Article Text

Abstract
This guide and glossary focuses on the role of theory and conceptual models within population health research. Upon discussing the critical need for theory in conducting interdisciplinary research, it provides strategies for crafting theories that can be empirically tested and a glossary of theory building terms that are useful for guiding research. In addition to general concepts, the glossary includes some terminology commonly found in the social sciences, whose well established traditions and practices of formal theory building may be particularly informative for epidemiologists and other population health researchers who have minimal formal social science training, but study social factors in their research.
- population health
- theory
- framework
- model
- research design
Statistics from Altmetric.com
Theory is the cornerstone of scientific endeavours. It is the lens through which we conceptualise a research question, propose hypotheses, design a study to test them, discuss the findings, and propose next steps for empirical inquiry. Yet, ironically, it can be one of the more under-appreciated aspects of research; it is very easy for anyone, from a first year graduate student to a senior researcher, to find a wealth of information on research methods, but it is far more challenging to find sources discussing how to develop and use new or existing theories in conducting research.
Within the past decade, the development of population health as a field concerned “with both the definition and measurement of health outcomes and the roles of determinants that impact health” has received increased international attention (p 380).1 Concurrently, the topic of theory conceptualisation in population health—that is, processes and mechanisms, not statistical or methodological issues—has received increased consideration from epidemiology, the social sciences, and public health.2,3,4,5,6,7,8,9,10 Despite this increased focus, it can sometimes be difficult to identify explicit theories used in population health research. The aims of this commentary and glossary are to: (1) emphasise the need for the explicit use of existing or new theories in conducting systematic, interdisciplinary research on population health issues and (2) provide researchers with a set of tools for evaluating existing theories and developing new theoretical approaches that can serve as a foundation for their research. Clearly stated theoretical approaches and the motivations for using them facilitate cross-disciplinary dialogue; ultimately improving our efforts to understand population health determinants and tackle health inequalities. We draw on principles and ideas from a variety of disciplines including epidemiology, sociology, political science, environmental studies, public policy, and public health to present an overview of what constitutes a theory, basic criteria necessary for constructing (and evaluating) a theory, the role of conceptual models within population health research, and a glossary of terms relevant to theory building for guiding research. In keeping with the intended aim of the JECH glossary series, we provide a broad range of concepts that junior researchers, practitioners, and even senior scholars will find useful for designing research and instructing students.11
THE EVER PRESENT NEED FOR THEORY IN STUDYING POPULATION HEALTH
While more research is needed that focuses on the multiple determinants of population health, a solid theoretical basis should underpin this research. Indeed, the theoretical foundations, or lack thereof, in population health research is the subject of a vibrant and ongoing debate.9,10,12 While this manuscript does not speak directly to that debate, it is motivated by the recognition that much research in population health lacks a robust theoretical base.11 In an era where interdisciplinary research is encouraged and embraced, where population health is being studied by researchers in a range of fields as diverse as epidemiology, sociology, political science, environmental science, anthropology, psychology, and medicine, research incorporating any two or more of these perspectives must be conducted with careful attention to theory. Doing so will not only promote effective cross disciplinary communication, but will also provide a more meaningful contribution to our understanding of population health issues. This is particularly the case when researchers incorporate complex and highly debated concepts from the social sciences (for example, social structure,10 social context,9 and social capital13,14). We contend that diligent application of existing theories as well as clear elaboration of new theories can help advance interdisciplinary knowledge and improve population health.*Theory is a necessity.
While theory building and theory testing are often viewed as two separate entities, for this discussion, we consider their inter-play because fields such as population health use theory in an effort to identify problems and design and evaluate solutions. In population health (as well as public health and even medicine), creating theory without testing it has limited utility for action.
EVALUATING A THEORY
Generally, a theory may be defined as logically related propositions that aim to explain and predict a fairly general set of phenomena. Theories allow for a systematisation of knowledge, explanation, and prediction, as well as generating new research hypotheses.15–23 While there are different schools of thought that guide theory development, our approach stems from postpositivism.24,25 Extensive discussion of other approaches (for example, positivism, critical theory) is beyond the scope of this manuscript, but we include other approaches in the glossary.† Below are five closely related criteria that are useful for crafting and evaluating any theory.
-
Logic: The major concepts and relations should be logically coherent.19,21,26 Terms must be clearly defined so that they can be understood by those examining the theory.19,27
-
Causality: The goal of theoretically based research is to identify the systematic components of a set of factors that produce change in the phenomena being studied. Causal drivers and a sense of causal process should be clearly identified.21,26,27
-
Falsification: At least some of the major propositions should be empirically falsifiable.21,28 All useful theories suggest ways in which they may be subjected to empirical assessment.16,19,27 To quote the biologist W A H Rushton, “A theory which cannot be mortally endangered cannot be alive”(p 349).29
-
Scope: Although it can change over time, the scope of the theory should be clear and relatively broad.21 It must be focused on generic processes and not unique characteristics of any specific situation or case.19
-
Productivity: The theory should promote non-obvious implications and produce a relatively large number of predictions per assumption.21,29
CONCEPTUAL FRAMEWORKS, THEORIES, AND MODELS
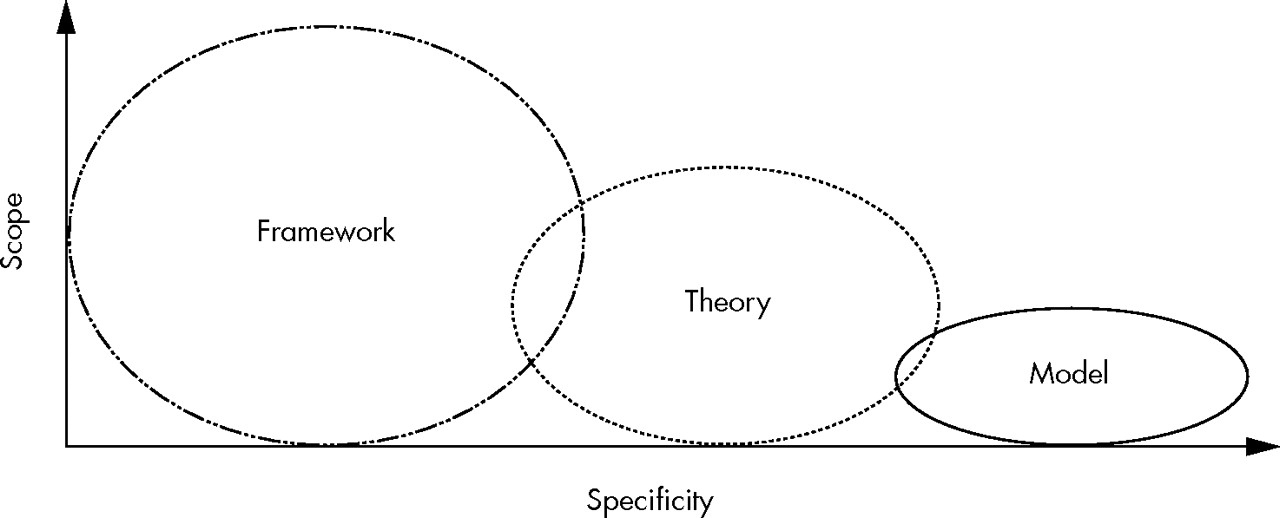
Despite being often conflated and used interchangeably by researchers, the terms “conceptual framework” (or simply “framework”), “theory,” and “model” (sometimes termed “theoretical model” or “conceptual model”) do not mean the same thing. A distinct typology is used in the policy sciences and is equally valuable for other disciplines. Involving more than semantics, these distinctions encompass different levels of abstraction from the broadest level of conceptualisation (framework) to the more focused (model).20,21,30
A conceptual framework identifies a set of variables and the relations among them that are presumed to account for a set of phenomena.20,21,30 It can range in scope from a modest set of variables to even a paradigm,20 which is a broad, overarching intellectual framework or architecture of assumptions used for examining an area of scientific inquiry. While used to organise inquiry and set the stage for theory development, frameworks do not provide explanations for outcomes31 (for example, see Patrick and Wickizer’s32 use of the term for organising ideas related to studying communities and health).
From a conceptual framework, one moves towards a theory, which explicates a more dense and logically coherent set of relationships, including direction, hypotheses, as well as how variables may covary.20,21,27 Nested within a particular framework, a theory makes specific assumptions that are necessary for a researcher “to diagnose a phenomenon, explain its processes, and predict outcomes” (p 40).30 Ideally, researchers use more than one theoretical approach when conducting their research, which allows them to test competing or rival hypotheses.20,27,29,33
Finally, a model is the narrowest in focus of the three. Models are developed and used to make specific assumptions about a limited set of parameters and variables.20,21,30 These assumptions are then systematically explored and tested on a limited set of outcomes by a particular method or methods.30 A model may also draw upon several theories to explore a specific problem in a particular setting.17,34 When presented as a diagram, a conceptual model can provide a useful visual picture of the proposed causal linkages between specific constructs drawn from a theory or theories.34
In summary, a framework, theory, and model can be envisioned as operating along a continuum. The scope decreases as the logical connectedness and specificity increase (see fig 1).20,21,30 Applying this typology to population health research, many of the purely theoretical pieces in population health are not detailing theories at all, but rather fall under the rubric of frameworks. Additionally, most population health theorising presented under the auspices of “models” are technically frameworks. This critique extends beyond semantics; these well established definitions (frameworks, theories, and models) can help to promote explicit and rigorous theoretically driven population health research, which will over time, help us identify and address processes that impact the health of populations.

The continuum of frameworks, theories, and model.
More than a visual aid: the utility of conceptual models
Population health researchers are increasingly using conceptual models to facilitate necessary integration of socioeconomic, political, cultural, psychological, and biological factors into its multidisciplinary research agenda.8,35 This is an important contribution to the field; however, it also highlights the need for theoretically driven research. In particular, we identify two issues that limit the utility of conceptual models that lack a corresponding theoretical approach for practical research purposes.
Firstly, discussion of these models has tended to heavily focus on their heuristic or metaphorical value—that is, their use for visualising and comprehending the multiple levels of influence on individual and population health.8 Provided they are concisely detailed, conceptual models certainly accomplish this task, but such an exclusive focus is a disservice to their powerful utility. Surprisingly, scant explicit attention has been paid to another function of these models: hypothesis formulation. Analogously, imagine if the rocket—another powerful tool for scientific progress—was only used for observing the complexity of earth from miles above and ignored for its potential to explore the moon and conduct experiments.
Secondly, many of the models presented in population health research to date are discussed at such a high level of abstraction that their utility for constructing empirically testable hypotheses is stunted. In a multidisciplinary arena, conceptual models can and should be put to better use. We recognise this is a challenging task, but we also argue that doing so will substantially advance our knowledge of population health.
Despite the pervasiveness of conceptual models in social and behavioural research, one is hard pressed to find any instructional literature that addresses how to develop a conceptual model.34 The language of model building is frequently taught in social science methodology courses; the guidelines for symbols, details, and nomenclature are similar to those found in statistical analysis texts under “causal models” and have been adopted for procedures such as path modelling and structural equation modelling.36–38 Drawing from this literature, we suggest that once a researcher has identified a theory or set of theories that may explain their phenomena of interest, they:
-
Identify important constructs. These are abstract concepts drawn from a theory. Constructs are used to guide the appropriate selection of observed measures or variables. For example, a researcher interested in the influence of poverty on health might operationalise these respective constructs using the measures of income and self rated health.16
-
Detail the causal flow, which typically proceeds from left to right. Variables appearing to the left of the model are assumed to be causally antecedent to the variables appearing on the right.34,36 For most population health models, this generally means that health (however operationalised) appears the furthest to the right.
-
Detail causal relations using arrows. This is generally done using single headed arrows that lead from one variable to another. Double headed arrows are commonly used in models to convey relations that are either reciprocal or correlated.36,38
-
Depending on the complexity of relations being tested, it is an accepted practice to illustrate the direction of hypothesised causal relation by placing + and − signs above the causal arrow to respectively indicate positive and negative relations.36
In summary, a good model does more than just allow the reader to easily comprehend complex relations. It can help researchers identify important causal logic or causal mechanisms, suggest important constructs that will need to be operationalised, and clearly indicate crucial relations or hypotheses that should be empirically tested. Additionally, a well structured model can also facilitate thinking about analytical approaches that may be used to test the relations suggested in the model.27,34,36 Overall, models can be enormously useful when they specify what is at stake in a theory test. However, when they are theory-less and simply mark concepts placed in some logical order (so that researchers may statistically manipulate variables associated with those concepts), they move towards being useless. When this practice becomes excessively complex with many concepts and arrows between them, the models created deserve the appellation “arrow salad.” (Bruce Link, 5 Nov 2004, personal communication)
A population health example of the theory building process
We draw upon a popular framework in population health—namely, that presented by Evans and Stoddart35 in their influential article “Producing Health, Consuming Health Care” to present a brief example of using existing frameworks and theories to develop concise, empirically testable models. These authors outline nine constructs, including social environment, individual response (behavioural and biological), genetic endowment, and health care as health determinants. This framework is far too abstract and comprehensive to be empirically tested; rather, it is meant to facilitate and broaden thinking about multiple determinants of health and wellbeing.35 Such high levels of abstraction suggest that theory, preferably competing theories, are needed to understand how some of these constructs may be causally related. While theories are less comprehensive than the framework from which they were derived, they are more specific and concrete than a framework (recall figure 1). For this example, we focus on a general question: How might the social environment impact health?
We consider three broad constructs in Evans and Stoddart’s framework to explore the pathways between the: (1) social environment; (2) individual response, and (3) health and function, all of which, as the process of research moves forward, will need to be clearly specified. Before this step, however, researchers should identify existing theories, or create new explicit theories, that might help them predict relationships between the social environment and health. For example, a materialist or resource based theory2 would suggest that the quality of a social environment can have a direct, health promoting influence on health behaviours via (among other things) the amount and quality of resources it makes available to individuals. In turn, this may shape individuals’ opportunities to adopt healthy behaviours and consequently enjoy better health than people without such resources. Compared with the more abstract framework, this suggests a denser and more logically coherent set of relations, including direction (that is, social environment → health behaviours → health), hypotheses (that is, health behaviours mediate social environmental influences on health), as well as how variables may covary (that is, better social environments encourage healthier behaviours and, consequently, make individuals healthier).
The final step is to develop a conceptual model that makes specific assumptions about a limited set of variables. If, according to our theory, resources within a given social environment influence individuals’ health behaviours and subsequently impact health, then we should be able to suggest potential social environments with different levels of resources where we could empirically examine these relations. To test this theory, we could explore how different neighbourhood grocery stores and markets (social environments) provide different quality of foods (resources). We could also examine the rates of obesity (our measure of health) among neighbourhood residents. Such an explicit model (displayed in figure 2) offers the opportunity to test a variety of competing hypotheses that might be based on different theories. If dietary practices were not found to mediate the relation between food availability and obesity, then the researcher is forced to consider why this hypothesis was refuted. Setting aside methodological issues that may account for the findings, a researcher might consider how well the constructs were operationalised, as well as exploring whether alternative explanations may be more viable (for example, cultural norms regarding eating habits, lack of income to purchase healthy foods, prices of healthy foods). Ultimately, this may lead to new hypotheses.

{kind=link}
{kind=link}
Example of the connection between a framework, a theory, and a conceptual model.
This example is intentionally simplistic. Theories are often far more elaborate and models may be developed that attempt to simultaneously test two competing theories (for example, Link et al39). Nevertheless, it adequately details the logical flow of theory building from framework to theory to model to hypotheses. Even if researchers began their work with a substantive focus such as exploring “what population-based social factors might account for unhealthy eating and obesity,” the theory and corresponding framework are still important for influencing decisions regarding what constructs to consider, how these construct might be operationalised, the pathways in which they operate, and the explication of hypotheses that can be tested. Without careful attention to theory and building models that are empirically testable, research results can be interpreted in any fashion, full of the influence of biases, proclivities, ideologies, and possibly even ignorance. The theory building process not only helps to keep us honest, it helps us progress.
A GLOSSARY OF THEORY BUILDING TERMS
In concluding this discussion, we leave the reader with a list of general terms and definitions that are connected to the process and activity of theory building. To reiterate, while the above discussion is rooted in the foundations of postpositivism, the glossary also includes terms pertaining to other philosophical approaches.
Abstracted empiricism
Coined by sociologist C Wright Mills,40 refers to the practice of social science research (but is applicable to any research) that over-emphasises methodology at the expense of theory. Mills viewed this practice as the polar opposite of grand theorising (see below). Similarly, sociologist Pierre Bourdieu and his colleagues used the term “hyperempiricism” in such discussions.41
Conceptual model
A tool for theory explication developed and used to make specific assumptions about a limited set of parameters and variables.20,21,30 These assumptions are then systematically explored and tested on a limited set of outcomes by a particular method or methods.30 (Sometimes termed “theoretical model” or “conceptual model”).
Constructivism
A theory building approach that contends that realities are only apprehendable in the form of multiple subjective constructions that are socially and experientially based, local and specific in nature, and dependent on the individuals or groups holding the constructions.24,25 Theory is developed inductively, as the researcher and object of investigation are linked in an interactive manner and findings are literally created as the investigation proceeds.24,25
Critical theory
A theory building approach in which the goal is to use theory to critique the way the social world is organised (and propose alternatives) as well as critique the utility of science for understanding it.18,19 It assumes an apprehendable reality consisting of historically situated structures that are crystallised over time; considers knowledge as value mediated and, thus, value dependent; and relies on a dialogical/dialectical methodology to transform previous constructions, whereby a dialogue between the researcher and the subjects of inquiry creates more informed consciousness.25 Although the term is often used to refer to a variety of theoretical approaches, its origins are rooted in the “Frankfurt School” of social theory, where, beginning in the 1920s, scholars such as Györgi Lukács, Theodor Adorno, Max Horkheimer, Herbert Marcuse, and Jürgen Habermas drew upon Marxist and Hegelian influences to better understand and critique structural conditions in an effort to promote liberation.18,19 Since then, a number of other critical theory approaches have emerged (for example, critical feminist theory, critical race theory, queer theory).
Deductive
Research that starts with a hypothesis and designs a study to systematically test it.16
Ecological
Refers to a theory that focuses on the interaction between an organism and its environment. Two examples include Bronfenbrenner’s42 theoretical work within human development and urban ecological theories developed by University of Chicago sociologists in the early 1900s to understand urban processes.19
Empirical
Refers to logic obtained from observation and/or experimentation.
Endogenous
Refers to variables in a model that receive causal inputs from other variables in the model. Epidemiologists frequently refer to endogenous variables as confounding factors.37 In economics, endogenous implies several things: in economic theory, it refers to a variable whose value is determined “inside” the model itself, and is not imposed as an “outside” assumption, while in econometrics, it refers to a variable correlated with the error term either because of omitted variable bias, simultaneous equations, or measurement error.43
Epistemology
The study of questions regarding the relation between the knower (or would-be knower) and what can be known. Answers to these questions are constrained by answers to ontological questions.25
Exogenous
Refers to variables in a model that do not receive causal inputs from other variables in the model.37
Falsification
The act of where a theory or hypothesis is refuted (or attempted to be refuted) by empirical evidence that stands in contrast to it. From a Popperian standpoint,44 conclusions that withstand falsification are treated as plausible until better evidence is found to challenge them (p 15).37
Framework
A theory building tool that identifies a set of variables and the relations among them that are presumed to account for a set of phenomena.20,21,30
Heuristic
A cognitive “tool” used for facilitating the conceptualisation of abstract, complicated, or complex ideas.
Hypothesis
A provisional conjecture or tentative assumption about the causes or relation between phenomena.45 Hypotheses can be directional (for example, impoverished populations will have higher mortality rates compared with more affluent populations) or non-directional (for example, populations X and Y will differ with respect to all cause mortality). A hypothesis should not be confused with a research question (see below), as the hypothesis serves as an extension of the research question.
Grand theory
A theoretical scheme that attempts to provide an overarching explanation of all phenomena or reality. In sociology, grand theorising is commonly associated with Talcott Parsons’ “structural-functionalist” theory of social structure and human action, which came to dominate the field during the first half of the 1900s, only to be strongly rebuked and abandoned by the 1950s for several reasons, including overly general assertions and lack of empirical testability.18,19 (See “Middle range theory”)
Inductive
Research that proceeds from observation to the development of hypotheses.16
Metaphor
In theory building, a word, concept, or symbol used as a heuristic device to convey and/or comprehend an abstract concept. The classic example of the use of metaphor in epidemiology is “the web of causation.” While touted by some for their utility in conceptualising complex ideas,3 metaphors can also restrict the development of new ideas due to their connotations.41,46,47
Method of multiple hypotheses
Credited to geologist T C Chamberlain,33 a scientific method whereby a researcher proposes two or more competing hypotheses that may be empirically tested. This method attempts to alleviate a researcher’s preference for or attachment to a single hypothesis and ensures that it is put to a rigorous empirical test.
Middle range theory
Popularised by sociologist Robert Merton,48 theories couched at the middle range of abstraction between grand theories and microlevel theories of very specific events/phenomena. Merton argued for these theories in social research as a reaction to grand theories, which, among other reasons, he viewed as lacking the capacity to be empirically tested.
Non-recursive
A model containing feedback loops or reciprocal relations between constructs (see Recursive).
Ontology
The study of questions regarding what is the form and nature of reality and what can be known about it.25
Paradigm
A broad, overarching intellectual framework or architecture of assumptions used for examining an area of scientific inquiry.20
Positivism
A theory building approach that assumes the existence of a “real,” apprehendable reality driven by immutable natural laws and mechanisms and that researchers are capable of studying objects without influencing them or being influenced by them.25 Although encompassing a variety of forms (for example, Comtean positivism, logical positivism, behaviourism), overall, positivism relies on a reductionist view in its search for universal mechanistic rules that are not contextually bounded and seeks to verify hypotheses (compared with falsifying them as in postpositivism).25,49–51
Postpositivism
A theory building approach that attempts to address some critiques of positivism. Reality is assumed to exist, but, in contrast with positivist assumptions, it is only imperfectly and probabilistically apprehendable.25 Although objectivity may not be possible, it remains as a “regulatory ideal” (p 205).25 Research entails making claims and then refining or abandoning some of them (via the use of quantitative and qualitative methods) for more strongly warranted claims.24,25,52 Findings are contextually bound and thus are not generalisable to all cases and situations.49,50 Because evidence is always imperfect and fallible, researchers do not verify a hypothesis (as in positivism), but rather indicate a failure to reject one.24
Recursive
A model containing no feedback loops or reciprocal relations between constructs.
Research question
A general question guiding the present research from which a theory and hypotheses may be developed. Although often used in place of formal hypotheses, research questions are not hypotheses and vice versa.
Tautology
A redundant argument where the conclusion only makes explicit that which is implicit in the premise (or simply restates the premise).18 For example, Putnam’s53 social capital theory (commonly applied to population health research) has been criticised for its tautological reasoning—that social capital leads to positive outcomes (for example, health) and these same positive outcomes are used to infer that a community has adequate social capital at the same time (without considering other possible factors that may be causing the outcomes).54
Theory
Logically related propositions that aim to explain and predict a fairly general set of phenomena. Theories allow for a systematisation of knowledge, explanation, and prediction, as well as generating new research hypotheses.15–23
Acknowledgments
The authors composed this manuscript while completing Robert Wood Johnson Foundation Health and Society Scholar Fellowships in the Department of Population Health Sciences at the University of Wisconsin-Madison. They wish to thank David Kindig, John Mullahy, Stephanie Robert, Elliot Friedman, Michelle Frisco, Kristina Sionean, and Margaret Weden for their encouragement and for contributing to the weekly intensive discussions on population health theory building conducted as part of the UW-Madison Health and Society Scholars Program that inspired and informed this manuscript. Special thanks are extended to Bruce Link, Javier Nieto, and Brian Kelly for their thoughtful reviews and comments and Stephanie Robert, David Vanness, Theresa Hoeft, and Andy Whitford for recommending reference materials that improved aspects of the glossary itself.
REFERENCES
Footnotes
-
↵* While we recognise that page limitations in journals may restrict the extent to which authors choose to detail the theoretical underpinnings of their research, this does not mean that diligent theorising should not have occurred in the conduct of that research. Much of what we are discussing in this glossary involves the use of theory in research, but not necessarily how this theory is conveyed in the finished manuscript. To promote interdisciplinary knowledge, however, we contend that it is important to try to effectively communicate important theoretical approaches that guide research.
-
↵† In the spirit of the JECH glossary and the practice of prior glossary authors, 55 we encourage and invite exchange on this topic, particularly via the use of alternative approaches (for example, positivism, critical theory). In no way should this manuscript be interpreted to imply that postpositivism is the only or best approach to research.
-
Conflicts of interest: none declared.
Linked Articles
- In this issue