Article Text

Abstract
Objective To ascertain the cost effectiveness of targeted interventions for female sex workers (FSW) under the National AIDS Control Programme in India.
Methods A compartmental mathematical Markov state model was used over a 20-year time horizon (1995–2015) to estimate the cost effectiveness of FSW targeted interventions, with a health system perspective. The incremental costs and effects of FSW targeted interventions were compared against a baseline scenario of mass media for the general population alone. The incremental cost-effectiveness ratio was computed at a 3% discount rate using HIV infections averted and disability-adjusted life-years (DALY) as benefit measures. It was assumed that the transmission of the HIV virus moves from a high-risk group (FSW) to the client population and finally to the general population (partners of clients).
Result Targeted interventions for FSW result in a reduction of 47% (1.6 million) prevalent and 36% (2.7 million) cumulative HIV cases, respectively, in 2015. Adult HIV prevalence in India, with and without (mass media only) FSW interventions, would be 0.25% and 0.48% in 2015. Indian government and development partners spend an average US$104 (INR4680) per HIV infection averted and US$10.7 (INR483) per DALY averted. Discounting at 3%, FSW targeted interventions cost US$105.5 (INR4748) and US$10.9 (INR490) per HIV case and DALY averted, respectively.
Conclusion At the current gross domestic product in India, targeted intervention is a cost-effective strategy for HIV prevention in India.
- Cost effectiveness
- female sex workers
- health service research
- HIV
- prevention
- targeted interventions
Statistics from Altmetric.com
India initiated the National AIDS Control Programme in 1992, which is currently in the third phase of implementation. The total budgetary outlay of the programme has increased from INR800 million to INR115 830 million from the first to the third phase.1 Prevention has been the mainstay of the programme. Gradually, the major strategy for prevention has shifted from creating awareness through mass media towards a behaviour change communication and providing an enabling environment through peer-led targeted interventions. These targeted interventions have focused on high-risk groups of female sex workers (FSW), men who have sex with men (MSM) and injecting drug users (IDU). The main service targeted interventions for FSW include peer-led counselling for behaviour change towards safer sexual practices, condom promotion, quarterly referral for health check-up and sexually transmitted infection (STI) treatment, and referral and support for accessing antiretroviral therapy (ART) after self-disclosure of HIV-positive status by the FSW to an outreach peer worker. Currently, there are more than 1500 targeted intervention projects, of which more than 1200 are funded by the National AIDS Control Organization (NACO).2
Case studies from India have shown the effectiveness of targeted interventions for FSW in reducing risky sexual behaviour.3–5 Other studies have used mathematical modelling to relate improvements in behaviour, with a declining trend in HIV incidence and prevalence.6 7 A significantly declining trend in HIV prevalence among FSW and the general population was observed in districts that had a high intensity of preventive programmes compared with low intensity districts in four south Indian high HIV prevalence states.2
Other studies conducted in developing and developed countries have also shown that preventive strategies promote safer sexual behaviours8 and are also cost effective.9 10 State-level analyses in India have recently reported targeted interventions to be cost effective in Gujarat state.11 More research has also been carried out to estimate the cost of scale-up of targeted interventions in the former state.12 However, no national-level study has been conducted so far, to inform resource allocation for the country's preventive interventions under the National AIDS Control Programme. The present study was thus conducted to ascertain the incremental cost effectiveness of targeted interventions in India. As female sex work is the major driver of India's HIV epidemic,13–15 a focus on FSW targeted interventions was considered appropriate for the present study.
Methods
General model description
A dynamic Markov model was parameterised on an MS Excel spreadsheet to estimate the incremental cost effectiveness of FSW targeted interventions. Incremental costs and the effectiveness of FSW interventions were estimated against a comparator scenario of mass media interventions alone. A time horizon of 20 years was considered, starting from the base year of 1995. The present study takes a health system perspective. Benefit was measured in terms of HIV infections averted and disability-adjusted life-years (DALY) averted. Both costs and benefits were discounted at 3% to account for time preference of cost and utility.16
Demographic and epidemiological assumptions
We assume the transmission of HIV virus from a high-risk group (FSW) to the client population and finally to the general population (partners of clients) (figure 1). We also include reverse transmission of HIV from clients to FSW, but assume no transmission of HIV from the general population to the client population.

Model structure for transmission of HIV epidemic from female sex workers to clients and general population, India. STD, sexually transmitted disease.
We used census growth rates and behavioural parameters to estimate the year-wise population size of FSW, clients and the general population from 1995 to 201517 (see supplementary table 1, text on pages 2–3, available online only). It is assumed that the FSW and clients are in the age group of 15–45 years and 15–50 years, respectively; and this cycle continues each year with the addition of a 15-year cohort and attrition of a 45 (50 for client)-year-old cohort. General all-cause mortality and HIV-specific mortality from existing Indian studies were applied to each of the population groups to estimate the annual attrition in numbers.18 19 The general population has been divided into married and unmarried cohorts using behavioural sentinel survey data (see supplementary table 1, available online only).20 21
The probability of HIV transmission from men to women and vice versa has been estimated using the Weinstein equation, based on the Bernoulli theorem22 (see supplementary material, pages 5–8, available online only). This equation incorporates the effect of baseline HIV prevalence in the partner group, the risk of HIV transmission per unprotected sex act, condom use rate, effectiveness of condom, average number of sex partners and average number of sex acts per partner. Transmission coefficients for HIV per sex act are derived from epidemiological studies.23–27 We have assumed a rather wide uncertainty range for transmission coefficients as there is a lack of reliable data from India on the risk of HIV transmission per sex act. STI as a cofactor increases the risk of HIV transmission three times.25 28 This has been assumed to be one for a generic sexually transmitted disease (STD). This has also been used in other Indian studies.11 29 It was assumed that it would fit to the overall STD prevalence in different population groups, ie, FSW, clients and the general population.20 21 30–34
Intervention effect
The targeted interventions result in an increase in safer sexual behaviour in terms of a reduction in multipartner sex and the greater use of condoms in commercial sex encounters. The programme incorporates regular quarterly check-ups for detecting any STI. Presumptive and specific treatments for STI are given based on a specified protocol. This results in a reduction of STI prevalence among the FSW. We assume the effect of targeted interventions on condom use, STI treatment/prevalence, number of sex acts and number of sex partners of FSW.1 Data from the two national rounds of behavioural surveillance (2001 and 2006), integrated biological and behavioural surveillance (IBBA) and demographic and health survey data have been used to compute the change in behavioural parameters (table 1).20 21 30 32–56
Demographic, behavioural and biological parameters for the model to assess cost effectiveness of FSW targeted interventions in India
The annual STI prevalence decline was estimated using programme FSW coverage, coverage of FSW for STI treatment and effectiveness of treatment. The probability of FSW getting re-infected with STI after being successfully treated for an episode is also incorporated in the model. FSW targeted intervention projects also treat partners of FSW.1 However, as not all partners (clients) of FSW are treated, we assume that there would be a reduction in client STI prevalence, which is one third of FSW STI prevalence reduction. We assume that any reduction in STI prevalence in the general population women is not the direct effect of FSW targeted intervention projects and thus has not been modelled.
The effectiveness of the mass media in enhancing condom use has been derived from the literature.8 57 Both scenarios of FSW targeted intervention and mass media alone were assumed to operate in a setting in which ART was available. Coverage of ART was estimated from the literature (2% in 2002; 34% in 2008) and trends computed for years in which the coverage estimates were not available.56 58 ART has a lowering effect on HIV transmission as a result of decreased viral load and improved CD4 cell counts. Based on the observed reduction in viral load in blood plasma, experts estimate that ART reduces infectiousness by a factor of 2 to 8.47 59 Because the effect of ART on infectiousness is varied, our analysis uses the base assumption of a decrease in transmissibility by a factor of 4.
Costing
Cost data from an economic perspective on different interventions for all the intervening years is very scarce. Therefore, we have estimated costs from a financial perspective. Cost in a no-targeted intervention scenario relates to the cost of mass media interventions and ART treatment for HIV patients. The targeted intervention arm additionally includes costs for implementing targeted interventions (see supplementary table 2, available online only). The cost of targeted interventions from 2003 onwards is a weighted average cost per FSW enrolled for both NACO and non-NACO including AVAHAN projects, using unit cost guidelines from NACO and AVAHAN (Bill and Melinda Gates Foundation and the Karnataka Health Promotion Trust (KHPT), personal communication, 2010 and A. Bhatia, personal communication, 2009). The weighting was done by the FSW population enrolled in each project according to the funding source. Cost data were validated with estimates on unit costing from other studies.2 11 12 51 The cost of mass media interventions in the targeted intervention scenario was used directly from the NACO financial reports and programme implementation plan outlays published in annual reports1 (table 1).
The model was parameterised with the cost of ART per beneficiary derived from a multicentric study from India (see supplementary figure 1, available online only).55 The unit cost for ART was revised for recent years based on revised estimates of ART costing from NACO guidelines, programme implementation plans and the recent proposal submitted to the global fund.1 60
All costs were converted to constant 2008 prices based on the consumer price index.61 The conversion factor for INR/US$ has been used for 2009. Both costs and benefits have been discounted at 3%.
Valuing benefits
The primary endpoint for estimating benefits was a reduction in HIV cases. As a secondary endpoint, we used standard methods to estimate DALY averted resulting from FSW targeted interventions (see supplementary material, page 9, available online only).62
Sensitivity analysis
Univariate sensitivity analysis was done to ascertain the influence of uncertainty in individual parameters on the summary measure of the incremental cost-effectiveness ratio (ICER). Key demographics (number of FSW, clients and general population), behavioural (condom use, sex behaviour), epidemiological (HIV prevalence among FSW, HIV and STD transmission probabilities, STD cofactor effect), intervention parameters (unit cost of targeted interventions, effectiveness of STI treatment) and discount rate (3% to 8%) were considered in sensitivity analysis.
Using MS Excel and Visual Basic, probabilistic sensitivity analysis was performed. We performed 1000 simulations using a uniform distribution of all parameters for which a plausible range was available (table 1 and supplementary table 1, available online only). Results from simulations were plotted on a cost-effectiveness plane. A cost-effectiveness acceptability curve was constructed to ascertain the probability of the targeted intervention being cost effective at varying threshold willingness-to-pay levels.
Results
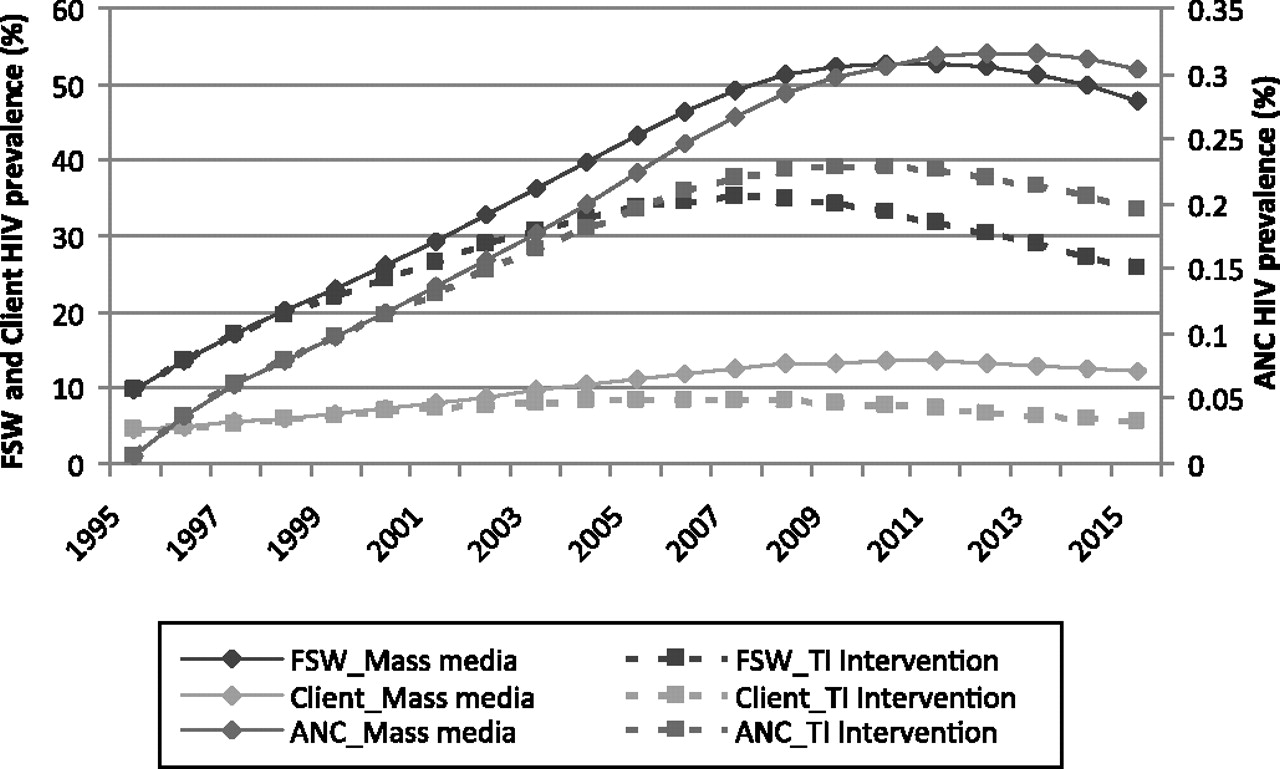
Targeted interventions for FSW result in a reduction of 47% (1.6 million) prevalent and 36% (2.7 million) cumulative HIV cases, respectively, in 2015. The prevalent and cumulative number of HIV cases in 2015, with targeted interventions for FSW, would be 1.8 and 4.7 million, respectively. Similarly, we found that FSW heterosexually acquired adult HIV prevalence in India would be 0.48% in 2015 (figure 2). The same prevalence would be reduced to 0.25% in the scenario of FSW targeted interventions. A reduction in non-condom use alone led to 32% and 40% declines in cumulative and prevalent numbers of HIV infections, respectively, in 2015.

HIV prevalence in India, without targeted interventions (only mass media) and with targeted interventions for female sex workers along with mass media, 1995–2015. ANC, antenatal clinic; FSW, female sex worker; TI, targeted intervention.
The cumulative cost of implementing the FSW targeted interventions scenario from 1995 to 2015 was found to be INR61 693.5 million (US$1991 million) (table 2) with an incremental cost of INR12 841 million (US$285.3 million). From a health system perspective, the government and development partners spend an average US$104 (INR4680) per HIV infection averted and US$10.7 (INR483) per DALY averted. Discounting at 3%, FSW targeted interventions cost US$105.5 (INR4748) and US$10.9 (INR490) per HIV case and DALY averted, respectively (table 2).
Cost effectiveness of FSW targeted interventions for HIV in India
The risk of HIV (4.4–44.7) and STD (4.1–16.7) transmission per sex act, STD cofactor effect (4.4–25.2), client size (5.8–23.4), per unit cost of implementing targeted interventions (4.1–16.6) and FSW condom use (9.9–11.3) were the six parameters that induced maximum variation in the ICER per DALY averted (see supplementary figures 2 and 3, available online only).
Other factors such as HIV prevalence (FSW), the prevalence of sexually active men who report commercial sex activity, the type of sex act, other demographic parameters, efficacy of condom use and STI treatment, condom use among the general population and discount rate were found to have minimal impact on the overall cost effectiveness of FSW targeted interventions.
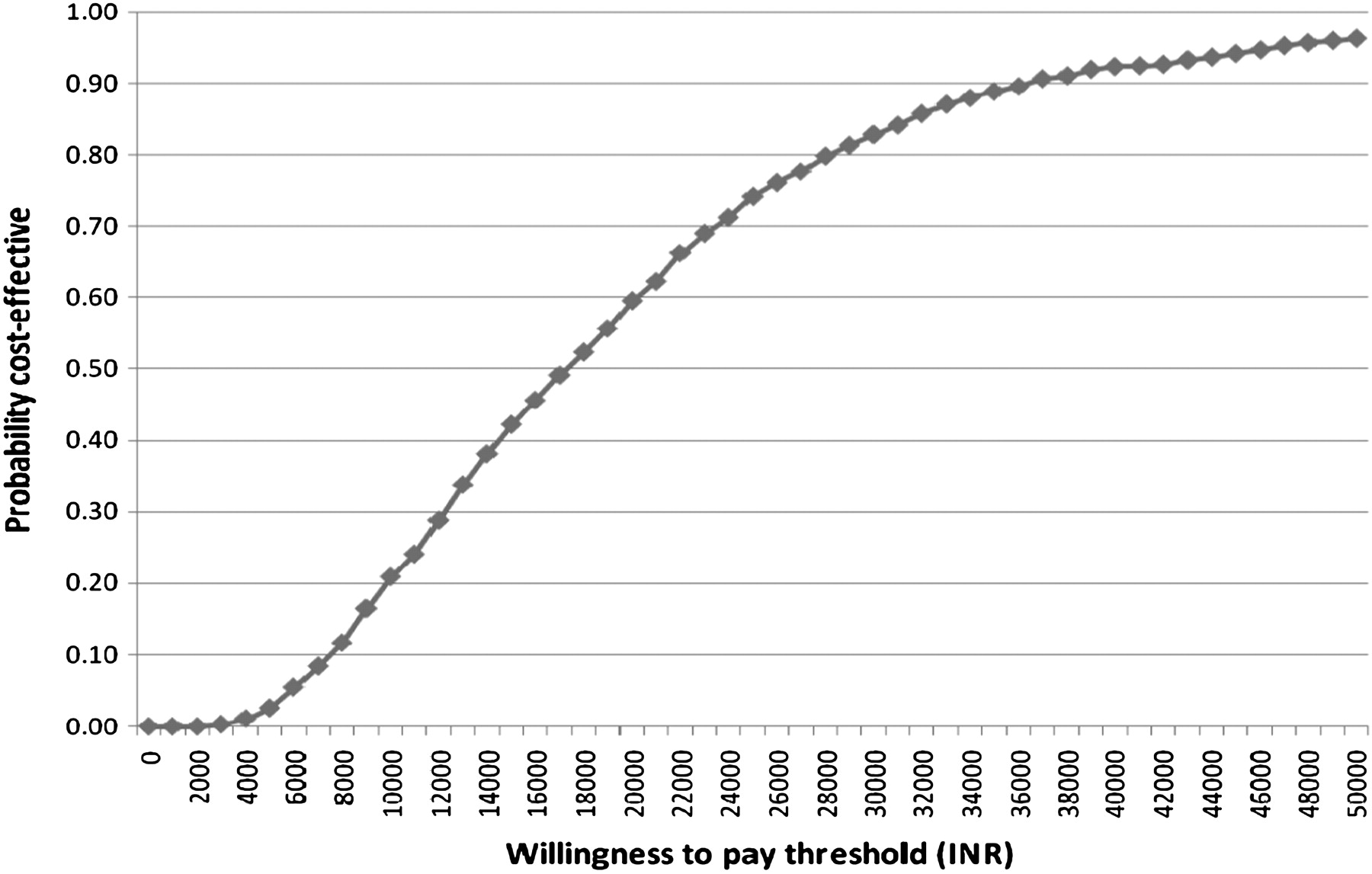
Targeted interventions for FSW are either dominant over the mass media-alone intervention (ie, cost saving) or cost effective at the current gross domestic product (GDP) level. Using 1000 simulations to account for all the parameters' uncertainty, there is nearly 70% probability for the targeted interventions to be cost effective at a willingness-to-pay threshold that is equal to the per capita GDP of India, ie, INR25 393 (figure 3).

{kind=link}
{kind=link}
{kind=link}
Probability of targeted interventions to be cost effective at varying willingness-to-pay levels.
Discussion
We used a compartmental mathematical model to demonstrate the impact of preventive targeted interventions for FSW on HIV/AIDS in India and their cost effectiveness. Targeted interventions for FSW were found to be very cost effective from a health system perspective at US$104 (INR4680) and US$10.7 (INR483) per HIV case averted and per DALY averted, respectively. According to WHO guidelines on cost effectiveness, an intervention is considered to be cost effective if the value of ICER falls between 1 and 3 times the GDP per capita, and very cost effective if it is less than 1 GDP per capita. At a GDP per capita of INR25 393 (US$564) for India, FSW targeted intervention is thus a very cost-effective strategy for HIV prevention.63 Fung et al11 also found similar findings in a model that was parameterised with data from Ahmedabad.
Our model made substantial improvements over the previous models for demonstrating the course of the HIV epidemic in India with or without interventions. Cost-effectiveness studies for preventive targeted interventions in India have used focal non-governmental organisation projects11 or defined geographical area with characteristic behavioural and epidemiological parameters.29 Our model is parameterised with India-specific demographic, behavioural and epidemiological data. The present model also accounts for the evolving nature of targeted interventions in terms of coverage and service provision. We modelled the effect of ART on viral load and its effect on the transmission of HIV, which is an improvement over some earlier models.64 Unlike some previous models64 the cost of ART in our study includes the cost for treating opportunistic infections, besides ART drugs, CD4 cell count testing, healthcare staff and other consumables.
Some of the earlier models have projected the HIV prevalence in India, which peaks to very high levels of almost 25 million cases.65 66 These observations could have resulted from overstated FSW numbers, or other behavioural and epidemiological parameters borrowed from African or other developed country settings. However, we used estimates on the FSW population based on revised mapping studies.38 The sex behaviours of FSW and their clients were reviewed and calculated using data from national-level behavioural surveys and IBBA survey. Our per contact risk of transmission is derived from a review of the literature that also matches with assumptions used in other recent models of HIV transmission in India.6 11 29 The estimates of HIV prevalence in our study are within the range of estimates from HIV sentinel surveillance in India. Our model shows 2.24 million HIV cases at the end of 2007 as against 2.31 million (1.8–2.9) according to revised estimates of HIV sentinel surveillance in India. We did not consider the HIV cases arising as a result of homosexual activity, parenteral and vertical transmission, or heterosexual networks of IDU and MSM. Our estimates should thus be viewed within this limitation. Adjusting for this limitation, the number of HIV-positive individuals in India would be in the range of 2.6–2.8 million assuming that the remaining modes of transmission constitute 25% to 15% of cases in India, respectively.1
Our estimates of the cost effectiveness of FSW targeted interventions (US$104 per HIV case averted) are similar to those of Fung et al11 (US$34–133) from Gujarat and Creese et al64 (US$79–160) from Cameroon but different from those reported by Hogan et al10 for south east Asian (SEAR D) countries, which found targeted interventions to cost $45, $47 and $50 international (2000) at coverage level of 50%, 80% and 95%, respectively. In terms of international dollars, we found FSW targeted interventions to cost $244 international (2005) per HIV infection averted.67 However, these differences are based on differing methodology and assumptions of two studies. Hogan et al10 have hypothetically assumed a scenario of ‘no condom use’ and ‘no STI treatment’ to compare with an alternative scenario of targeted interventions for FSW.
Certain limitations of the present research need to be highlighted. A wide range of STI cofactor effect on HIV transmission as a result of different bacterial and viral STI has been noted.28 However, we have assumed a constant STI cofactor multiplicative effect of 3 for a generic STI. A higher viral load enhances HIV transmission during the sex act.47 Our model uses average per sex act transmission probabilities for HIV acquisition among uninfected individuals. However, we do factor the viral-lowering effect of ART treatment and thus lowered transmission of HIV among those on treatment.
Our predicted HIV prevalence among FSW and clients is higher than those from HIV sentinel surveillance and those reported by Alary et al15 using the IBBA data. FSW HIV prevalence in increasing order is found from HIV sentinel surveillance followed by Alary et al15 (IBBA surveillance data) and is highest according to our study. We would also like to emphasise that the antenatal clinic HIV prevalence predicted from our model matches those from the HIV sentinel surveillance data and the IBBA results. This could be due to the lesser representative nature of sentinel sites for high-risk groups in HIV sentinel surveillance, especially during early years; and the non-random nature of sample collection (for further discussion, refer to the supplementary material available online only).
The present study was limited to an analysis of the cost effectiveness of FSW targeted interventions. Two more approaches for future research on the resource allocation of India's HIV prevention programme are suggested. First would be to look at a broader level and ascertain the impact and cost effectiveness of different preventive interventions such as targeted interventions for MSM, IDU, voluntary counselling and testing centres, mass media, etc. This will inform a better resource allocation decision making in India's National AIDS Control Programme. Second, similar interventions (eg, targeted interventions for FSW) are delivered with different intensity and different strategy (such as NACO-funded projects and AVAHAN-funded projects). Therefore, it is suggested to ascertain the impact and cost effectiveness of different approaches of service delivery at the micro level.
Key messages
We assessed the cost effectiveness of targeted interventions for FSW in India, which is a strategy for the prevention of the focused HIV epidemic among high-risk groups through peer-led behaviour change communication.
Our study found that the targeted interventions for FSW reduced the prevalence of HIV infections in India by 47% from 1995 to 2015.
Using a deterministic model, we found that targeted intervention for FSW is a very cost-effective strategy for HIV prevention in India, with an incremental cost of US$10.7 (INR483) per DALY averted.
Under all uncertainties involved with parameter estimation, we found a 90% probability of targeted interventions for FSW to be cost effective at a willingness-to-pay threshold equal to 1.5 times per capita GDP of India.
References
Supplementary materials
Web Only Data sti.2010.047829
Files in this Data Supplement:
Footnotes
Funding This study was funded by the National AIDS Control Organization, New Delhi, India.
Competing interests All authors have received support from the National AIDS Control Organization, New Delhi, India, for the submitted work.
Ethics approval This study was conducted with the approval of the Ethics Committee, PGIMER, Chandigarh, India.
Provenance and peer review Not commissioned; externally peer reviewed.