Article Text

Statistics from Altmetric.com
Key questions
What is already known?
Cardiovascular disease and diabetes represented 17.4% of the global burden of disease in 2017, however, only 2% of overall development assistance for health was dedicated to combating non-communicable disease (NCD) in that same year.
Prior research suggests that community-based interventions can be both cost saving and associated with improved outcomes among patients with hypertension and diabetes in countries and communities across a broad range of socioeconomic settings.
What are the new findings?
Patients affiliated with HealthRise programmes in Brazil and the USA showed progress in meeting diabetes and hypertension treatment targets and declining blood pressure and haemoglobin A1c since programme enrolment.
In India and South Africa, no detectable differences in blood pressure or A1c levels were observed between patients being served by facilities involved in the HealthRise programme and facilities that were not affiliated with HealthRise.
Existing health systems infrastructure and social determinants of health limit the potential effect of community-based programmes aimed at improving the detection, treatment and care of hypertension and diabetes.
What do the new findings imply?
Continued work is needed to understand which community-based NCD interventions may work best given local contexts and needs.
Health system strengthening, increased financing for NCDs and a locally driven focus on how interventions and community factors together, may contribute to improving health for individuals.
Introduction
Hypertension and diabetes account for increasingly more early death and illness worldwide,1–3 particularly in places where rapid sociodemographic changes have spurred shifts in diet, physical activity and other key risk factors for non-communicable diseases (NCDs). Despite cardiovascular diseases and diabetes resulting in 17.4% of the global disease burden in 2017,2 these conditions and NCDs more broadly remain severely underfunded by national governments and donors alike, with only 2% of overall development assistance for health dedicated to NCDs in 2017.4
Challenges in implementing models of care that address chronic diseases persist in low-income and middle-income countries (LMICs),5–7 where many health systems are not equipped to reliably diagnose and treat NCDs,8–11 and also in high-income countries, where medication affordability and health insurance can be major obstacles to high-quality care.12 13 As a result, sizeable gaps observed along the cascade of care—diagnosing, treating and controlling disease—emphasise the need to better reach patients, retain them in care and promote effective interventions for disease management.5 14–19
Community-based programmes, which bridge communities and health systems and include a range of interventions such as education and outreach, self-management and home-based care, have emerged as a promising approach to filling gaps in access.20–22 Past research suggests community-based interventions focused on hypertension and diabetes detection and case management can be both cost saving and associated with improved outcomes.23–26 Specifically, results from LMICs include lower blood pressure (BP) associated with mobile technology-supported primary healthcare interventions in Indonesia27; decreased BP related to a community health worker (CHW)-led chronic disease programme in rural Uganda28; reduced BP and blood glucose associated with Iran’s rural Behvarz system29; better hypertension control for patients receiving CHW home visits in Gauteng, South Africa30 and higher odds of hypertension or diabetes control related to CHW-led interventions in Chiapas, Mexico.31 Some studies indicate community-based screening for hypertension and diabetes can be effective,32–35 but how well these activities identify undiagnosed or at-risk individuals across underserved communities is less well known.
To strengthen the evidence base for community-based NCD interventions, HealthRise was developed to implement and evaluate pilot programmes aimed to improve screening, diagnosis, management, and control of hypertension and diabetes among underserved communities.36 37 HealthRise was launched in 2014 and pilot programmes were implemented in nine communities in Brazil, India, South Africa and the USA between 2016 and 2018 and were composed of interventions tailored to local needs and contexts. A prospective evaluation of these initiatives at each site sought to assess whether these community-based programmes could increase the proportion of patients meeting treatment targets for diabetes and hypertension compared with usual care. This study presents the main cross-country findings, aiming to provide insights for community-based NCD programmes targeting underserved populations globally.
Methods
Study design
A global evaluation framework was designed prior to intervention implementation at all sites and is presented in online supplementary file 1 and described elsewhere.36 37 Briefly, we used a mixed-methods quasi-experimental approach, drawing from process indicators to assess programme implementation; quantitative data to measure changes over time and/or differences in patient outcomes associated with programme participation and qualitative data to contextualise patients, providers and stakeholders’ experiences with HealthRise. Process and endline evaluation methods and indicators ultimately varied across sites due to data availability, resource constraints and government regulations; however, each location’s study design aligned with the global evaluation framework.
Supplemental material
HealthRise programme
HealthRise involved several partners for each site in Brazil (Teófilo Otoni and Vitória da Conquista), India (Udaipur and Shimla), South Africa (uMgungundlovu and Pixley ka Seme) and the USA (Minnesota’s Rice, Hennepin and Ramsey Counties) to support programme implementation and evaluation. Online supplementary file 2 details the programme organisational structure and additional detail also can be found elsewhere.36 37 Countries were selected by the Medtronic Foundation, the funder of HealthRise, prior to programme implementation and evaluation onset, and pilot sites were determined by a combination of factors (ie, range of underserved populations with existing health service gaps, high NCD burden, interest of government and nongovernmental partners). A summary description of the health system in each of the selected countries is presented in online supplementary file 3. Programme implementation and monitoring duration varied by site, as shown in online supplementary file 4, with India and USA having the longest implementation periods (2016–2018), and Brazil and South Africa having the shortest (2017–2018). The Institute for Health Metrics and Evaluation (IHME) conducted the evaluation, and was not involved in pilot programme design or implementation.
Supplemental material
Supplemental material
Supplemental material
Table 1 summarises each site’s target population, health demands and challenges (as identified by baseline needs assessments conducted by IHME38–41), and programme implementation dates and main interventions; greater detail on each intervention can be found elsewhere.36 Intervention composition and implementation inherently varied by HealthRise site, as they sought to explicitly address gaps and barriers identified through the needs assessments. Across sites, interventions were implemented alongside usual care and services provided previously, and involved healthcare worker training, health education, patient empowerment activities and regular monitoring of programme enrollees. Individual sites often had unique interventions and implementation approaches (eg, interventions focusing on lifestyle modification included building three outdoor public gyms at primary healthcare units in Vitória da Conquista and building a full-service grocery store with an in-house interdisciplinary wellness team in Hennepin County), as well as main locations of implementation. While most sites’ interventions occurred at primary care clinics or units, others extended to secondary care (eg, increased availability of specialised tests in Teófilo Otoni) and the workplace (eg, workplace-based screening in Vitória da Conquista and uMgungundlovu).
Overview of interventions by HealthRise site
Case definitions
The following case definitions were used across all sites: for hypertension, (1) prevalent cases were patients with a reported or documented diagnosis of hypertension based on country-specific guidelines, or those without a previous or current diagnosis but had systolic BP (SBP) ≥140 mm Hg or diastolic BP (DBP) ≥90 mm Hg at the time of data collection; (2) diagnosed cases were patients with a reported or documented diagnosis of hypertension and (3) patients meeting treatment targets were prevalent cases with SBP <140 mm Hg and DBP <90 mm Hg. For diabetes, (1) prevalent cases were patients with a reported or documented diagnosis of diabetes based on country-specific guidelines, or those without a previous diagnosis but had haemoglobin A1c ≥6.5% at the time of data collection; (2) diagnosed cases were patients with a reported or documented diagnosis of diabetes and (3) patients meeting treatment targets were prevalent cases with A1c <8%.
Data collection
All survey instruments were designed by IHME with input from local evaluation partners and translated to the appropriate languages and are available at http://www.healthdata.org/healthrise-evaluation/data-collection-tools
Process indicators (eg, screening, health workers training indicators) and endline quantitative and qualitative data collection varied by programme site, a result of the variability in site-specific programme activities, intervention populations, and existing data infrastructure. In brief, de-identified patient or medical record extractions were available for Brazil and the USA while patient exit surveys were performed at facilities in Shimla and South Africa. Where possible, comparison group data were collected or drawn from available databases on comparable patient populations. Details on site-specific endline data collection processes and sources are available in online supplementary file 5, including descriptions of sampling procedures for exit surveys. Qualitative data consisted of key informant interviews with facility administrators, clinic- and home-based providers, and policymakers as well as focus group discussions with patients, which were facilitated by either IHME (US only) or independent local data collection professionals contracted by IHME (Brazil, India and South Africa). Endline data for Udaipur, India are not currently available due to delays in government approval for data collection. Table 2 summarises data availability and sample sizes by site and data type.
Supplemental material
Endline data availability and patient sample sizes by HealthRise site and for intervention and comparison patients
Endline evaluation analysis
Quantitative data
We used two main outcome indicators for both diabetes and hypertension across sites: (1) the proportion of HealthRise patients (Brazil and USA) or those surveyed at facilities (Shimla and South Africa) meeting defined treatment targets and (2) average change in biometric measures among enrolled patients (Brazil and USA). We limited all analyses to patients who were prevalent cases and had corresponding biometric data.
For Brazil, at least two biometric readings were needed: one at HealthRise enrolment (baseline) and the most recent measure by endline. We ran paired-sample t-tests to assess whether statistically significant changes in hypertension and diabetes measures—per cent meeting treatment targets and average biometric readings—occurred for HealthRise patients from baseline to endline readings.
For the USA, where we had biometric readings at baseline and endline for HealthRise patients and for comparison groups at each site, we conducted difference-in-difference analyses to quantify the potential effect of intervention exposure. We first ran an unadjusted model, only including binary variables for HealthRise status and timing (ie, baseline or endline) and then an interaction term for HealthRise at endline to capture the effect of HealthRise over time. We also considered an adjusted model, including the following covariates to account for potential systematic differences in US HealthRise and comparison patients: sex (female, male); age (<50 years, 50 years or older); time elapsed from baseline to endline (<12 months, 12 months or more) and comorbidities at baseline (prevalent case of only hypertension or diabetes, prevalent case of both hypertension and diabetes).
In Shimla and both sites in South Africa, we used the average of up to three SBP and DBP measures taken as overall BP status for each patient. Patients also reported treatment status, ever and current (ie, taken medication for hypertension or diabetes as prescribed by a healthcare provider in the last 2 weeks), allowing us to assess cascades of care from diagnosis to meeting treatment targets among prevalent cases. We ran Welch’s t-tests (ie, assuming unequal variance between groups) to evaluate whether statistically detectable differences were observed between patients presenting at facilities in implementation and comparison areas.
Qualitative data
Key informant interviews and focus group discussions were audio recorded, and as necessary, translated and transcribed in English. Each transcription was read (or audio file was listened to) multiple times by a single researcher who assessed open-ended questionnaire responses using thematic analysis.42 Themes were identified at the semantic level. Data were entered into excel templates for analysis with a focus on data patterns associated with overarching research questions. Data codes were collated to generate themes by site. Qualitative data analysis presented in this study is limited to common themes across intervention sites only.
Patient and public involvement
Patients were not involved in the design or the development of the HealthRise evaluation.
Results
Across Brazil, India and South Africa sites, 59 342 people without a previous hypertension diagnosis and 56 642 individuals not previously diagnosed with diabetes were screened at public screening events, home visits or at health clinics through HealthRise programmes (table 3). The majority of screenings were conducted in India (78.8% for hypertension and 69.7% for diabetes). Of those screened for hypertension, 6439 surpassed diagnostic thresholds for elevated BP and were referred to health facilities for diagnostic confirmation, of which 1464 were newly diagnosed with hypertension. Of those with no previous diabetes, 2563 exceeded diagnostic thresholds for elevated blood glucose and were referred for further testing, resulting in 295 new diabetes diagnoses.
HealthRise screening and diagnosis outputs for programme sites in Brazil, India and South Africa
Across all nine sites, 3637 local healthcare professionals were trained on diabetes and hypertension-related topics through HealthRise programmes: 979 in Brazil, 1847 in India, 778 in South Africa and 33 in the USA. CHWs comprised 60.7% of all healthcare professionals trained. A summarised country-specific flow chart of HealthRise participants and additional process evaluation indicators, by site, are in online supplementary file 6.
Supplemental material
Endline quantitative findings
Differences or changes in hypertension and diabetes metrics varied across sites. In Brazil and the USA, where patient-level changes since programme enrolment could be tracked, HealthRise patients generally saw progress in reducing biometric measures and meeting treatment targets. In Vitória da Conquista, more patients met treatment targets for hypertension (45.9% (43.0%–48.9%)) and diabetes (61.8% (49.4%–72.7%)) at endline than at baseline (35.4% (32.6%–38.6%), p<0.001; and 36.8% (26.0%–49.1%), p<0.001, respectively), and patients showed declines for SBP (ie, an average decrease of 4.2 mm Hg (3.1–5.2); p<0.001) and A1c (ie, an average reduction of 0.9 (0.5–1.4); p<0.001) since programme enrolment. Teófilo Otoni HealthRise patients also recorded reductions in SBP (ie, an average decrease of 1.9 mm Hg (0.7–3.1); p<0.01) and A1c (ie, an average decline of 0.6 for A1c (0.4–0.9); p<0.001), with more patients meeting hypertension treatment targets at endline (52.2% (49.3–55%)) compared with baseline (48.3% (45.5–51.2%); p<0.05). For diabetes, more patients met treatment targets at endline (59.7% (52.3–67.0%)) than at baseline [49.4% (42.0–56.9%); p<0.01). Detailed changes in hypertension and diabetes metrics in both Brazilian sites are presented in online supplementary file 7.
Supplemental material
In the USA, unadjusted difference-in-difference model results (figure 1; all model results are included in online supplementary file 8) show that HealthRise programme participation was associated with reductions in SBP compared with comparison patients in Ramsey (14.4 mm Hg decline (2.3–26.4); p<0.05) and Rice (8.4 mm Hg decrease (1.6–15.2); p<0.05) counties. In only Hennepin County, HealthRise participation was associated with an increase in the percent of hypertension patients meeting treatment targets (24.3% point increase (6.8–41.8); p<0.01) relative to comparison patients. For patients with diabetes, HealthRise participation was associated with declines in A1c relative to comparison groups in Hennepin (0.7 decrease in A1c (0.1–1.3); p<0.05) and Ramsey (1.4 decrease in A1c (0.5–2.4); p<0.01) counties. The percentage of HealthRise patients with diabetes meeting treatment targets increased compared with comparison patients in Hennepin (21.7% point rise (6.5–36.9; p<0.01) and in Ramsey county (19.1% point increase ([0.2–38.1; p<0.05) but not among patients in Rice county. Unadjusted model results corresponded with adjusted results across outcome measures in all sites except for change in patients meeting treatment targets for diabetes in Ramsey county (19.1% point increase (0.0–38.0; p=0.05)).
Supplemental material

Differences among US HealthRise and comparison patients from baseline to endline for systolic blood pressure (A), percentage of hypertension patients meeting disease treatment targets (B), haemoglobin A1c (C) and percentage of diabetes patients meeting disease treatment targets (D). Included us patients are limited to prevalent cases of hypertension or diabetes at baseline with at least two biometric measures. Treatment targets were <140 mm Hg SBP and <90 mm Hg DBP for hypertension, and <8% A1c for diabetes. The effect of HealthRise was quantified with a difference-in-difference analysis; the effect of HealthRise by endline is reported for each site, with statistical significance denoted by *P<0.05, **P<0.01. DBP, diastolic blood pressure; SBP, systolic blood pressure.
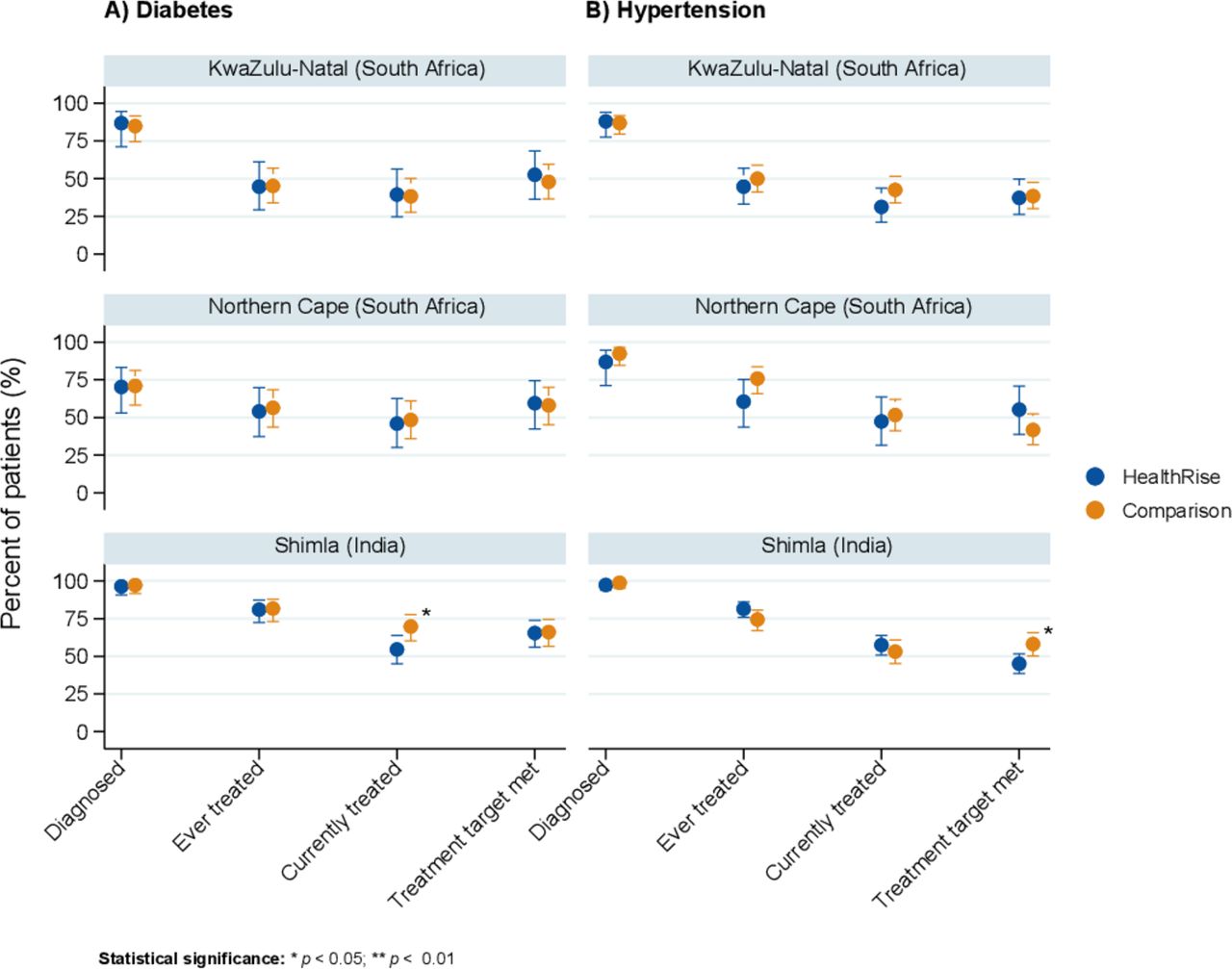
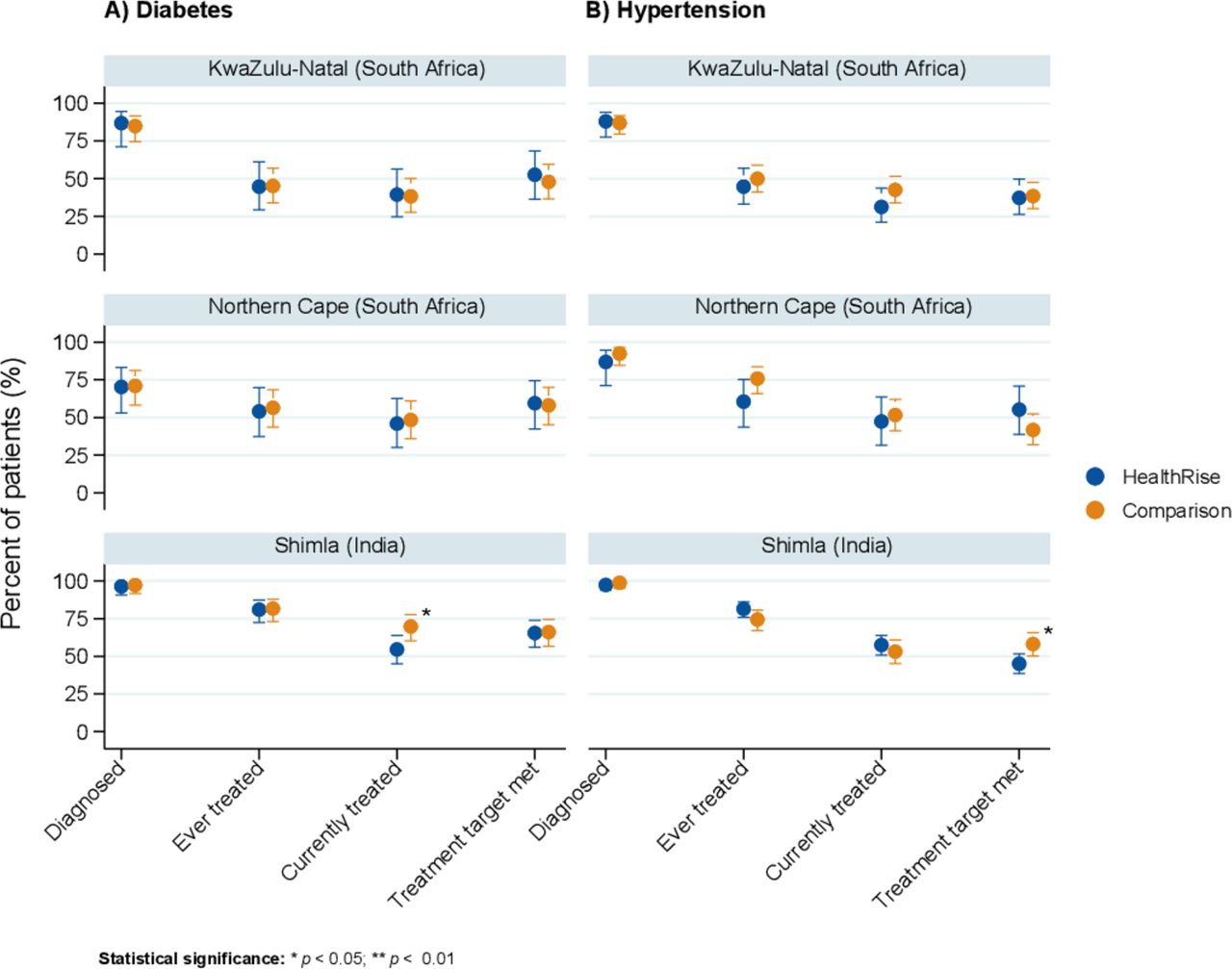
For Shimla, India and South African sites, endline analyses focused on differences between patients presenting at facilities in HealthRise implementation and comparison areas (figure 2). In Shimla, patients with hypertension and diabetes at facilities in HealthRise areas generally did not differ from patients in comparison areas in terms of the cascade of care metrics; exceptions were meeting treatment targets for hypertension and percent currently on treatment for diabetes, where the patients in the comparison areas showed higher rates than patients in HealthRise facilities. In Pixley ka Seme and uMgungundlovu, patients attending facilities in HealthRise areas did not differ from those in comparison areas along hypertension and diabetes cascades of care.
{kind=link}
{kind=link}
Cascade of care for diabetes (A) and hypertension (B) based on patient interviews at facilities located in HealthRise implementation and comparison areas in Shimla, India and in South Africa sites. Included patients are limited to prevalent cases of hypertension or diabetes with biometric measures corresponding with prevalent conditions. Treatment targets were <140 mm Hg SBP and <90 mm Hg DBP for hypertension, and <8% A1c for diabetes. Statistical significance was determined by Welch's t-test, and is denoted by *P<0.05 and **P<0.01. DBP, diastolic blood pressure; SBP, systolic blood pressure.
Endline qualitative findings
Qualitative analysis identified key themes relevant across sites (table 4). First, respondents expressed positive views of the overarching intervention model—an international programme focused on community-based interventions for NCDs—and opportunities to test new services or structures at their sites. In Brazil, providers specifically identified reorganising patient flows and health unit routines as supportive of more structured care delivery. New training opportunities, intensified group activities for patients, increased availability of some specialised tests, and using tablets to aid in patient record-keeping and care decisions were also viewed as positive developments. In the USA, enabling clinical staff to work with in-home providers for the first time was viewed as beneficial for patient care.
Summary of key themes and sample quotes from qualitative data collected across all HealthRise sites
Second, social determinants of health contributing to the risk, onset and management of hypertension and diabetes were consistently reported as substantial challenges. Barriers to healthcare and better health outcomes, including poverty, low levels of health education and limited access to affordable and nutritious food were reported across all sites.
Third, local front-line health workers such as CHWs, ASHAs and community caregivers were viewed by patients and health facility staff and administrators as vital to programmes, as they supported patients facing substantive linguistic, cultural and geographic barriers. For instance, in Shimla, clinic-based providers found CHWs valuable in providing counselling services beyond what is possible within the time constraints of typical clinical appointments.
Care coordination (ie, linkages between different types of providers; homes, communities and clinics; and myriad information systems) also was viewed as critical for supporting more efficient and effective care. Overall, integrated care was viewed positively by participants; however, substantive challenges also emerged, many of which were related to incorporating in-home providers in care teams in the USA. For example, some clinical providers showed initial scepticism about the added value of in-home providers, and most administrators did not have prior experience managing CHWs and community paramedics. In Brazil, interviewees often indicated preferences for health professionals beyond doctors and nurses to be more involved in their care.
Some patients and providers also reported improved patient empowerment through knowledge gained about NCDs and greater confidence in managing these conditions. Further, as highlighted by CHWs in Shimla, providers also learnt more about NCDs and disease management practices. In Brazil, health providers requested more regular opportunities for in-person training, particularly in-depth technical trainings on measuring blood glucose and BP during home visits.
Finally, interviewees across sites stressed the importance of strong health systems, particularly since interventions relied on the availability of necessary staff, facility capacities and services. For instance, in Brazil, Shimla and South Africa, patients and providers identified several long-standing challenges related to core health system functions, particularly adequate medication supplies, sufficient staffing and reliable referral processes. Many of these challenges were outside the scope of HealthRise intervention; nonetheless, they played a role in how interviewees viewed the implementation strengths and issues of the programme.
Discussion
The prospective evaluation of the multisite, global HealthRise programme, a community-based programme seeking to improve hypertension and diabetes care among underserved populations, demonstrates the complexity of assessing community-based interventions across diverse settings and variable data environments. The programme’s implementation and evaluation faced many challenges, including some associated with establishing and maintaining monitoring efforts, particularly within pre-existing systems in underserved communities. Yet, process evaluation findings indicate that more than 56 000 and 59 000 individuals were screened for diabetes and hypertension, respectively, in Brazil, India and South Africa; however, a much smaller proportion of patients received new diagnoses and were referred to care, highlighting potential limitations of large-scale screening programmes. While Brazil and most US sites showed patient-level progress, with increasingly more hypertension and patients meeting disease control targets since programme enrolment and substantial declines in patients’ A1c and SBP decreased since baseline, improved disease management was not detected among patients in HealthRise implementation areas compared with those in comparison areas in Shimla and South Africa. A relatively short implementation period in some sites, alongside the inherent tension between demonstrating impact within time constraints and properly capturing the often slower or complex changes of health behaviours and systems, may underlie these findings. Limited data availability on intervention adherence and fidelity precludes further assessments of the programmes’ implementation quality and its impact on endline findings in each site.
Qualitative data highlighted some positive views of integrating home-based health workers in NCD care to bridge geographical, linguistic and cultural divides, and the importance of effective care coordination across provider types, data platforms and between facilities and communities. Nonetheless, long-standing gaps in system infrastructure likely contributed to continued challenges with care provision and social determinants of health continued to play roles in patient abilities’ to access treatment and manage their conditions. In combination, these findings demonstrate the potential for community based, and particularly, CHW led, interventions to improve NCD outcomes, but also underscore how their reach and effectiveness can be hindered by broader health system, infrastructure and policy constraints. Irrespective of their increasingly vital role for underserved populations, community-based programmes cannot fully remedy inadequate prioritisation or investments in strong, well-coordinated primary care and NCD services.
Successes and challenges for HealthRise and broader community-based NCD interventions
HealthRise programmes referred thousands of screened individuals to care, yet relatively few new diagnoses occurred. Low yields from population-based screening activities are not uncommon,43 44 and these findings support guidelines recommending more selective screening of high-risk groups to improve cost-effectiveness.45 A primary focus on screening may also have contributed minimal community-level effects in India and South Africa. Interventions in Brazil and the USA were more oriented towards improving access to care and medication adherence, which could more quickly affect health outcomes than screening activities, which only initiate the process of bringing patients into care.
In Brazil, both HealthRise sites exhibited notable progress; nevertheless, since comparison patient data were not collected for Brazil sites, we cannot ascribe these patient-level patterns to HealthRise participation. Despite these positive trends, qualitative data indicated poor adherence to medication for both Brazil sites, as well as patient-reported sociocultural tensions around adopting dietary changes and health system-level obstacles to accessing multidisciplinary care and reliably stocked medication at health facilities. In the USA, HealthRise participation was associated with reductions in A1c or SBP and increases in patients meeting treatment targets at some sites relative to comparison patients. Several factors may have contributed to observable impacts at US sites, which had among the longer programme implementation durations and the most robust evaluation, relative to other sites. Interventions in the USA were targeted to address specific barriers to keeping patients in care; the number of patients reached was small, so each person received substantial focus; and the US health system is better organised and equipped to deal with NCDs and therefore did not face the same health system challenges experienced in other HealthRise sites. However, as demonstrated by recent analyses of ‘superutiliser’ patients with medically and socially complex conditions,46 replicating intervention impact to larger populations may be difficult, especially if the resource intensity and patient attention provided through the US HealthRise programmes are not feasible or sustainable. This is particularly relevant given some of the reported difficulties in early-stage programme implementation in the USA, such as recruiting and retaining CHWs and ensuring all providers could access and update electronic medical records.
Additional data and contextual information are needed to better understand why programme impact was not found in India and South Africa. Unlike the Brazil sites, where HealthRise interventions were incorporated into longstanding community-based healthcare structures and CHW-led service provision, India and South Africa HealthRise grantees often had to build systems—both physical and administrative—from the ground-up to support NCD care coordination, medication logistics and community engagement. This challenge, in combination with relatively short implementation periods, and screening being higher programmatic priorities in these sites, may underlie the negligible community-level effects on outcomes. Further, we could not fully account for other local or national initiatives to expand NCD care in both HealthRise and comparison areas; for instance, India launched national guidelines for NCD screening activities through CHWs and community platforms in 2017,47 48 potentially spurring the scale-up of broader community-based NCD programming throughout India after HealthRise began in Shimla. Other studies, including an evaluation of a CHW-managed intervention for patients in India with high cardiovascular disease risk,49 indicate patient-level barriers to care like cost, transport and medication availability could affect intervention impact as well. Substantial drop-offs in care cascades also emphasise the need for locally relevant mechanisms for coordinated care.50 These findings correspond with larger-scale assessments of diabetes care cascades in India and South Africa,14 18 both of which stressed the importance of strengthening NCD case detection and management for more rural, underserved communities.
Additional challenges were highlighted in qualitative analyses. Despite some indication of heightened patient empowerment, as measured by self-reported knowledge and confidence in at least some sites, adherence to recommended dietary and physical activity behaviour changes emerged as a source of tension between patients and providers, highlighting the difficulty of enacting meaningful cognitive and behaviour change amid strong social and environmental influences. Additional challenges that could negatively affect the adoption and scale-up of community-based NCD interventions in resource-constrained settings included the availability and quality of technologies for care coordination; minimal experience managing or working with in-home providers as members of care teams; and challenges in securing long-term funding for community-based NCD programmes, as well as broader health system capacities for NCD care (eg, functional diagnostic equipment, reliable stocking of NCD pharmaceuticals, accessible primary care services). Without greater prioritisation of NCDs in health financing—from government sources to development partners alike—the potential impact of community-based NCD programmes could be hindered by the lack of underlying infrastructure and resources.4 9
Potential implications for community-based NCD interventions
Building off of previous work, the present study offers some programmatic considerations, including facility-level and community priorities, as well as for national agendas on NCD prevention and treatment. In Brazil, India and South Africa, pre-existing health system challenges, ranging from medication stock-outs to long travel times to reach health facilities, posed obstacles to patients and providers. To more effectively treat the rising burden of NCDs, it is critical to address deficiencies in facility infrastructure, transportation, staffing and supplies. In the USA, many providers and administrators had limited previous exposure to home-based providers, which made programme implementation challenging at times, especially during the early stages of intervention. Identifying processes and supportive technologies by which care teams may incorporate home-based care more seamlessly, particularly in terms of sharing patient data and informing facility staff about findings from home visits, is likely to be beneficial. Finally, especially for LMICs, there is an urgent need for development partners to dedicate more funding to NCD care and strengthening health systems more broadly.4 Without a greater emphasis on these health financing areas, many communities in LMICs will remain ill equipped to provide effective NCD care.9
Limitations
Our study’s findings should be interpreted in light of its limitations. First, while HealthRise sites were selected to represent a range of underserved populations worldwide, findings are not generalisable to all underserved communities seeking to improve NCD care. Continued work is needed to understand which community-based NCD interventions may work best given local contexts and needs. Second, despite being incorporated into the initial process evaluation framework, comprehensive information on intervention reach and fidelity (ie, the degree to which interventions were implemented per protocol) were not available across sites and thus could not be included in the present study. To better understand intervention impact, ongoing and future community-based programmes could greatly benefit from ensuring adequate funding, personnel and infrastructure to establish and maintain data collection for evaluation indicator monitoring. Third, in the USA, comparison groups were constructed retrospectively by each grantee, using available patient record information and were not selected by random assignment. While efforts were made to ensure that included comparison patients generally represented individuals who would have been eligible for HealthRise enrolment, they may have differed from individuals who enrolled. Fourth, in Shimla, India and South Africa, we were limited to cross-sectional patient data at endline, and thus could not directly assess potential differences in cascades of care from baseline to endline among HealthRise implementation and comparison areas. Not being able to explicitly account for pre-intervention differences in these areas and how they changed over time may contribute to some findings in Shimla (ie, patients presenting at facilities in comparison areas having somewhat higher levels of current diabetes treatment and meeting treatment targets for hypertension than patients in HealthRise implementation areas). Also, based on our sampling strategy, we cannot rule out cross-contamination in Shimla and South Africa (ie, patients presenting at facilities in comparison areas engaged in HealthRise activities and/or patients in HealthRise implementation areas were not exposed to HealthRise programming). Fifth, the global evaluation team could not verify monitoring data accuracy for sites in India and South Africa, as only aggregated data were provided by grantees due to government regulations governing data use outside the country. Organisations were assigned by the government in each country to check the validity of data before it was transmitted to IHME. Sixth, for Brazil and the USA, we only included patients who remained enrolled at endline in the endline analyses; by taking this ‘as treated’ analytical approach, which provides insights into programme effects closer to full adherence, these patients may not represent all potential target populations for HealthRise interventions and results may be positively biased. Seventh, while results varied by site, the relative lack of differences for several indicators between patient groups and over time could be related to factors beyond programme effectiveness. It is possible that, on average, HealthRise programme implementation and patient duration in the programme was not long enough to detect positive effects; this may be particularly relevant for sites where community-based care and CHW networks had not previously been longstanding models of service provision and therefore required substantial time to establish. Changes in clinical outcomes also can lag behind intervention exposure and thus improvements may not have been fully realised by endline. Eight, information on the existence of preintervention services or programmes were not available across sites; subsequently, it was not possible to ascertain the potential effects of this factor on endline evaluation results.
Conclusion
The global HealthRise programme involved multisite, locally tailored community-based pilot interventions focused on NCD care among underserved populations and incorporated a prospective evaluation by an independent party—all important steps towards strengthening the knowledge base of what works and what does not for improving NCD service delivery at local levels. Across the nine sites in four countries, some progress on patient-level indicators occurred; nonetheless, constraints on both implementation and evaluation periods and variable comparison groups across sites emphasise the need for longer-term evaluations of community-based NCD programmes in the future. Biological, behavioural and sociocultural factors all contribute to the risk for and development of NCDs, requiring multifaceted approaches to optimally support patients and families coping with these complex conditions. Achieving notable impacts on NCDs will not only require broader health system strengthening and increased financing for NCDs, but also a more locally driven focus on how interventions and community factors together contribute to improving health for all individuals.
Acknowledgments
We would like to acknowledge the support and insight of local data collection teams Social Surveys Africa, GfK Mode, IGMC Shimla, Development Solutions, Dinamica Cursos, Tesla Gestao and Press Consultoria and implementation partners Expectra Health Solutions, Project HOPE, Catholic Health Association of India, MAMTA Health Institute for Mother and Child, Pillsbury United Communities, Regions Hospital Foundation, HealthFinders Collaborative Inc, and the HealthRise teams at Universidade Federal dos Vales do Jequitinhonha e Mucuri, Telehealth Network of Minas Gerais, Universidade Federal de Minas Gerais, Universidade Federal de Bahia, Universidade Estadual do Sudoeste da Bahia, Servico Social da Industria, and Associacao de Apoio ao Portador de Diabetes de Vitoria da Conquista who provided the data for this study. Without them, this work would not be possible. We also acknowledge the state and local governments in HealthRise areas for their cooperation and support with HealthRise intervention and evaluation activities. We thank Kelsey Bannon, Erin Palmisano, and Laura Di Giorgio for assisting in the management and execution of the HealthRise evaluation. We also thank Gopal Chauhan for his sincere efforts to support and strengthen the HealthRise programme in India and Maria de Fátima Marinho and Ceres Almeida for their support which was fundamental to the success and sustainability of the HealthRise programme in Brazil. Last, we thank all individuals who participated in this study.
References
Footnotes
Handling editor Valery Ridde
Contributors LSF, KC, NF and EG contributed to the analysis of the data, produced tables and figures, and wrote the initial draft of the manuscript. LSF, NF and EG finalised the manuscript based on reviewer feedback. LSF, SW, MB, JNC, DVC, KC, HCD, NF, RG, TG, KPH, CRM, VM, MN, BP, MBR, GR, BT, AW and EG developed survey instruments, collected data, verified and managed data, contributed to analyses or some combination of the aforementioned contributions. EG conceptualised and managed the evaluation. PB, NC, JD and MTUB provided guidance on the HealthRise project as a whole. AB, CCh, CCi, HCN, MLC, VEK, PE, MALB, JMa, CM, MSM, SMa, DSdM, SMi, JMu, JAQO, MGO, VP, TR, ALR, DR, GS, DAS, TT, HT and SV developed, managed or implemented HealthRise intervention activities or data monitoring systems, or some combination of the aforementioned activities. VC and TPN managed data collection activities. All authors read and approved the final manuscript.
Funding Funding for the HealthRise project came from the Medtronic Foundation. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. JAQO received doctoral scholarship from CNPq/CAPES/IATS, Brazil. ALR was supported in part by CNPq (grant 310679/2016–8), and Instituto de Avaliação de Tecnologia em Saúde - IATS, grant 465518/2014–1) and by FAPEMIG (Programa Pesquisador Mineiro, PPM-00 428–17).
Competing interests PB, NC, JD and MTUB are employees of the Medtronic Foundation. AB, CCh, CCi, MLC, VEK, PE, MALB, JMa, CM, MSM, SMa, DSdM, SMi, JMu, HCN, JAQO, MGO, VP, TR, ALR, DR, GS, DAS, TT, HT and SV are recipients of HealthRise grants from the Medtronic Foundation to implement HealthRise interventions. LSF, SW, MB, JNC, DVC, KC, HCD, NF, RG, TG, KPH, CRM, VM, MN, BP, MBR, GR, BT, AW, VC, TPN, and EG are recipients of funding from grants from the Medtronic Foundation to evaluate HealthRise interventions.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Ethical approval for this study was obtained from the institutional review board of the University of Washington, as well as the local data collection agencies and government entities for each site. This research conforms to the principles embodied in the Declaration of Helsinki. All personal identifiers were removed prior to the data being sent to IHME for analysis; only de-identified data were analysed.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. The datasets generated and/or analysed during the current study are available, when possible, in the GHDx data repository, http://ghdx.healthdata.org/series/healthrise-evaluation