Article Text

Statistics from Altmetric.com
Introduction
A kind of courtship is going on between proponents of universal health coverage (UHC) and proponents of global health security (GHS). In our opinion, efforts to make progress on the path to UHC and efforts to improve GHS can be synergistic, but are not self-evidently so. Making this partnership work will require careful thinking and planning.
Several comments on ‘lessons from Ebola’ highlight the potential of UHC as a way to improve GHS.1 Simon Rushton, Louis Lillywhite and Bhimsen Devkota argue that the “[p]romotion of health security therefore entails ensuring that effective health systems exist before a crisis, are sustained during and after conflict and disaster, and are at all times accessible to the population.”1 Rob Yates, Ranu Dhillon and Ravi Rannan-Eliya remind us that several epidemics of global concern ‘occurred in settings without universal health coverage where health systems were unable to perform effective public health functions’.1 In a reaction to these ‘lessons from Ebola’, and a preview to the G7 summit in Ise-Shima of May 2016, Gavin Yamey argued that a way to make the case for UHC more compelling ‘could be to link UHC to the worldwide concern about pandemics in the wake of the Ebola crisis’,2 and he encouraged Japan—a longstanding proponent of UHC and GHS—to ‘rouse the G7 nations into action on universal health coverage’.2 Japan indeed promoted UHC and GHS, as an ‘inseparable couple’,3 and the ‘G7 Ise-Shima Vision for Global Health’ outcome document highlights both.4
Not a new attempt to create an alliance
The present courtship is not new. The 2007 World Health Report, on ‘A safer future: global public health security in the 21st century’,5 highlighted the importance of strong health systems to enhance GHS. Without using the expression UHC, this report tried to tie efforts to make progress towards UHC into the GHS agenda. For most low-income and middle-income countries, this was self-evident, but not for high-income countries. As Aldis explains, there was a very different understanding of the meaning of ‘health security’: “Policymakers in industrialized countries emphasize protection of their populations especially against external threats, for example terrorism and pandemics; while health workers and policymakers in developing countries and within the United Nations system understand the term in a broader public health context.”6 The division went as far as causing the banning of the GHS expression from later WHO reports: “At the 122nd EB [Executive Board]—the first EB meeting after the release of the 2007 World Health Report—the delegate from Brazil went to considerable lengths to stress that there was no consensus about the use of the phrase ‘global health security’ or its meaning.”7
Pitfalls
In our opinion, efforts to make progress on the path to UHC and efforts to improve GHS are not an ‘inseparable couple’. They can be synergistic. In well-funded, well-staffed and well-equipped health systems, efforts to improve UHC and efforts to improve GHS are indeed inseparable: every dollar spent, every hour of a health worker, every effort, contributes to both, at least indirectly—if only by building trust in the system, which will encourage people to come forward when some new epidemic hits, and to follow the advice of health workers. But especially in an underfunded and underdeveloped health system, the obvious ‘next step’ on the path towards UHC is not always the obvious ‘next step’ in the direction of GHS. For example, if a ministry of health, responsible for an underfunded and underdeveloped health system, must make a choice between improving the laboratory functions, or expanding the health workforce, prioritisation of GHS may lead it in the direction of laboratory functions, while prioritisation of UHC would probably lead it in the direction of expanding the health workforce.
Furthermore, the lack of a clear consensus on what UHC means makes it vulnerable to being deeply influenced by being linked with GHS. For some, progress towards UHC requires a substantial increase in public financing, because private financing, even if pooled in the form of voluntary insurance schemes, appears to be most often regressive (‘groups with a lower income contribute a higher percentage of their income than do groups with a higher income’).8 For others, it does not really matter whether additional financing for UHC comes from public or private sources, as long as it is pooled, and moves away from out-of-pocket expenditure.9 As long as no policy agreement is found on this crucial issue, tying UHC and GHS together may come with pressure on low-income and middle-income countries to use their limited public financing resources for efforts to control infectious disease (ie, GHS efforts), while relying on private financing for the rest of UHC. This would take us back to the health sector reform promoted by the World Bank in 1993 (and following years), under which governments should focus their public resources on ‘public health’—and in the fine print, it was clarified this meant infectious disease control—while for the financing of ‘essential clinical services’, the report suggested “[c]ommunity-financing schemes, whereby patients at local health centers and pharmacies pay modest fees.”10
Opportunities
How then would UHC benefit from being linked with GHS? As Adam Kamradt-Scott puts it: “it conceivably could still prove to be a very valuable political tool for improving the health outcomes of people all over the world due to the simple fact that security, like sex, sells.”7 However, whether that assumption holds true remains to be verified. This assumption is based on one of the dominant explanations for the impressive increase in international public financing for the global HIV/AIDS response, namely that high-income countries are preserving their own interests by trying to control HIV/AIDS in other parts of the world, but there are alternative explanations for the global HIV/AIDS response, namely the influence of global advocacy networks.11 Furthermore, although the International Health Regulations (IHR) include a section on international ‘collaboration and assistance’,12 achievements in this area (since the revision of the IHR in 2005) are rather disappointing. According to Suman Paranjape and David Franz, the so-called Global Health Security Agenda (GHSA), launched in 2014 by the USA with the explicit intention to promote ‘collaborative, capacity-building efforts to achieve specific and measurable targets around biological threats, while accelerating achievement of the core capacities required by the WHO's International Health Regulations (IHR)’,13 started with a budget of US$63 million in 2014: a small fraction of the $8.5 billion the USA intended to spend on global health in 2014.14 If ‘enlightened self-interest’ were the main driver of international public financing, one would expect to see more.
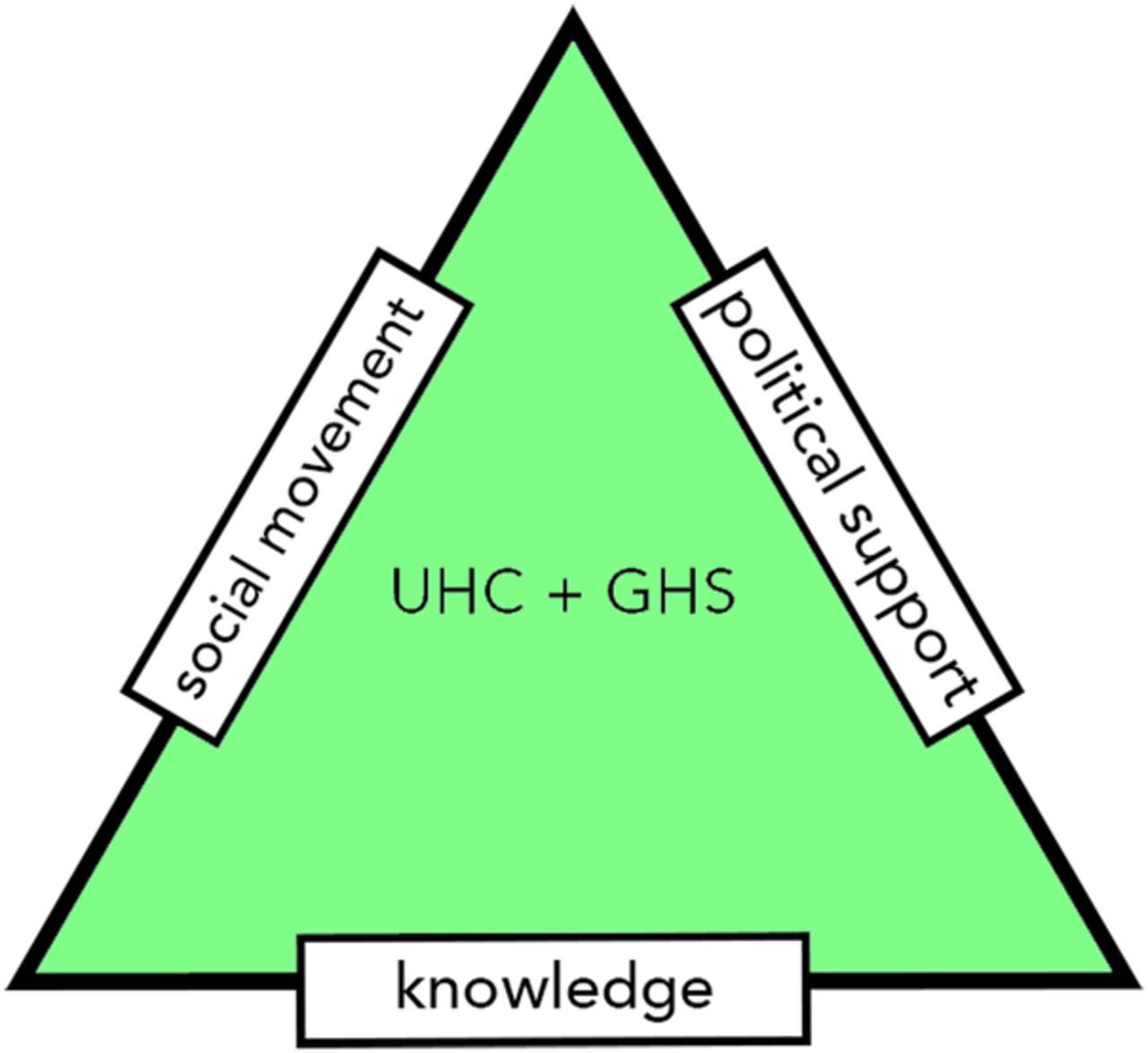
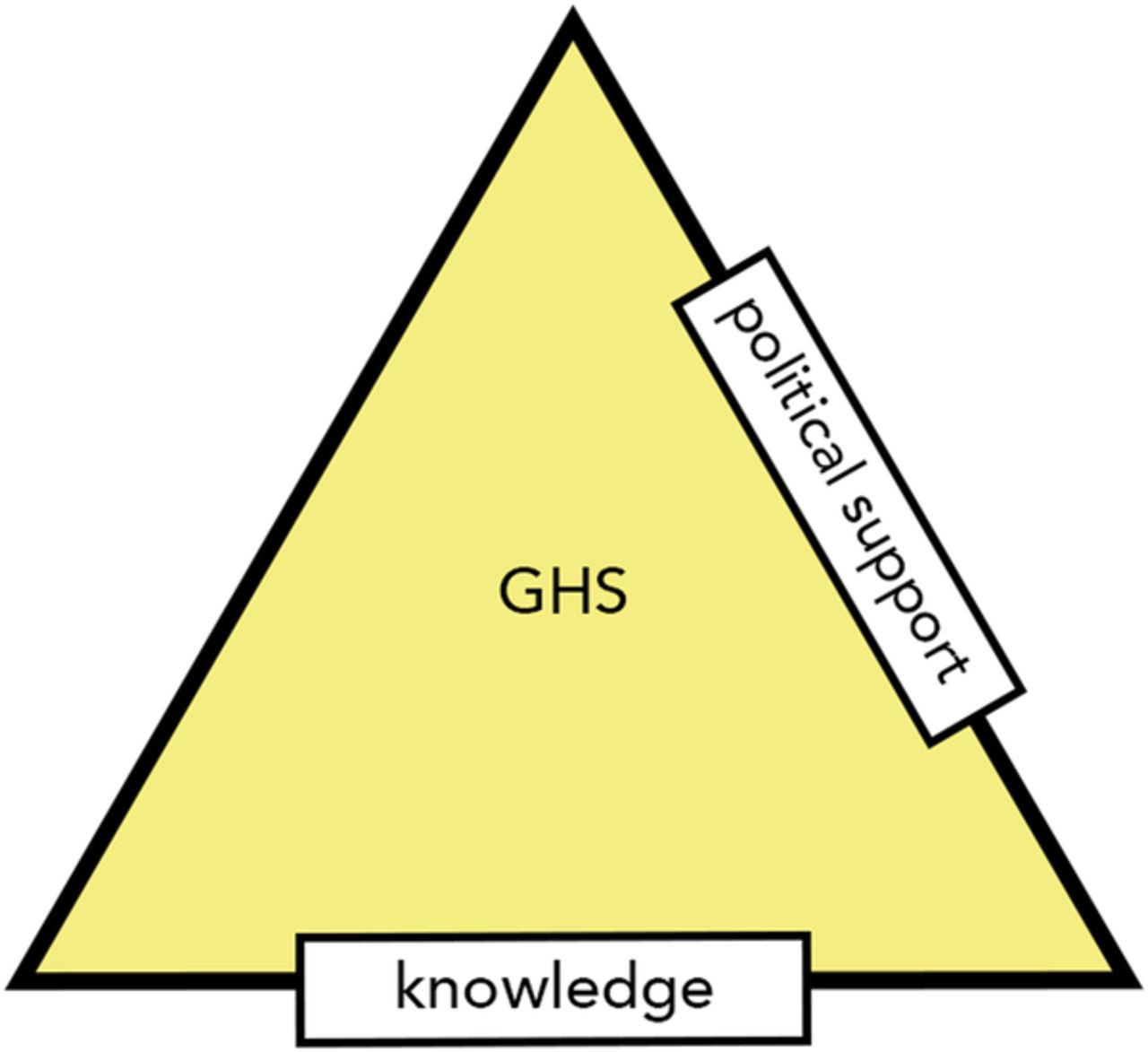
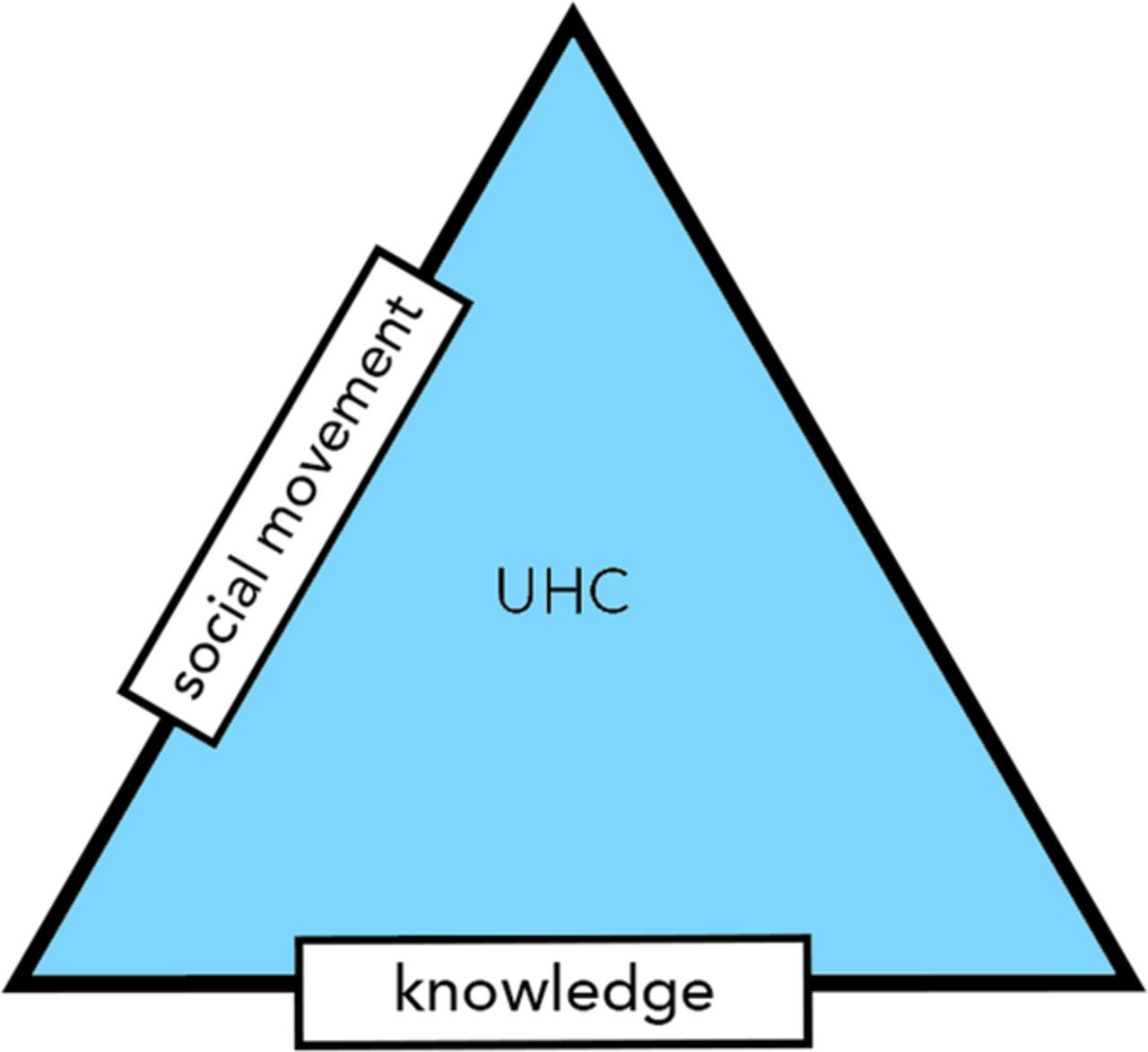
Nonetheless, we presume that when proponents of UHC try to link UHC with GHS, they aim for the kind of political support (of high-income country governments) that UHC alone would not receive, because of being primary focused on the well-being of the inhabitants of low-income and middle-income countries. Likewise, when proponents of GHS try to link their agenda with UHC, they probably hope to attract support from civil society groups and governments of low-income and middle-income countries, who feel that ‘securitization predicates Western, high-income countries’ interests above others’.7 In as much as the ‘triangle that moves the mountain’—a concept originally used to explain how the combination of knowledge, social movement and political support enabled health sector reform in Thailand15—an alliance between the GHS and UHC agendas could create a ‘complete’ triangle: knowledge, social movement and political support. Figures 1⇓–3 illustrate this.

Triangle for global health security.

Triangle for universal health coverage.
{kind=link}
{kind=link}
{kind=link}
Triangle for universal health coverage+global health security.
Conclusion
Based on the considerations above, we would conclude that the courtship between UHC and GHS could at best result in a marriage of convenience. And such a marriage of convenience should be properly planned. The challenge or opportunity is not an entirely novel one: when the global AIDS response started becoming serious, everyone agreed that the provision of AIDS treatment in low-income and middle-income countries would require stronger health systems. The global HIV/AIDS response came with opportunities for health systems strengthening, but also with pitfalls; what McCoy et al wrote at the time—“positive benefits will only happen if we explicitly set out to achieve them”16—seems valid too for the potential alliance between GHS and UHC. The question whether AIDS treatment efforts and programmes strengthened or weakened health systems divided the global health community during almost a decade.17 ,18 It was resolved, at least to some extent, when in 2008, WHO launched the ‘Maximizing Positive Synergies’ initiative, intended to make sure that the disease-specific global health initiatives like, for example, the Global Fund to fight AIDS, Tuberculosis and Malaria, would strengthen health systems, not burden them.19 During a year, more than a hundred scholars, policymakers and civil society representatives worked together, to examine the evidence of synergies and tensions, and to formulate recommendations intended to maximise the synergies and to overcome the tensions. In our opinion, WHO should now do something similar, to maximise the synergies between efforts to promote GHS and efforts to promote UHC.
Acknowledgments
The authors want to thank Jonas Ooms for designing the illustrations.
Footnotes
Handling editor Seye Abimbola.
Twitter Follow Gorik Ooms @GorikOoms
Contributors GO wrote the first draft of the manuscript. CB, WF, JH, OM, MM, TO, MS and AJ contributed to the writing of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.