Universal health coverage, health systems strengthening, and the World Bank
BMJ 2017; 358 doi: https://doi.org/10.1136/bmj.j3347 (Published 31 August 2017) Cite this as: BMJ 2017;358:j3347Read the full collection

- Marlee Tichenor, postdoctoral research fellow,
- Devi Sridhar, professor and chair in global public health
- Correspondence to: M Tichenor Marlee.Tichenor{at}ed.ac.uk
Key messages
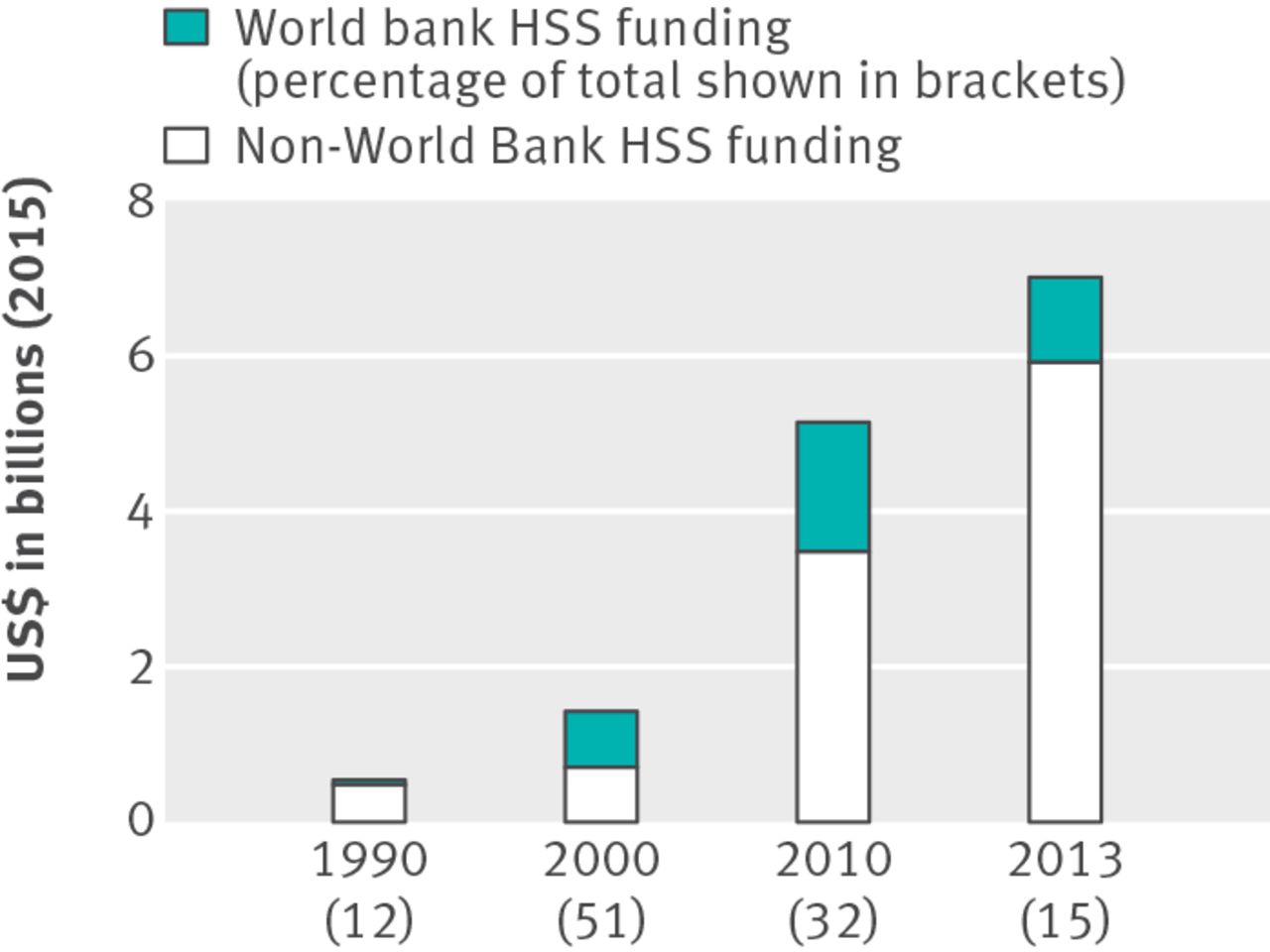
In the era of sustainable development goals, the World Bank plays a pivotal role in promoting universal health coverage and strengthening health systems. In 2010, the bank provided 32% of the global health systems support budget
The World Bank’s health policy focus has shifted from population control (1970s), to primary healthcare direct lending (1980-6), to health reform (1987-96), to the enhancement of healthcare systems (1997-2007), to a health systems approach (2007-present)
The World Bank has a comparative advantage over WHO to lead the universal health coverage agenda given its access to ministries of finance, its staff expertise in measurement, its broad multisectorial portfolio, and its lending power
The World Bank’s expanded role in global health carries with it the risks of further privatisation of the health sector and major tension between its mandate and the right to health at the heart of universal health coverage
The sustainable development goals (SDGs) formally promote universal health coverage as a key objective for the global health community. This focus on universal health coverage arose both from a desire to maintain the health gains achieved by the millennium development goals and from criticism that those goals were short term in nature and narrowly focused on disease specific approaches.12
On 12 December 2012, universal health coverage had unequivocal endorsement from the UN General Assembly (including the United States) with the approval of a resolution that confirmed the “intrinsic role of health in achieving international sustainable development goals.”3 Also in 2012, a World Health Organization discussion paper on the post-2015 health agenda (what would emerge as the SDGs) identified universal health coverage as a “way of bringing all programmatic interests under an inclusive umbrella.”4 The 2014 Ebola virus outbreak struck in the middle of deliberations on the SDGs, and reviews of the global health community’s response to the epidemic have emphasised the importance of health systems strengthening to achieving equitable, accessible, and resilient healthcare.56
In this paper, we examine the World Bank’s past and present role in health systems strengthening within the current global health architecture, and critically analyse several points this raises.
The governance of health systems strengthening
Despite universal health coverage’s growing prominence, the term and its relationship to health systems strengthening are under debate.7 To better understand trends in the World Bank’s investment in health systems and its role in promoting universal health coverage, we must find workable definitions for the terms. The World Bank defines health systems as “the combination of resources, organisation, financing, and management that culminate in the delivery of health services to the population.” While WHO’s definition is “all activities whose primary purpose is to promote, restore, and maintain health.”89 The term “health systems” has, in the last decade and a half, brought with it systems thinking. As a result, health systems—which are understood to include public and private sectors, communities and families, and health financing bodies and pharmaceutical companies, among other health related organisations—are understood to be “complex adaptive systems” that are continually reorganising in “both formal and informal ways” and unpredictably reacting to inputs into the system.910
Within the SDGs, universal health coverage includes “financial risk protection, access to quality essential healthcare services, and access to safe, effective, quality, and affordable essential medicines and vaccines for all.”11 Health systems strengthening, then, is often taken to indicate the actions taken to achieve the goal of universal health coverage and is often framed as the horizontal approach in contrast to disease specific or vertical approaches.1213
Because the definition of a health system is different in different organisations, the means of strengthening it are similarly varied. The bank emphasises that strengthening health systems requires attending to the many actors, commodity chains, policies, and financing mechanisms that make up a country’s health system. To the bank, strengthening health systems involves “enhancing public-private partnerships,” “setting up the right payment mechanisms,” and “ensuring the right logistics,” among many other interventions.9
However, the bank’s approach is just one of several institutions in the global architecture (table 1⇓, figures 1, 2, 3⇓). For example, in recent years the Global Fund to Fight HIV/AIDS, Tuberculosis, and Malaria, along with Gavi, have increasingly channelled funding to strengthening health systems, albeit with a restricted agenda tied to these three diseases, thereby promoting a diagonal approach that mirrors the 1980s movement of “selective primary healthcare” (table 1⇓). WHO first focused on the right to health at its 1978 Alma-Ata Conference; in recent years, however, it has focused on technical support through creating better metrics for measuring progress towards universal health coverage and quality of strengthening health systems.14 The Bill and Melinda Gates Foundation is largely involved with the universal health coverage agenda through its work with WHO and the World Bank on their existing initiatives and supporting the Global Financing Facility at the World Bank.15


{kind=link}
{kind=link}

Fig 3 World Bank commitments to health systems performance
{kind=link}
The World Bank’s history in strengthening health systems
Since its first funded health project in Jamaica in 1970, the World Bank has devoted much of its health financing to strengthening health systems, defining that elusive term here as a broad based, multisectorial, and infrastructural approach to developing health systems. Using the Independent Evaluation Group’s timeline, the bank’s policy focus has shifted from population control in the 1970s, to primary healthcare direct lending from 1980 to 1986, to health reform from 1987 to 1996, to the enhancement of healthcare systems from 1997 to 2007, to a health systems approach from 2007 to the present.213
The inaugural health sector project in Jamaica marked the first trend in the bank’s policy focus in health: population control. Of the $2m (£1.6m; €1.8m) invested in the programme, 84% was spent on the expansion and remodelling of Jamaica’s major maternity hospital and the construction of 10 rural maternity centres. With important exceptions—like the Onchocerciasis Control Programme established in 197418—the bank’s early interest in the health sector was rooted in its desire to “slow down population growth,” ease “population pressure,” and thereby mitigate its “heavy strain on government expenditures on education, health, and housing” in the global south.20 It was within this context of population control that the bank supported infrastructural and technical support of health services.
In 1981, the bank initiated the health and population project in Tunisia, which was arguably its first project explicitly promoting basic healthcare. The project corresponded with a policy shift away from population control towards tackling growing urban-rural disparities and emphasising a preventative approach to healthcare over a curative one. This shift towards primary healthcare was a part of international health development’s emphasis on “health for all” following the Alma-Ata Declaration of 1978. However, because of what the bank saw as systematic constraints that served as obstacles to providing more efficient and equitable health services, it restructured its approach to health sector funding, which is outlined in their 1986 policy document.13
It is in this document—which calls for health reform and more attention to the world’s poor—that the bank’s population, health, and nutrition department (HNP) introduced user charges as a means to equalise access to government run health services in developing countries. They argued that user charges could help make health systems more equitable, considering that the rich—who benefit most from public services—would have to pay. This would theoretically free up government resources that could be directed at programmes and facilities for the poor.21 Like WHO and Unicef’s Bamako Initiative after it, the introduction of user charges led to a further widening of health inequities in many contexts in the global south, producing results at odds with the policies’ intentions.2223
As a result of its health investment restructuring, the bank came to fund “umbrella” projects with other international health financiers at the end of the 1980s and in the early 1990s. These incorporated “capacity building” within larger projects on maternal health and nutrition. The Independent Evaluation Group has pointed out that this restructuring actually isolated bank funded projects from the health ministries of recipient countries and contributed to the fragmentation that had become increasingly part of global health aid.24 The sector-wide approach was introduced in 1997 as a means to “overcome inefficiencies, lack of government ownership, and a number of other problems” constraining international aid.25
The HNP’s 2007 Healthy Development policy document explicitly took on the work and language of health systems strengthening, and re-emphasised the connection between the bank’s goal of eradicating poverty with the financial constraints and risks that illness put on the world’s poor.9 Since 2007, the bank’s investment in strengthening health systems has included many new approaches to financing—for example, the Health Results Innovation Trust Fund, established in 2007; the lending instrument Programme for Results Financing established in 2011; and the recently launched Global Financing Facility. These are all mechanisms with which the bank aims to capture more resources for countries’ health systems for the promotion of equitable, financially accessible healthcare. With these mechanisms, the bank emphasises the importance of including private health services within a holistic view of strengthening health systems. The Programme for Results Financing was established as the third arm next to the bank’s longstanding investment project finance and development policy finance instruments (figure 3⇑). Within the context of innovative financing, there have been some questions about the limits of results based financing, as the Health Results Innovation Trust Fund and Programme for Results Financing lent on the condition of countries’ ability to prove they met certain health indicators. The Global Financing Facility has explicitly not incorporated requirements for results based financing in its framework because of backlash.15
The bank’s current portfolio in strengthening health systems includes project loans, trust funds, partnerships, new lending instruments, and general budget support, among other modalities. Included within this portfolio are partnerships such as the Primary Health Care Performance Initiative and the International Health Partnership, which provide platforms for coordinating between multiple modes of defining, supporting, and measuring strengthening health systems. Along with the World Bank contributions discussed above, figure 3⇑ provides a timeline of trends of when some approaches to strengthening health systems and lending instruments have been introduced and phased out.
Benefits and risks of the bank’s expanding role
With its long standing interest and involvement in broad based health systems support and experience with innovative financing, the bank has strengths that can support universal health coverage. Firstly, because it has access to ministries of finance, the bank can push for universal health coverage in the way no other global health agency can. Secondly, because it is simultaneously a knowledge bank with expert staff, it can drive the development of metrics for monitoring progress towards universal health coverage. In 2015, as a means to monitor countries’ progress towards the goal, WHO and the bank published the first report on measuring universal health coverage, using both the indicator of service coverage and the indicator of financial protection, and putting into motion the close monitoring many believe is necessary for progress towards universal health coverage.26 Thirdly, with its broad portfolio including education, water and sanitation, and transport, the bank can work across sectors to address broader determinants of healthcare access. Finally, with these financial, logistical, and scientific resources on hand, it can leverage the money needed to promote transformative health policy.
However, at least two major risks accompany these potential benefits. Firstly, the bank has been criticised for promoting a diminished role for the state and encouraging the private sector in public health efforts in the global south, through strategies such as structural adjustment programmes and the introduction of user fees, which has increased inequality in some of the poorest countries in the world.22 The move towards funding private hospitals, clinics, and health insurance (such as the Health in Africa initiative) has also been criticised for not reaching those most in need.27
Secondly, the bank’s mandate to create new markets is often in tension with the fundamental concept at the heart of universal health coverage—that access to non-ruinous, quality healthcare is a human right. The idea of universal health coverage is firmly rooted in the right to health, set out in the International Covenant on Economic, Social, and Cultural Rights.28 The bank’s Articles of Agreement, however, state explicitly that it shall not be involved politically with member states and only be motivated by technical and economic considerations. Because of the bank’s role in the promotion of universal health coverage, how it manages this tension will be critical to achieving global access to equitable healthcare.
Universal health coverage: technical or political goal?
At the start of the 21st century, the push for universal health coverage seems stronger than ever. The new WHO director general, Tedros Adhanom Ghebreyesus, asserts that the global health community is recommitted to health as a human right with universal health coverage, echoing the commitments made in 1948 and 1978.29 Over the past decade, WHO and the World Bank have pointed to a lack of metrics for strengthening health systems as hampering efforts. In fact, in a 2013 speech, bank president Jim Kim argued that the Alma-Ata Declaration’s Health for All goal can be achieved in the contemporary era because we have the capacity to measure success towards that goal.30 Yet, while global efforts and consensus towards the importance of universal health coverage are crucial, the real driver of change will come from national stakeholders such as health workers demanding the right to health and pressuring governments to find the mechanisms to deliver this goal. Such political movements have already happened all over the world—such as the launch of Senegal’s Agence de la couverture maladie universelle in 2013, on the heels of years of health union engagement; Thailand’s Universal Coverage Scheme, established in 2001; and Brazil’s Unified Health System, established in 1988.313233
Footnotes
This article is one of a series commissioned by The BMJ based on an idea by the University of Edinburgh. The BMJ retained full editorial control over commissioning, external peer review, editing, and publication. Open access fees are funded by the Wellcome Trust..
Contributors and sources: MT collected the data, analysed it, and drafted the initial version of the paper. DS helped conceptualise and design the study and revised the draft. Competing interests: We have read and understood BMJ policy on declaration of interests and have no relevant interests to declare. This work was supported by the Wellcome Trust [106635/Z/14/Z]. A senior member of the World Bank is on our project’s advisory board.
Provenance and peer review: Commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/.