Article Text

Statistics from Altmetric.com
Summary box
Civil registration and vital statistics (CRVS) systems are complex adaptive systems involving multiple stakeholders in different government agencies (at a minimum, ministry of health, civil registration authority and national statistics office).
CRVS systems not only generate data, but also offer a gateway to services that people need, such as identity, legal entitlements, access to essential services and social protection.
To date most attempts to strengthen CRVS systems have been ad hoc and reductionist, focused on single components of the system and introducing short-term technical fixes such as assessment, digitization of administrative tasks, advocacy and training.
The potential of new technologies to bring CRVS systems to acceptable levels of coverage and quality can be realised only if structural bottlenecks are dealt with and system-wide actions are taken to ensure scale up and sustainability.
The ‘Ten CRVS Milestones’ framework is designed to help CRVS stakeholders—policy-makers, managers and development partners—better understand how CRVS systems function as a whole, from end-to-end, by describing the key processes that must be accomplished in any CRVS system.
The ‘Ten CRVS Milestones’ framework, used as part of the CRVS assessment and during the design and integration of new interventions, encourages CRVS stakeholders to have a systemic approach to all the essential steps needed for the system to be fully operational.
All countries need timely and complete national vital statistics, the cornerstone for population and socioeconomic policies. For the health sector in particular, reliable data on how many people are born, how many die and why are fundamental to decision-making, health systems planning and resource allocation. Civil registration and vital statistics (CRVS) systems, unlike periodic surveys and other methods to estimate mortality and fertility statistics, provide a continuous, real-time and locally representative flow of information that permits governments to plan and monitor progress in health and social development.1 CRVS systems are not only about data, but are also the gateway to services that people need, such as identity, legal entitlements, access to services and social protection.
There is an urgent need for countries to strengthen CRVS in order to monitor and attain the Sustainable Development Goals (SDGs) and inform efforts to achieve Universal Health Coverage.2 Yet many CRVS systems in low-income and middle-income countries are failing to register all vital events and to produce vital statistics with acceptable levels of completeness and quality, despite introducing technical solutions proven to work well in high-income countries.3 This suggests system failure rather than technical failure. The ‘Ten CRVS Milestones’ framework has been developed to help policy-makers, managers and development partners better understand how CRVS systems function as a whole, from end-to-end, and to unpack complexity by focusing on ten key milestones that must be achieved in any CRVS system.
CRVS systems are complex adaptive systems. They perform hundreds of activities on a daily basis to continuously register the occurrence of vital events, issue certificates, maintain registration archives and produce vital statistics. Although in all settings they share the same objectives, pathways towards achieving them differ, reflecting varied historical, political and administrative conditions. Country CRVS systems are vastly different in terms of governance, accountability to multiple ministries—such as justice, security, local government and health—institutional set-up, organisation, implementation, processes, scale, partners and capacities. Each CRVS system is embedded in a particular national political, economic, social, health and information environment. And each encompasses multiple subsystems that deal with legal identity, civil registries, vital statistics and information technologies.
There is growing country, regional and global interest in CRVS, as exemplified by the SDGs, regional initiatives especially in Africa, Asia and the Pacific and the Global Health Data Collaborative4 (https://www.healthdatacollaborative.org). But to date most attempts to improve CRVS systems have been reductionist, focused on technical fixes and tools, for example, digitisation of administrative tasks or development of CRVS assessment tools. Such ad hoc and disjointed approaches have been tried and found wanting in the past.5 What countries need to accelerate progress is both technical innovations and also systems-wide re-engineering. New technologies have a huge potential to bring CRVS systems to acceptable levels of coverage and quality but they will fail if they cannot be sustained and scaled, if they are not properly integrated in the system and if country decision makers do not face up to the structural changes that their CRVS systems require.
Managing complexity requires that multiple stakeholders work in a coherent way to tackle the challenges in the system. Since 2015, as part of the Bloomberg Data for Health Initiative, Enterprise Architecture process mapping and modelling methodology6 has been applied to national CRVS systems for births and deaths in 16 countries across Africa, Asia, Latin America and Oceania. This has facilitated, for the first time in most settings, collaboration among officials from the ministry of health, the civil registration authority and the national statistics office collectively to identify system process flaws and bottlenecks. With this knowledge, country stakeholders were able to reach consensus on needed actions to ensure that the system tracks the required information from the occurrence of a birth or a death, through its official registration and certification and eventually to its incorporation into the vital statistics system. Developing and analysing CRVS process maps informed structured discussions of the activities and operational procedures that must be carried out for the system to function effectively and deliver on its potential. This led to the concept of Ten CRVS Process Milestones. Each milestone represents the output or product of a number of activities that are logically grouped together and encapsulate a set of requirements that every CRVS system should fulfil.
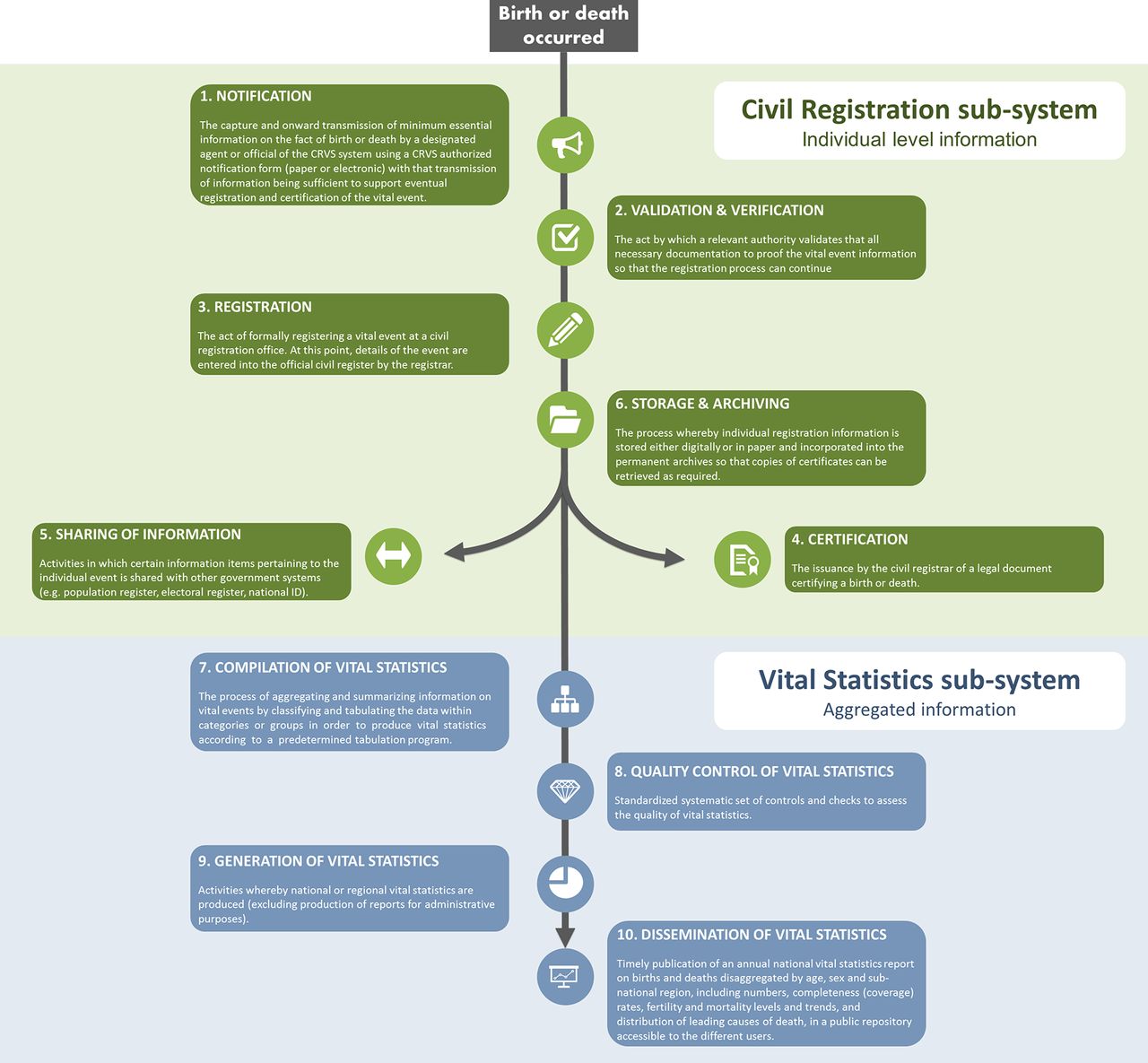
Although some of these steps or outputs of CRVS processes have been defined elsewhere,7 8 there is no international, national, academic or operational document where all of them are described and seen as part of the same set of work flows. We offer here a first attempt to provide a working definition of each CRVS milestone (see definitions in figure 1). The systematic application of this framework exposed hitherto neglected aspects in many CRVS systems such as the importance of the formal notification of vital events, where the health sector could play a crucial role. The Milestones framework offers a simplified sequence of actions needed to ensure that every birth and every death is reported, recorded and compiled to produce vital statistics by age, sex, date and location, thus addressing one of the most pressing information needs in many low resource settings. While the focus in this paper is on births and deaths, the framework can be applied also to other vital events such as marriages, divorces and adoptions.

{kind=link}
‘Ten CRVS Milestones’ framework with a working definition of each milestone. CRVS, civil registration and vital statistics.
This framework, used as part of the CRVS assessment or in the design and integration of new interventions, encourages CRVS stakeholders to have a systemic approach to all the essential steps needed for the system to be operational. As part of the process improvement application, the Milestones framework has been extremely useful to align stakeholders’ understanding of how the CRVS system operates and the need to standardise procedures assigning functions within and between institutions. It has also facilitated the design and integration of new interventions to improve CRVS performance by exposing the implications of the new activities for existing operating procedures and highlighting responsibilities and roles among CRVS stakeholders. Finally, the Milestones framework has also been key to structure the legal review undertaken by some countries to map all existing laws and regulations governing CRVS systems.9
Following CRVS processes mapping and modelling and the application of this framework, countries have focused on ensuring that guidance, forms and standard operating procedures are in place at each step, thus facilitating the transfer of information from each step to the next, and ensuring the overall coherence of the process from the occurrence of a vital event to its incorporation into the vital statistics system. The systematic application of this framework will improve the design and operations of CRVS systems by providing a systemic view of CRVS processes from end to end including all subprocesses, thus enabling the identification of innovative solutions to improve performance. Anticipated outcomes from the application of the method will be an enhanced experience for individual and families wishing to register vital events, improved completeness of registration and better quality resulting vital statistics.
Footnotes
Handling editor Seye Abimbola
Contributors DCM drafted the first manuscript of the comment and all authors contributed equally to the final version of the manuscript.
Funding This study was funded by Bloomberg D4H Initiative via the University of Melbourne.
Competing interests None declared.
Patient consent Not required
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data from the study.