Article Text

Abstract
MomConnect is a national initiative coordinated by the South African National Department of Health that sends text-based mobile phone messages free of charge to pregnant women who voluntarily register at any public healthcare facility in South Africa. We describe the system design and architecture of the MomConnect technical platform, planned as a nationally scalable and extensible initiative. It uses a health information exchange that can connect any standards-compliant electronic front-end application to any standards-compliant electronic back-end database. The implementation of the MomConnect technical platform, in turn, is a national reference application for electronic interoperability in line with the South African National Health Normative Standards Framework. The use of open content and messaging standards enables the architecture to include any application adhering to the selected standards. Its national implementation at scale demonstrates both the use of this technology and a key objective of global health information systems, which is to achieve implementation scale. The system’s limited clinical information, initially, allowed the architecture to focus on the base standards and profiles for interoperability in a resource-constrained environment with limited connectivity and infrastructural capacity. Maintenance of the system requires mobilisation of national resources. Future work aims to use the standard interfaces to include data from additional applications as well as to extend and interface the framework with other public health information systems in South Africa. The development of this platform has also shown the benefits of interoperability at both an organisational and technical level in South Africa.
- Child Health
- Health Systems
- Maternal Health
- Public Health
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known?
Digital health solutions, particularly mobile health applications, are often developed and implemented as pilot projects that lack extensibility, interoperability and integration with the public health system resulting in them failing to reach scale.
What are the new findings?
We have shown that it is possible to optimise the architecture of a mobile health project and rapidly implement a robust system which is compliant with the South African interoperability framework which is extensible, scalable and inclusive of other partners.
What do the new findings imply?
The design of public health information systems needs to follow an open architecture that has been endorsed by the responsible government department(s) and follows best practices on interoperability, extensibility and scalability in order to be sustainable.
Policies such as the South African Health Normative Standards Framework are imperative in implementing compliance to standards and interoperability between different components of the national health information system.
Robust national health information systems, at scale, can be developed using open source software components implemented, together, in an open architecture and interoperable health information exchange model.
Introduction
South Africa is a middle-income country with an inherited public healthcare system that has historically inequitable levels of investment in primary health services.1 In 2014, the Minister of Health, Dr Aaron Motsoaledi, initiated MomConnect to improve maternal and child health and accelerate progress towards the Millennium Development Goals (MDGs) in South Africa.2 When MomConnect was introduced, maternal, new-born and child health mortality had decreased significantly over the previous decade,3 4 but the rates remained unacceptably high and required additional efforts to decrease at the required rate to achieve the then MDGs5 and subsequent Sustainable Development Goals (SDGs).6 Electronic data collection and mobile health (mHealth) interventions provide opportunities for improving health service delivery.2
MomConnect is a national initiative of the South African National Department of Health (NDoH) that sends free mobile phone text messages in all eleven official languages to pregnant women who voluntarily register at any public healthcare facility in South Africa. The objectives include registering pregnancies in the public sector, sending targeted, stage-based health promotion messages and providing mechanisms for interactive feedback on service.
In 2014, key drivers of the initial programme included using the mobile phone infrastructure in South Africa, using open source systems for the technical platform for MomConnect and using local capacity to build and maintain the system and to keep system costs as low as possible. As of 3 September 2017, there were 1 770 988 unique mobile phone numbers registered on MomConnect.
The NDoH published the country’s first eHealth Strategy in 2012,7 the mHealth strategy in 20158 and the National Health Normative Standards Framework for Interoperability in eHealth in South Africa (HNSF) in 2014,9 providing a framework supporting the development of interoperable systems and adoption of messaging and data standards.10
In this paper, we present the design, development and implementation of the MomConnect technical platform as well as technical considerations for mobile messaging solutions in low-resource settings. Interoperability is highlighted as a key feature of the technical infrastructure to achieve scale and get data into the system, using open-source tools.i Last, we discuss learnings for strengthening health services.
Technical considerations in resource-constrained environments
mHealth is an important means of strengthening health service delivery.11 Although there is widespread access to mobile phones in South Africa,12 connectivity and handset costs are a particular barrier to access for the socioeconomically disadvantaged. Poorer, mainly rural communities remain less likely to have access to either mobile phones or more sophisticated phones with data-enabled capacity (eg, able to access the internet or download data-based applications such as WhatsApp). MomConnect was designed to ensure that anyone with a mobile phone, no matter the type, could use the service.10 The logical architecture of MomConnect (figure 1) was designed to accommodate this and also implement the tiered architecture and health information exchange (HIE) detailed in the HNSF13 and the MomConnect process and information flows (figure 2).
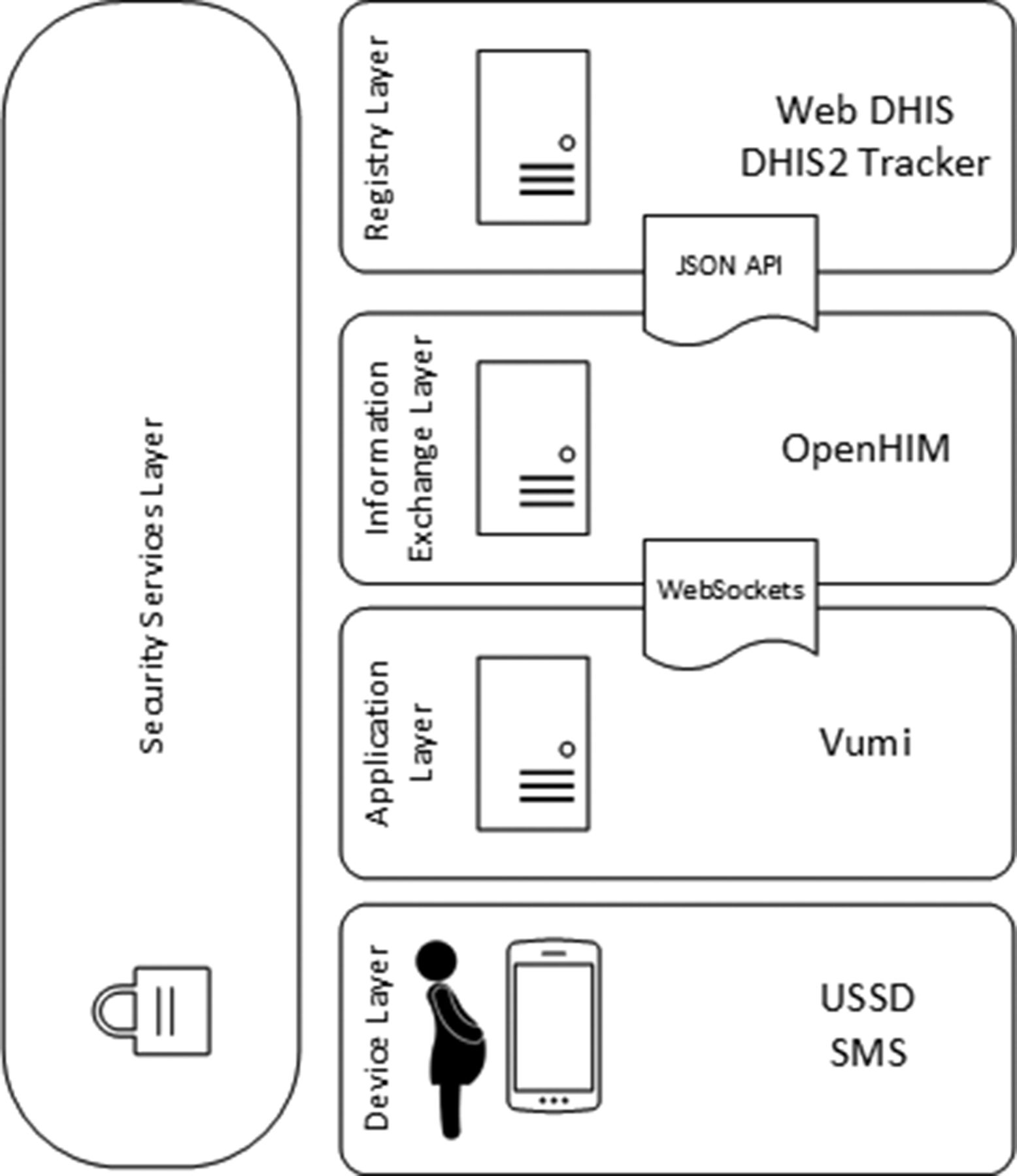
Technical architecture of the MomConnect platform. Key: DHIS2 (District Health Information System, version 2 (https://www.dhis2.org/), and Tracker application (https://www.dhis2.org/individual-data-records)); JSON API (Javascript Object Notation Application Programming Interface); OpenHIM (Open Health Information Mediator (http://openhim.org/)); SMS (short message service); USSD (Unstructured Supplementary Service Data); Vumi (https://www.praekelt.org/vumi-intro/).
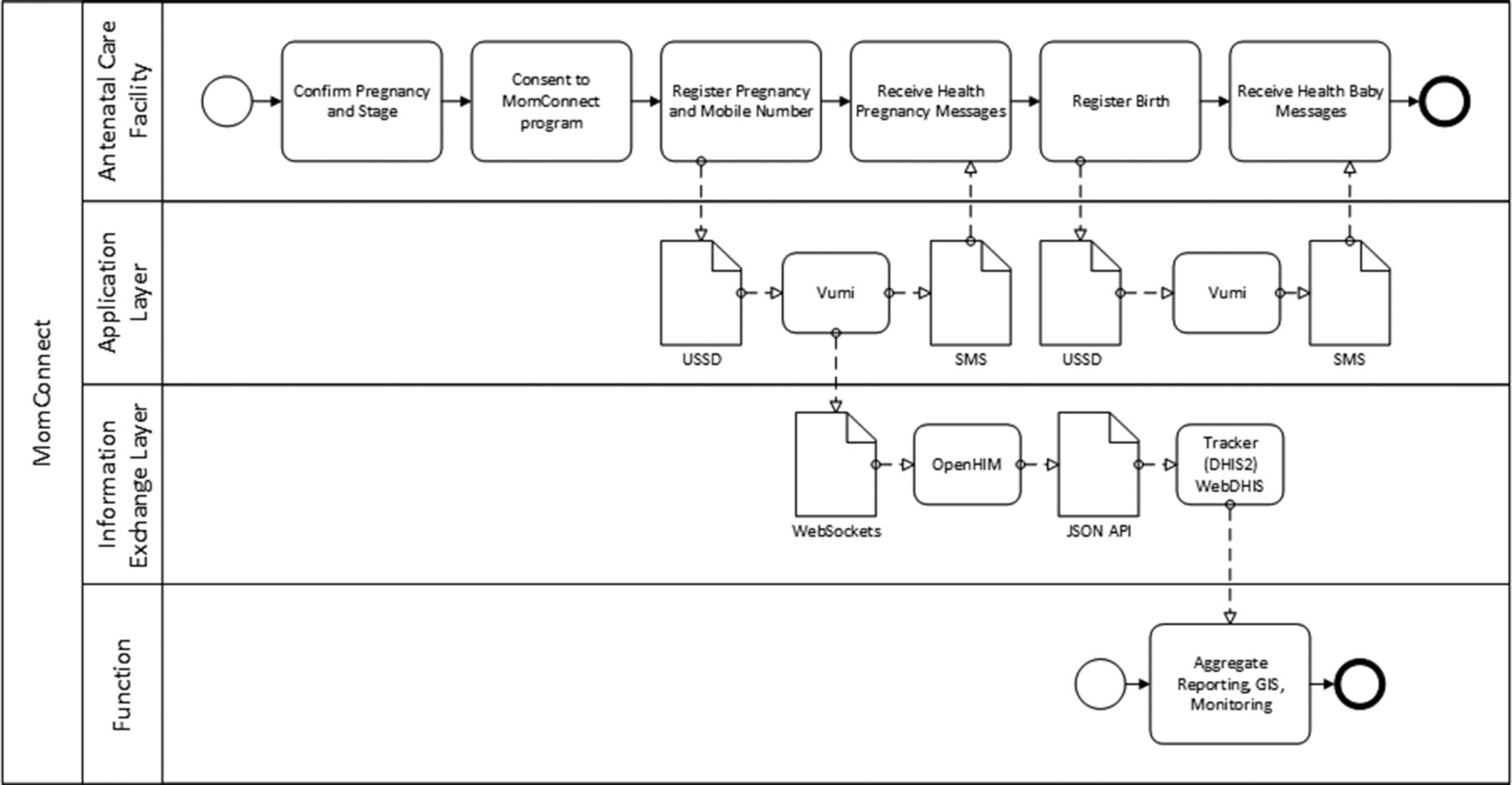
MomConnect process and information flows. DHIS2, District Health Information System, version 2; JSON API, Javascript Object Notation Application Programming Interface; OpenHIM, Open Health Information Mediator; SMS, short message service; USSD, Unstructured Supplementary Service Data.
The benefits of digital health interventions to address health service delivery in low-resource environments are usually limited by a lack of interoperability, data integration and data availability.14 The data generated by such interventions mostly remain isolated to facilities or vertical services as applications are usually designed and developed in the absence of a national architecture and interoperability guidelines. A key objective of national health information systems is to ensure that data are included in the public health system.
Implementation of an interoperability framework, such as the HNSF, is potentially a game-changing step forward in addressing this problem by guiding systems designers to develop applications that can operate according to defined and agreed standards and profiles and integrate data into public health information systems.
Low-income and middle-income countries often have access to donor-funded technical capacity in building mobile health services, but then face longer-term maintenance and support problems.15 The MomConnect technical platform planned to use existing knowledge and local expertise to strengthen sustainability.
Building out the technical infrastructure
MomConnect supports two specific use cases. Clinic registration entails confirmation of a pregnancy by a healthcare worker in a registered health facility followed by registration to receive messages. Public subscription is an open process that allows registration by anyone to receive a limited set of messages.
The District Health Information System, version 2 (DHIS2)16 was selected as the warehouse for MomConnect data and the DHIS2 Tracker application was used as the registry for pregnancy data. DHIS2 also serves as the facility registry and enables the inclusion of a facility code and differentiation of MomConnect clinic registration data from public subscription data. The Open Health Information Mediator (OpenHIM)ii 17 was selected as the interoperability layer for the HIE and Vumiiii (upgraded to Seed) to host the Unstructured Supplementary Service Data (USSD) application and to schedule the sending of stage-based messages to enrolled mothers based on estimated delivery date.
The Patient Identifier Cross-Reference/Patient Demographic Query standards profile of Integrating the Healthcare Enterprise was initially considered for demographic data and the Mobile Health Document profile for clinic data, with a Clinical Document Architecture (Health Level Seven (HL7)) document for clinical data. However, a custom Javascript Object Notation (JSON) message was developed as there was no existing messaging profile catering for client enrolment and notification as well as HL7 Fast Health Interoperability Resourcesiv (FHIR) messages for specific clinical messaging, such as referral requests and clinical encounters.
The USSD clinic registration process for MomConnect has five mandatory fields for the pregnant woman: (1) mobile phone number; (2) estimated delivery date; (3) date of birth; (4) the msisdnv of the device being used to register the mother which can be different from the mother’s mobile number and is automatically populated via the USSD service and (5) chosen language to receive the text messages (all 11 national languages are available). The South African National ID number (alternatively, a passport number) is captured optionally, as the time taken to input the official 13 digits increased USSD time-outs and could pose a potential barrier to accessing the service. Instead, the mobile number given by the woman during registration on MomConnect is used as a proxy system identifier for the purposes of sending and receiving messages. The implication is to focus the service on provision of health information rather than on the development of a data repository. Mobile numbers can be shared or changed and will be insufficient to support a demographic database or a longitudinal health record in the long term.
Getting data into the system
Universally available mobile services, including USSD, a simple text-based system and short message service (SMS) text messages were chosen for registration and information dissemination, rather than data driven applications. Both services are supported by all networks and devices in South Africa. By August 2017, around 3 years after inception of the programme, more than 100 million text messages have been sent to mothers.
The NDOH and MomConnect Task Team also decided to implement an SMS-help deskvi to help answer pregnancy and maternal health-related questions that MomConnect users have as well as to send compliments and complaints. Snappy Helpdeskvii was initially used as the helpdesk software, but was replaced by an open source platform (CaseProviii), originally developed by the United Nations Children’s Fund (Unicef) and adapted by Praekelt.org for use in MomConnect. The helpdesk is hosted within the NDoH building in Pretoria and is staffed by a team of trained nurses who reply to questions submitted by mothers via SMS. Responses are also sent via SMS and the question-response pairs are submitted to DHIS2 for reporting purposes.
The MomConnect information exchange was built to enable the transfer of data between consumer applications (Vumi/Seed) and the central national registry (DHIS2 Tracker). It consists of a number of components. The OpenHIM interoperability layer provides routing, security, transaction logging and auditing services and a framework to integrate other microservices, called mediators, into a coherent architecture. Four node.js microservices are implemented: The Validation Mediator ensures that messages sent into the exchange have valid structures and acceptable data values. The Queuing Mediator accepts validated messages and adds them to a file-based queue which balances load and allows destination systems such as DHIS2 to be taken down for maintenance without affecting the operation of MomConnect. The Caching Mediator provides an in-memory cache for lookup values, also ensuring that the system can operate when central data registries such as the Facility Registry are unavailable due to maintenance. The Tracker Mediator is a generic service that wraps all logic needed to add data to DHIS2 Tracker, including logic for message deduplication and multiple calls to the DHIS2 Tracker Application Programming Interface.
Registration data are processed by the main DHIS2 application to generate aggregate data, reports and maps (figure 3). The DHIS2 server is located in a secure web-hosting environment as part of the national DHIS2 infrastructure.

{kind=link}
{kind=link}
{kind=link}
Example of a map of MomConnect registrations generated from aggregated data by the DHIS2 MomConnect instance.
Care was taken to ensure the security and integrity of the system. All servers run the Ubuntu 14.04 operating system and are firewalled using Uncomplicated Firewall so that they may only communicate with each other, with the exception of the demilitarised zone server which accepts HTTPS requests to an Nginx server. Nginx then load-balances these requests to a cluster of redundant OpenHIM servers ensuring that maintenance and upgrades can be carried out with no interruption to the operation of MomConnect. Any interruption in data from connectivity or service outages is catered for by the system ability to cache data and restart information flows from the relevant point. The OpenHIM uses a 3-node MongoDB cluster, an inherently scalable document database.
Ongoing system maintenance
Once the MomConnect platform stabilised in early 2015, daily maintenance has been minimal without little or no human intervention for significant periods of time.
Contributors to the costs of an electronic data-based system include where the data are stored (or hosted), maintaining services in the system and any associated transaction costs, such as text messaging, USSD and mobile data, as shown in table 1.
Cost breakdown of MomConnect infrastructure, storage and inventory
MomConnect includes measures to alert administrators of any system issues. These include automated email and text alerts from the OpenHIM if any messages flowing through the interoperability layer fail, automated uptime alerting through Pingdom (OpenHIM) and Monitor.us (DHIS2) and alerts for issues in the messaging platform through sentry logs. All components were well tested in staging environments and the infrastructure is able to easily accommodate hundreds of thousands of incoming messages per day and millions of outbound text messages.
Strengthening health services
MomConnect was launched at a clinic in August of 2014 by the Minister of Health, accompanied by a national roadshow in each of the nine provinces. Training was relatively simple given the technology and focused on educating nurses in clinics around how to register patients on the system using USSD. Programme implementation was carefully monitored by comparing registration numbers at individual health facilities with projected antenatal service case load based on historical data.
Since its launch, a number of improvements and extensions have been made to MomConnect. The early success of MomConnect18 led to the development of a complementary service for healthcare workers, especially nurses, providing these services.
The new NurseConnect service was launched in 2016 using the same front-end applications (USSD and SMS) with an interactive mobile website available for compatible devices. NurseConnect uses the same infrastructure as MomConnect. The MomConnect registration in DHIS2 was extended to include nurses and potentially populate a future back-end provider registry for the NDoH.
Since the inception of MomConnect in 2014, technical partners have held ‘connectathons’, encouraging standards-based interoperability with the MomConnect backend by other mHealth application developers and potentially extending the sources of new registrations and subscriptions. The extension of the messaging platform to use HL7 FHIR, allows other mHealth providers to enrol mothers into MomConnect using data-enabled phones to interact with the HIE using this standard. Community health workers can now subscribe mothers using existing mHealth applications.
Discussion and learning points
MomConnect has illustrated the use of mobile technology in reaching pregnant women both in urban and rural settings in South Africa. Despite its limitations, USSD was successful for registration and subscription. Non-reliance on a mobile data service meant that any type of mobile phone could access the service, with a single USSD short code implemented across all four Mobile Network Operators (MNOs) in South Africa. However, the limitations of USSD and its reliance on short, prepopulated answers or drop-down menus require careful flow and data design techniques. Prior to July 2013, USSD was offered by most MNOs in South Africa as a free service, but the commercial costing model introduced since then means that such design issues have substantial impact on costs.
Issues with SMS include the readability of messages by anyone with access to the device, and the limitation of message size to 160 characters (including spaces). Other limitations included the fact that the commercial rates offered by MNOs for text messages are often limited in terms of economy of scale. Although the MomConnect task team was able to negotiate a reduction in rates for all SMS and USSD interactions for the programme with all four MNOs in South Africa, the costs are still substantial. MNOs will also recycle mobile phone numbers not used for a defined period of time, potentially resulting in the broadcasting of messages to mobile numbers not officially registered for the service.
The use of an interoperability layer is invaluable as a way to monitor messages flowing between the consumer facing mobile application and the central data stores and repositories. The ability to inspect messages during development and in the production online system allows system issues to be rapidly identified and fixed.
Future directions
The MomConnect technical platform has a number of successes. The technical architecture is compliant with policies and frameworks published by the NDoH, demonstrating the advantages of national policies and guidelines to harmonise and harness digital health technologies. The technical architecture was designed and implemented relatively quickly and scaled successfully during the project, supporting the national plan to extend the architecture and to include other domains. Using an open architecture and open standards, as required in the HNSF, has proven cost-effective and efficient from a procurement perspective. It is also consistent with international initiatives, such as the Open Health Information Exchangeix (OpenHIE).
The MomConnect technical platform is a reusable framework based on an open architecture, standards and information systems which can be readily replicated in other settings. Open standards facilitate communication between open source software components that can be adopted and reused.
MomConnect shows the potential and limitations of using mHealth to support maternal health promotion messaging in resource constrained environments. The full benefits of MomConnect’s scalable and extensible architecture will depend on the ability of front-end systems to generate appropriate information to populate a demographic repository and longitudinal health record, so as to share with other HNSF compliant public health initiatives such as the Health Patient Registration System.19
Acknowledgments
The authors acknowledge the leadership of the South African Minister of Health who initiated and leads the MomConnect project as well as the direction and contribution of the South African National Department of Health, especially Dr Yogan Pillay who convened and leads the MomConnect Task Team. The mobile phone and mobile health application components were implemented and managed by a group from Praekelt Foundation. The interoperability components were implemented and managed by a group from Jembi Health Systems and the Council for Scientific and Industrial Research (CSIR) Meraka Institute. The registry and data warehouse components were implemented and managed by a group from the Health Information Systems Programme, South Africa (HISP-SA). Additional inputs for the technical design and implementation of MomConnect were provided by ICF International. Regular inputs and feedback were provided by all members of the mobile maternal health Task Team. The support provided by John Snow, Inc. (JSI) in the President’s Emergency Plan for AIDS Relief (PEPFAR) and United States Agency for International Development (USAID)-funded MEASURE Evaluation Strategic Information for South Africa (MEval-SIFSA) project to enable this publication is acknowledged with gratitude.
Footnotes
↵i A secondary aim of this paper is to show the availability of open-source software as part of a component-based information system design for public health in resource-constrained settings. Although the global knowledge base of such software is growing, it remains limited with consequent implications for policy makers and managers who seek to implement such systems.
↵v A number assigned to uniquely identify a subscription in a Global System for Mobile communications (GSM) network.
↵vi As opposed to a traditional voice based call centre which is very expensive to set up, staff and maintain.
Handling editor Seye Abimbola
Contributors CS, PD, DR, VS and TF were part of the team that designed and developed the MomConnect technical platform and maintain it through its ongoing operations. PB led the mobile maternal health task team on behalf of the NDoH from inception and provided critical inputs to the design and development of the technical platform as well as final sign-off. ANP and MB contributed early inputs to the design and development of the system from a technical and public health aspect. All authors contributed to writing and reviewing the manuscript.
Funding MomConnect is supported by a consortium of local and international funders, including the United States President’s Emergency Plan for AIDS Relief (PEPFAR), the United States Agency for International Development (USAID), the Johnson & Johnson Foundation, UNICEF South Africa, ICF International, Elma Philanthropies, Cardno Emerging Markets and Regenstrief Institute. The mobile operators in South Africa—Cell C, MTN, Telkom Mobile and Vodacom—afforded generous discounts on the commercial cost of SMS messages and USSD sessions.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The anonymised, aggregate data set for figure 3 is available from the South African National Department of Health by application to the corresponding author.