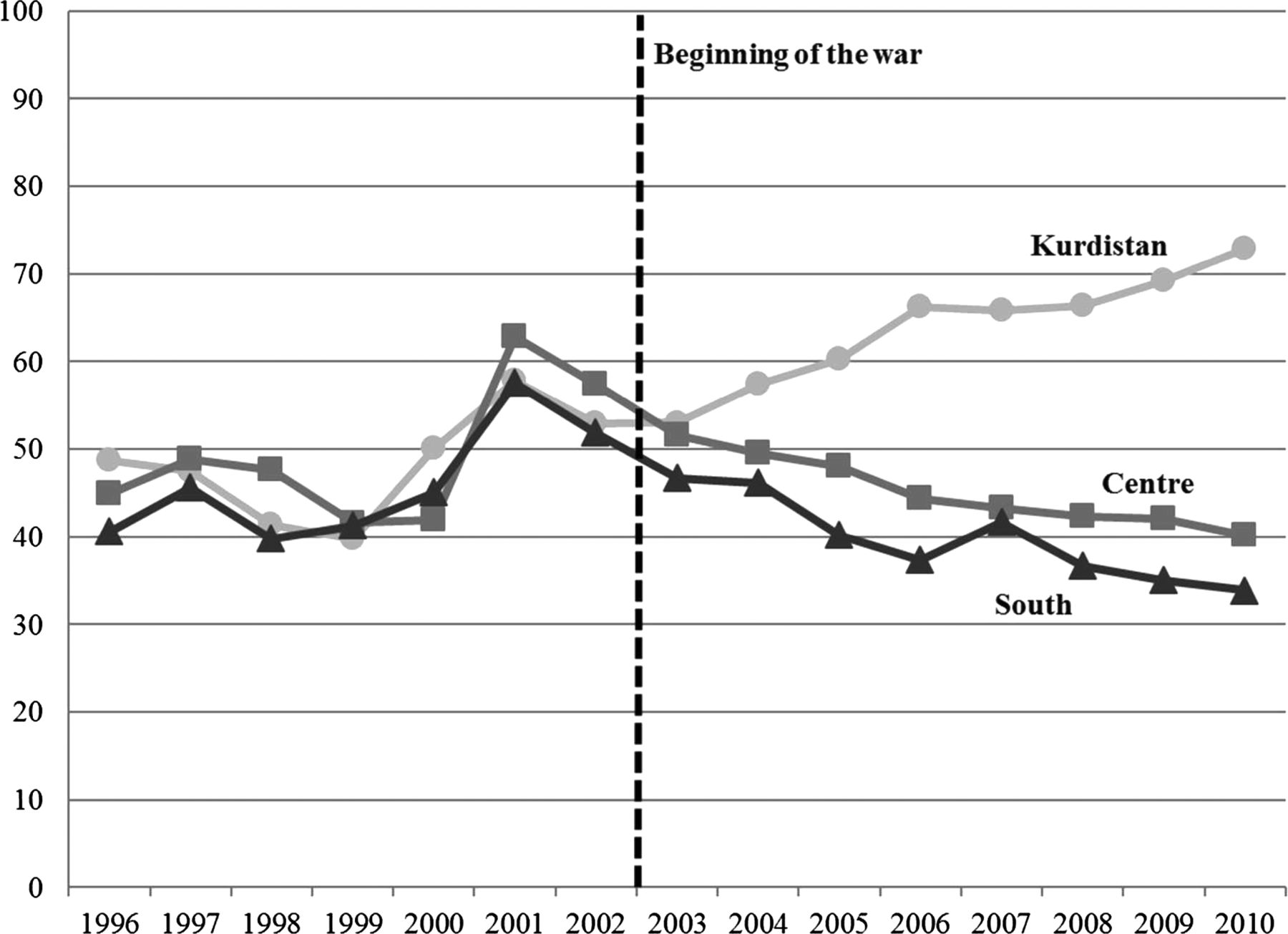
Figure 3 shows changes in neonatal polio immunisation coverage from 1996 to 2010 for Kurdistan, central and southern Iraq. During the prewar period, from 1996 to 2002, immunisation coverage in the three regions followed a common trend. The percentage of children receiving a dose of OPV within two weeks from birth fluctuated between 40 and 50 in the late 1990s. Coverage began to rise in 2000 and reached approximately 60% in 2001. After the 2003 US-led military invasion, the percentage of immunised children continued to rise in Kurdistan, exceeding 70% in 2010. By contrast, in central and southern Iraq, immunisation coverage declined during the war, and in 2010 it was well below the early-2000s level. The diverging trends between Kurdistan and the rest of Iraq for the post-2003 period provide preliminary evidence of the adverse effects of war on immunisation coverage.
{kind=link}
{kind=link}
{kind=link}
Percentage of children receiving a dose of oral polio vaccine within 2 weeks from birth by region and year. Source: Author's calculations using pooled retrospective neonatal polio immunisation histories from 2000, 2006 and 2011 Iraq Multiple Indicator Cluster Surveys.
Table 2 presents estimates from difference-in-difference regressions that quantify the impact of war on the probability of being immunised, while controlling for individual and household characteristics, year of birth and province fixed effects. Coefficients for the linear probability model are reported in the first column. On average, children exposed to the war were 21.5 percentage points (95% CI −0.341 to −0.089) less likely to receive a dose of OPV within 2 weeks from birth compared with non-exposed children. The magnitude of this effect is large, especially if compared with the mean immunisation coverage before the onset of the war.
Probability of receiving a dose of OPV within 2 weeks from birth
As it is generally the case in low-income and middle-income countries, the probability of being immunised varied significantly with household characteristics. Children whose mothers had primary and secondary education were, respectively, 5.6 (95% CI 0.035 to 0.076) and 9.8 percentage points (95% CI 0.069 to 0.126) more likely to be immunised compared with children whose mothers were illiterate. Children residing in urban areas were 5.3 percentage points (95% CI 0.034 to 0.071) more likely to be immunised compared with children in rural areas. Female children were as likely to be immunised as male children (95% CI −0.014 to 0.009). This is consistent with previous research documenting the absence of gender disparities in immunisation coverage across the Arab region.28 Interaction terms between these individual and household characteristics and the war exposure variable were examined, and none was significant.
As a robustness check, average marginal effects for a logistic model are reported in the second column of table 2. The estimated effect of war is virtually the same as that obtained from the linear probability model. Children exposed to the war are estimated to be 20.8 percentage points (95% CI −0.311 to −0.105) less likely to have received a neonatal dose of OPV compared with non-exposed children. The effects of the other covariates also maintain the same magnitude and significance as in the linear probability model.
Discussion
A number of studies have documented insufficient child immunisation coverage in war zones. Robertson et al29 found poor immunisation coverage during the Bosnian War in 1993. The authors could not access any data for the prewar period, but anecdotal reports from public health institutions and primary healthcare physicians suggested that before the war most children were fully immunised. Agadjanian and Prata30 showed that in 1996, during the Angolan Civil War, the country's level of age-adequate immunisation was lower than in most of sub-Saharan Africa. A significant disadvantage of children residing in areas more affected by fighting was also detected. Senessie et al31 collected data in the Greater Freetown area in 1998–1999 during the Sierra Leone Civil War. For most children, immunisation was inadequate for their age and was often delayed during periods of increased hostilities. Mashal et al32 examined changes in immunisation coverage between 2000 and 2003 in Afghanistan. Although progress was observed in all regions of the country, the authors found that the most insecure areas had lower immunisation coverage regardless of the available resources for immunisation services.
Lack of data over longer time periods prevented previous studies from assessing causality and determining to what extent poor immunisation coverage was attributable to war-related disruption or to pre-existing trends. Relying on retrospective neonatal polio vaccination histories from three consecutive surveys, this paper is the first to quantify the effect of the 2003–2011 Iraq War on immunisation trends in Iraq and to provide causal inference regarding the nature of this effect. After dropping dramatically in the aftermath of the Gulf War, neonatal polio immunisation coverage was recovering during the early 2000s. In the autonomous Kurdish provinces, the status of health services continued to improve during the last decade and neonatal polio immunisation coverage increased considerably, exceeding 70% in 2010. By contrast, in central and southern Iraq, coverage declined again during the recent war, and in 2010 less than 40% of children were immunised within 2 weeks from birth. Difference-in-difference regressions demonstrate that children exposed to the war were over 20 percentage points less likely to receive neonatal polio immunisation compared with non-exposed children, even after controlling for individual and household characteristics, year of birth and province of residence.
Using retrospective immunisation histories for the difference-in-difference analysis has a number of limitations. In particular, the effect of war might be somewhat overestimated or underestimated as a result of endogenous migration, fertility and mortality. If, for instance, children from better-off households were more likely to flee the war, the reduction in neonatal polio immunisation coverage would be in part due to a change in the population composition of war-affected provinces. Similarly, the effect of war on immunisation coverage would be overestimated if better-off women were less likely to give birth during the war. However, an opposite source of bias could be due to differences in child mortality. The effect of war would be underestimated if children with no access to basic health services during the war were more likely to die and therefore not to be included in the sample.
This study confirms previous reports documenting that since 2003 pervasive violence and disruption have restricted access to primary health facilities and at the same time reduced the quality of services provided in such facilities.15–17 According to UNICEF, the erosion of basic health services during the war has made emergency polio immunisation campaigns, implemented on a regular basis, the only feasible way to maintain sufficient immunisation coverage and prevent a possible resurgence of the disease.33 The decline in neonatal polio immunisation coverage in central and southern Iraq is therefore part of a broader war-induced deterioration in the country's healthcare capacity. The findings of this study highlight urgent need to enhance the provision of comprehensive maternal and newborn health services. In particular, promoting institutional deliveries and ensuring adequate vaccine availability in primary health facilities could increase dramatically the percentage of newborns immunised.
What is already known on this subject
-
A number of reports suggested that since 2003 pervasive violence and disruption in Iraq have restricted access to primary health facilities and at the same time reduced the quality of services provided in such facilities.
-
However, robust causal inferences regarding the impact of the war on key public health outcomes, such as routine immunisation, had remained lacking.
What this paper adds
-
This study is the first to quantify the effect of the war on neonatal polio immunisation coverage and to provide causal inference regarding the nature of this effect.
-
A difference-in-difference analysis demonstrates that children exposed to the war were over 20 percentage points less likely to be immunised compared with non-exposed ones, even after controlling for potential confounding factors.
Acknowledgments
I thank UNICEF for providing the data. I am very grateful to Stephen Jenkins and Tiziana Leone for their help and advice. I have also benefited from discussions with Berkay Ozcan, Ben Wilson and Paul Bouanchaud. The usual disclaimer applies.
References
Footnotes
-
Funding This study was supported by a UK Economic and Social Research Council Doctoral Studentship.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.