Article Text

Abstract
Objective By a randomised, double-blind, placebo-controlled trial of aciclovir 800 mg twice daily for 5 days added to the syndromic management of genital ulcer disease (GUD) to determine the impact on ulcer healing and HIV outcomes.
Methods Patients presenting with GUD in Malawi were evaluated for HIV and herpes simplex virus type-2 (HSV-2) serologies, ulcer aetiology, lesional, genital and plasma HIV-1 RNA and CD4+ count. Patients were followed up at days 2, 4, 7, 14 and 28. The primary study outcome was ulcer healing at day 14, with secondary outcomes being lesional and genital HIV-1 shedding at day 14 and HIV-1 plasma viral load at day 28 among HIV-1/HSV-2 co-infected individuals.
Results Four hundred and twenty-two patients (74% male) were randomised (208 to aciclovir, 214 to placebo), of whom 61% were HIV-1 seropositive and 72% HSV-2 seropositive; 67% (267/398) had HSV-2 ulcers. 85% of ulcers were healed at day 14 with no difference between treatment arms (risk ratio (RR)=1.02, 95% CI 0.93 to 1.11). Among 244 HIV-1/HSV-2 co-infected individuals, aciclovir reduced lesional HIV-1 RNA (adjusted RR=0.64, 95% CI 0.41 to 0.99) and seminal HIV-1 RNA (adjusted RR=0.59, 95% CI 0.40 to 0.88), but not cervical HIV-1 RNA or plasma HIV-1 RNA.
Conclusions Episodic HSV treatment with aciclovir added to syndromic management did not produce a significant clinical benefit in this African population.
- Aciclovir
- genital herpes
- genital ulcers
- trials
- Africa
Statistics from Altmetric.com
Introduction
Genital ulcer disease (GUD) and herpes simplex virus type-2 (HSV-2) infection are associated with an increased risk of HIV acquisition and transmission.1–4 HIV-1 and HSV-2 co-infected individuals experience frequent genital shedding of both viruses.5–7 These synergistic relationships underline the importance of controlling HSV-2 for HIV prevention.8
The WHO recommends the use of syndromic approach for the management of GUD in developing countries.9 In most settings, patients with GUD are treated for bacterial infections but not for HSV-2, the most common cause of GUD nowadays.10 11 Addition of aciclovir has been recommended in settings where the prevalence of HSV-2 as a cause of GUD exceeds 30%,9 but aciclovir is often not available or widely used in resource-limited settings.
HSV-2 is an increasingly common cause of GUD in Malawi,12 13 which may be partly attributable to increasing HIV prevalence and immunosuppression,14–16 resulting in greater frequency and severity of genital herpes lesions.8 However, Malawian national GUD syndromic treatment guidelines (January 2003) did not include aciclovir.17 Sentinel syndromic surveillance established at the Kamuzu Central Hospital (KCH) STI clinic in Lilongwe has shown increased rates of treatment failure among patients with GUD (Phiri S, personal observation). To assist the Ministry of Health revise its guidelines, we conducted a randomised controlled trial (RCT) of the addition of aciclovir to standard syndromic management for episodic treatment of genital herpes. The primary objective of the trial was to determine whether aciclovir offers any clinical benefit when provided empirically to unselected patients who present to the health services with GUD. The primary outcome was the impact of aciclovir on the proportion of ulcers healed 14 days after treatment. Secondary outcomes included time to ulcer healing, and detection and quantity of lesional, genital and plasma HIV-1 RNA among HIV-1-seropositive patients with HSV-2 infection.
Patients and methods
The study was an individually randomised double-blind placebo-controlled trial of aciclovir 800 mg twice daily for 5 days added to syndromic management of GUD. The protocol was approved by the National Health Sciences Research Committee in Malawi and the ethics committees of the London School of Hygiene and Tropical Medicine, the University of North Carolina and the US Centres for Disease Control and Prevention (CDC).
Population and procedures
Consecutive patients attending the KCH/STI clinic with verified genital ulcer(s) between September 2004 and June 2006 were eligible for enrolment if they were aged ≥18 years and living in Lilongwe. Patients were excluded if they were severely ill and required hospitalisation, had severe proteinuria or any contraindications to aciclovir, benzathine penicillin or ciprofloxacin. Pregnant, lactating and menstruating women were excluded. Drugs (including antiretroviral agents) taken before enrolment were recorded.
Eligible patients who provided written informed consent and were willing to be counselled, tested and receive results for HIV/STI were interviewed in the local language (Chichewa) using a standardised questionnaire to collect sociodemographic and sexual history data. A trained STI service provider conducted a genital examination with a detailed description of ulcer(s), including number, location and size. The size of the largest ulcer on the external genitalia was measured using disposable millimetre-calibrated paper tapes, and the ulcer surface area (mm2) was calculated. Speculum and bimanual pelvic palpation were performed for women.
A computer-generated randomisation list was drawn up by the statistician (WCM), with a 1:1 allocation to aciclovir (800 mg twice daily) or matching placebo, using random permuted blocks of size 4, 6 and 8. The randomisation lists were given to Carlsbad Laboratories (San Diego, California, USA), who manufactured and packaged the drugs to maintain allocation concealment. Placebo tablets were identical in appearance, taste and weight to the aciclovir tablets, to preserve blinding by participants and the trial team.
At the end of the randomisation visit, participants received their allocated drugs, plus directly observed syndromic treatment for chancroid (ciprofloxacin 500 mg orally in a single dose) and syphilis (intramuscular injection of benzathine penicillin 2.4 million units in a single dose), STI and HIV counselling, partner notification slips and a supply of condoms. HIV-positive participants were counselled and referred to the adjoining HIV treatment centre (Lighthouse Clinic). Participants were asked to return to the clinic on days 2 or 4 (women only), 7, 14 and 28. At each visit, a brief questionnaire focusing on symptom evolution and intervening sexual history and a genital examination was administered, ulcers were measured for healing and specimens collected. Menstruating women were deferred for genital sampling until the next visit.
During treatment, study nurses assessed adherence by self-report and pill counts, recorded and graded side effects or adverse events and counselled on adherence. Participants whose ulcers had not improved by day 14 (ie, <90% surface area reduction compared with day 0) were given second-line chancroid treatment (erythromycin 500 mg four times daily for 7 days) according to national guidelines. At study exit (day 28), patients with persistently non-healing ulcers (<90% surface area reduction compared with day 0), or with new ulcers, were given open-label aciclovir for 5 days.
Specimen collection and laboratory methods
At day 0, swabs were collected from the largest ulcer to determine GUD aetiology and presence of lesional HIV-1 RNA in HIV-1-seropositive patients. Ulcer aetiologies were determined at the Reference Laboratory and Research Branch, Division of STD Prevention, CDC (Atlanta, Georgia, USA). Real-time multiplex PCR used for the molecular diagnosis of HSV-2, Haemophilus ducreyi and Treponema pallidum was based on TaqMan technology using a CDC in-house protocol. The diagnosis of lymphogranuloma venereum was based on a Chlamydia trachomatis L1–L3 strain-specific, real-time multiplex PCR assay developed by CDC.18
At days 0 and 28, blood samples were tested for HIV, HSV-2 and syphilis serologies, and for HIV plasma viral load and CD4 T-lymphocyte count among HIV-seropositive participants. HIV-1 serostatus was determined at the clinic following a nationally recommended and quality-controlled algorithm (see online supplementary data) using two parallel rapid tests (Determine, Abbott Laboratories, Illinois, USA; and Uni-Gold, Trinity Biotech, Co Wicklow, Ireland), with discordant results resolved using an HIV-1 ELISA (Genetics Systems, Illinois, USA). HSV-2 serology was performed with HerpeSelect IgG2 ELISA (Focus Technologies, Cypress Hill, California, USA) using the manufacturer's cut-off point.19 20 Syphilis serology was performed using a non-treponemal test (rapid plasma reagin, Macro-Vue, Becton-Dickinson, Sparks, Maryland, USA) with reactive samples confirmed by T pallidum haemagglutination assay (Serodia-TPHA, Fujirebio, Tokyo, Japan). Plasma HIV-1 RNA was quantified using Roche Amplicor HIV-1 Monitor Test, version 1.5 (Roche Diagnostic Systems, Branchburg, New Jersey, USA) with a lower limit of detection of 400 copies/ml. CD4 T-lymphocyte count was done using standard flow cytometry (FACScan, Becton-Dickinson). All tests were performed at the HIV/STI laboratory in Lilongwe.
Additional genital samples were collected from HIV-1-seropositive individuals. At all visits, cervical swabs were obtained from HIV-1-seropositive women for the detection of cervical HIV-1 RNA. In HIV-1-seropositive men, a semen sample could not be collected at enrolment, but was requested at all follow-up visits from day 7 onwards. Detection and measurement of HIV-1 RNA in cervical swabs were determined using Roche Amplicor HIV-1 monitor test version 1.5 with a lower limit of detection of 400 copies/ml. Detection and measurement of HIV-1 RNA in lesional swabs and seminal plasma samples were determined using Nuclisens HIV-1 QT (Bio-Merieux, Durham, North Carolina, USA). Lesional and genital samples were analysed at the UNC Retroviral Laboratory in Chapel Hill (North Carolina, USA).
Definitions
Ulcer healing was defined as ≥90% reduction in surface area of the largest ulcer compared with its size at day 0 (D0). Fully re-epithelialised ulcers were considered healed.
HSV-2 ulcers were defined by lesional HSV-2 DNA. First HSV-2 episodes were defined as ulcers with lesional HSV-2 DNA and negative HSV-2 serology. Recurrent HSV-2 ulcers were defined as the presence of lesional HSV-2 DNA with positive HSV-2 serology. Ulcers with bacterial aetiology only were defined as the presence of H ducreyi, T pallidum or lymphogranuloma venereum in the absence of lesional HSV-2 DNA. HSV-2 infection was defined as the presence of HSV-2 DNA in lesion or positive serology.
Statistical methods
Sample size calculations were based on healing rates recorded at the KCH/STI clinic. For the primary outcome, a sample size of 165 patients per arm would provide 80% power to detect a difference in ulcer healing rate at day 14 of 75% in the aciclovir arm versus 60% in the placebo arm at the 95% significance level. Allowing for 15% losses to follow-up, the minimum sample size was 388 patients. This sample size provides 88% power to detect a 50% reduction in detection of genital HIV-1 RNA from 60% to 30% among HIV-1-seropositive patients with HSV-2 infection. Data were double entered using Microsoft Access 2000 and analysed with STATA version 10.0 (StataCorp). Categorical data were compared using χ2 tests. Continuous data were assessed using t-tests if normally distributed, and the Wilcoxon rank sum test otherwise.
The primary analysis used an intention-to-treat approach. The primary end point was at day 14, and visits on days 11–17 were included in this analysis (referred to as the D14 visit). Similarly, the D2 visit includes visits on days 1–4, D7 includes visits on days 5–10 and D28 includes visits on days 25–31. Analysis groups defined a priori were (a) all patients; (b) HIV-1-seropositive patients with HSV-2 infection; (c) HIV-1-seropositive patients with HSV-2 ulcers; (d) HIV-seronegative patients with HSV-2 ulcers. HSV-2 ulcers were further stratified by type (first episode or recurrent).
The impact of aciclovir on ulcer healing at the D14 visit was estimated using Poisson regression with robust standard errors to estimate the RR and 95% CI.21 Kaplan–Meier plots were used to estimate the median time to ulcer healing and the log-rank test to test for statistical significance. Risk ratios were also used to estimate the impact on the presence of lesional, cervical, seminal and plasma HIV-1 RNA, adjusting for the presence of HIV-1 RNA in the corresponding samples at baseline, except for seminal HIV-1 RNA, where no baseline samples were collected and adjustment was by baseline plasma HIV-1 RNA. Linear regression was used to assess the impact of aciclovir on the mean quantity of HIV-1 RNA using similar adjustments.
Results
Figure 1 shows that, between September 2004 and June 2006, 432 of 460 patients presenting with GUD at KCH/STI were eligible and 422 were enrolled in the trial: 208 were randomised to aciclovir and 214 to placebo. Of these, 84% (178 and 176 in the aciclovir and placebo arms, respectively) were seen at the D14 visit.
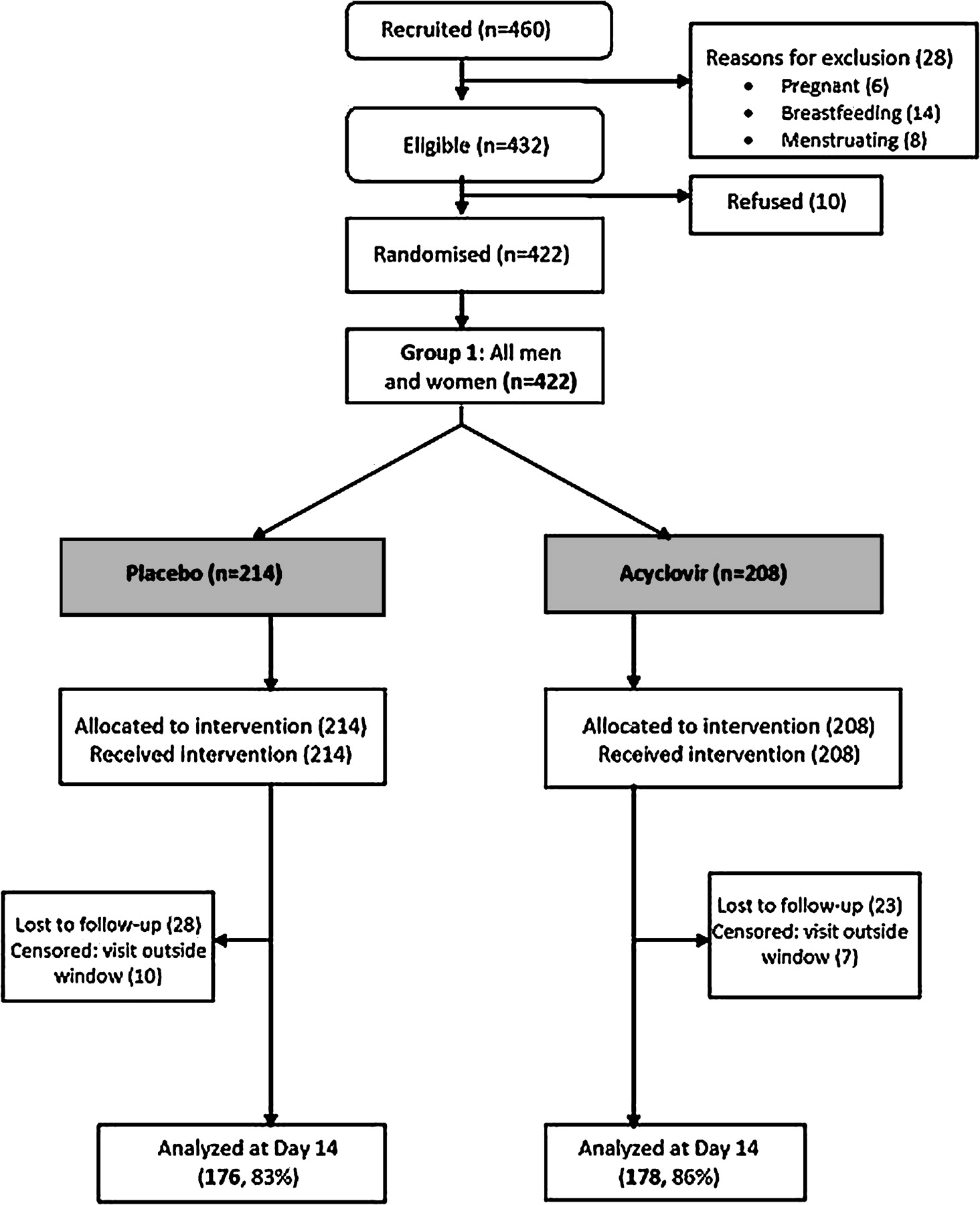
Randomisation and follow-up of patients presenting with genital ulcers at Kamuzu Central Hospital, Lilongwe, Malawi.
Patients in both study arms had similar demographic and behavioural characteristics at enrolment (table 1). The median age was 28 years (interquartile range (IQR) 24–33), and the majority were men (n=313, 74%). The median duration of the ulcer at enrolment was 7 days in the aciclovir arm and 6 days in the placebo arm. Most patients had multiple ulcers (median 2, IQR, 1–4).
Baseline characteristics of 422 patients presenting with genital ulcer disease at Kamuzu Central Hospital, Lilongwe, Malawi
Overall, HSV-2 and HIV-1 seroprevalences were 72% and 61% among all patients, respectively, while 21 patients (5.0%) had active serological syphilis. We tested ulcer aetiology from 398 of 422 patients: and 267/398 (67%) patients had HSV-2 ulcers (67 were first episodes and 196 were recurrences), of whom 216 were HSV-2 only and 51 of mixed aetiology; 52/398 (13%) had a bacterial aetiology only; and 79/398 (20%) had undetermined aetiology (table 1).
Among the 244 HIV-1-seropositive patients with HSV-2 infection, the median CD4 count was 228 cells/μl (IQR, 120–396) and mean plasma HIV viral load (PVL) was 4.87 log10 copies/ml (95% CI 4.76 to 4.97). Among the 179 HIV-1-seropositive patients with HSV-2 ulcers, the median CD4 count was 230 cells/μl (IQR, 111–379) and mean PVL was 4.86 log10 copies/ml (95% CI 4.74 to 4.97). Among the 70 HIV-1-seropositive patients without HSV-2 ulcers, these values were 261 cells/μl (IQR, 171–447) and 4.83 log10 copies/ml (95% CI 4.61 to 5.05), respectively.
Treatment adherence and adverse events
Adherence based on pill count at the D7 visit was high (>95% of participants reported having taken all their tablets). The frequency of side effects was low (8.1% overall) and all were mild to moderate (table 2).
Side effects by treatment group at day 7
Impact of aciclovir on ulcer healing
The majority of ulcers were healed at D14 in both the aciclovir and placebo arms (85% vs 84%; RR=1.02, 95% CI 0.93 to 1.11) (table 3). Healing rates were comparable between arms when stratified by sex, HIV-1 serostatus, CD4 count, type of HSV-2 ulcer (first episode vs recurrent) or duration of ulcer at randomisation, and in the subgroups of HIV-1-seropositive patients with HSV-2 infection or HSV-2 ulcer (table 3).
Effect of aciclovir on ulcer healing among men and women by treatment arm, seen at day 14 visit*
Overall, there was no difference in the median time to ulcer healing between arms (8 days in both arms (IQR, 7–14); p=0.98, figure 2), and no difference in the median size of ulcer by treatment arm, among those with unhealed ulcers (p=0.73). Among both the 244 HIV-1-seropositive patients with HSV-2 infection, and the 179 HIV-1-seropositive patients with HSV-2 ulcers (figure 2), median healing times were 8 days (IQR, 7–14) and 12 days (IQR, 7–14) in the aciclovir and placebo arms, respectively (p=0.70 and p=0.82). Among 152 HIV-1-seropositive patients with recurrent HSV-2 ulcers, healing times did not differ significantly (median time to healing 14 days (IQR, 7–14) vs 13 days (IQR, 7–14); log-rank p=0.67). However, among the 44 HIV-seronegative patients with recurrent HSV-2 ulcers, healing was faster in the aciclovir arm than in the placebo arm (median time to healing 7 days (IQR, 7–10) vs 14 days (IQR, 7–28); p=0.02).
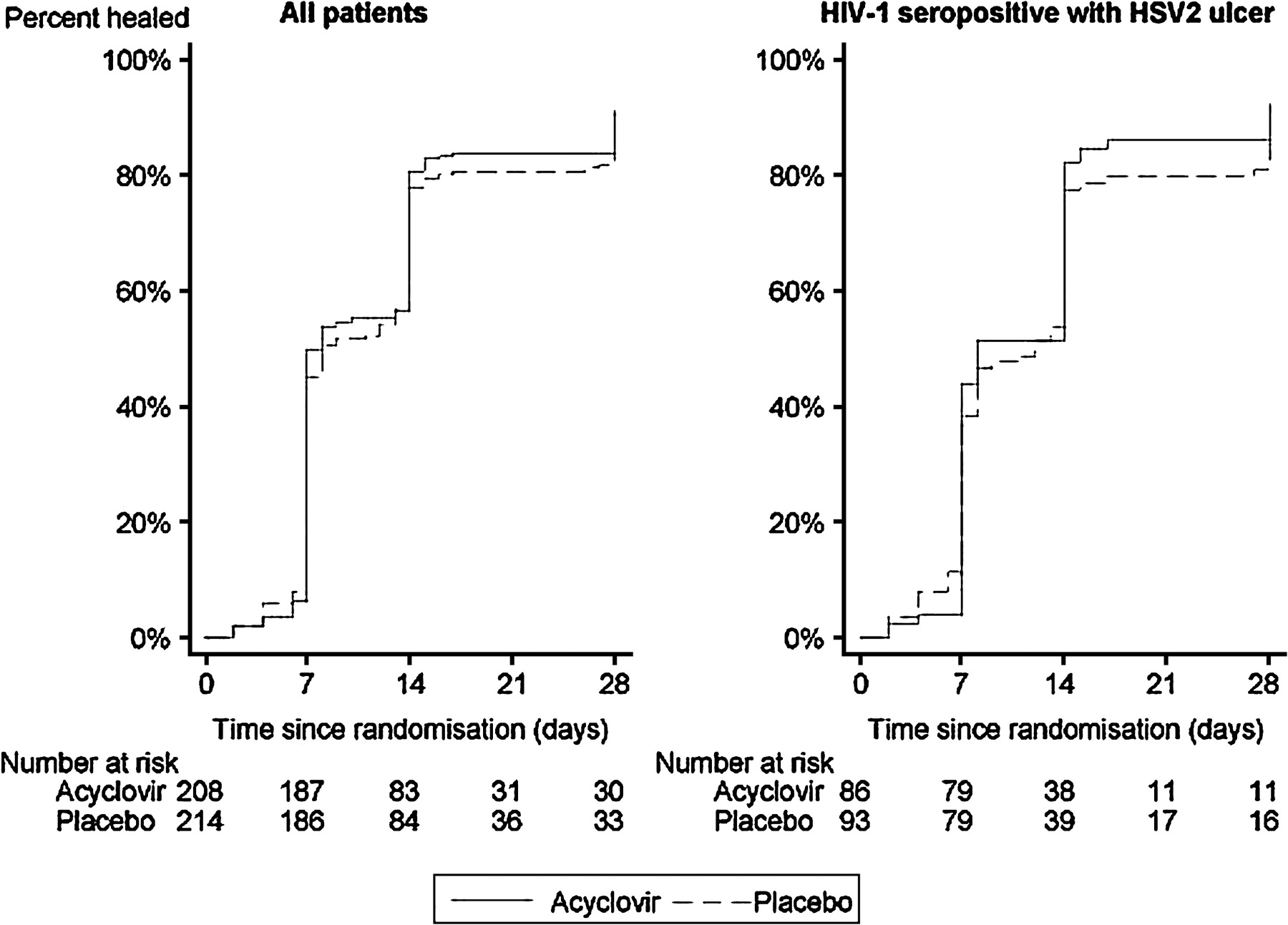
Ulcer healing in all patients and among HIV-1-seropositive patients with HSV-2 ulcers.
Impact on lesional, seminal, cervical and plasma HIV-1 RNA
Two hundred and six of the 244 (84%) HIV-1-seropositive patients with HSV-2 infection were seen at D14, and ulcers were still present in 34/206 (17%), 16 and 18 patients in the aciclovir and placebo arms, respectively. Patients in the aciclovir arm were less likely to have detectable lesional HIV-1 RNA than those in the placebo arm (56% vs 76%; adjusted RR=0.64, 95% CI 0.41 to 0.99; table 4). However, the viral loads were similar across arms among the 26 patients with detectable virus (RR=0.36 log10 copies/ml, 95% CI −0.47 to 1.19; table 4).
Effect of aciclovir on lesional, seminal, cervical and plasma HIV-1 RNA among HIV-1 positive patients with HSV-2 infection, by treatment arm, seen at day 14 visit*
The proportion of men with detectable HIV-1 RNA in semen at D14 was lower in the aciclovir arm after adjustment for baseline PVL (adjusted RR=0.59, 95% CI 0.40 to 0.88). Among those with detectable virus, the mean quantity of seminal HIV-1 RNA did not differ after adjustment for baseline PVL (p=0.62) (table 4). In repeated measures analysis, there was some reduction in the proportion of men with detectable seminal HIV-1 RNA among HIV-1-seropositive patients with HSV-2 infection over time (adjusted RR=0.75, 95% CI 0.51 to 1.09; p=0.13; figure 3).

{kind=link}
{kind=link}
{kind=link}
Proportion of men with detectable seminal HIV-1 RNA among HIV-1-seropositive men with HSV-2 infection.
Among women, aciclovir had no significant impact on detection of cervical HIV-1 RNA at D14 (adjusted RR=0.83, 95% CI 0.56 to 1.22) or on mean quantity of cervical HIV-1 RNA among those with detectable virus (p=0.77) (table 4), or over time (data not shown).
Overall, aciclovir did not affect the mean quantity of plasma HIV-1 RNA at D28 (adjusted coefficient 0.09, 95% CI −0.08 to 0.26; table 4).
Discussion
This is one of three RCTs designed to evaluate the impact of adding aciclovir to GUD syndromic management on ulcer healing. As far as we know, this study is the first to include both sexes, and to measure the impact of episodic treatment on seminal plasma HIV-1 RNA. These trials follow an international research agenda outlined by WHO22 and conducted to inform national and international GUD management guidelines.
Our results show that aciclovir at the recommended dosage and duration9 23 did not provide improved ulcer healing over that provided by syndromic management. These results are consistent with an episodic treatment trial among women with GUD in Ghana and the Central African Republic.24 In contrast, a similar trial conducted among South African men showed that healing was increased by a median of 3 days at the D7 visit, in a population with slightly higher median CD4 count among HIV-infected individuals (282 vs 232 cells/μl).25 Moreover, the median duration of illness before treatment in the South African study was 1–2 days shorter than in the Malawi and Ghana/Central African Republic trials, suggesting that aciclovir must be used very early to alter the course of a genital ulcer and lesion healing.26 However, it was reassuring to note the effect of aciclovir in reducing time to healing in the subgroup of HIV-negative patients with recurrent HSV-2 ulcers, as would be expected.26 27
Given the high HIV prevalence among patients with STI in Malawi, it was also critical to examine the effect(s) of HIV co-infection. Unfortunately, we found no additional benefit on healing rates of giving aciclovir to HIV-infected patients, contrary to earlier small-scale observational reports.28 However, aciclovir did reduce shedding of HIV in both ulcer lesions and seminal plasma. The concentration of HIV-1 RNA in lesions and genital secretions determines the sexual transmission probability.29 Previous studies have shown that ulcers increase HIV-1 shedding in semen,30 and HSV-2 increases HIV-1 shedding in cervico-vaginal secretions5 6 31 and in genital lesions.7 28 These observations have been ascribed to inflammation and immune reactions caused by HSV-2 reactivation32 33 and molecular viral interactions.34 Most, but not all,35 trials of daily suppressive HSV treatment with aciclovir or valaciclovir have subsequently demonstrated a significant effect on HIV-1 shedding in cervico-vaginal secretions36–40 and in rectal and seminal samples.41 42 Daily long-term aciclovir has also been reported to modestly reduce blood plasma HIV-1 levels,36 38 41 perhaps as a direct antiretroviral effect43 44 or by reducing inflammation and/or viral transactivation.34 In this study, we did not observe any significant impact of aciclovir on plasma HIV-1 RNA, nor would we expect a major change from short-course aciclovir.
These results need to be considered in light of recent RCTs designed to determine the effects of HSV treatment on HIV acquisition35 45 and transmission,46 which showed no impact of HSV suppressive treatment with aciclovir (400 mg twice daily) on HIV incidence. Aciclovir at this dose did not completely prevent recurrent ulcers in these trials, and there is increasing evidence of substantial and prolonged subclinical inflammation in patients with recurrent HSV-2 receiving treatment.47 48
On the basis of our results it would be difficult to recommend inclusion of aciclovir for genital ulcer treatment, except for patients presenting early and in HIV-negative patients with recurrent herpes. Furthermore, the benefits of suppression of HIV in the genital tract whether in a lesion or in semen are unknown since we do not know the exact mechanisms of HIV transmission, or the concentration of HIV required for transmission. Given the high prevalence of HSV-2 and its role in driving the HIV epidemic in Africa,49 more effective ways to combat or prevent HSV-2 infection are urgently needed.
Key messages
Recent trials of herpes episodic treatment in Africa have shown benefits on genital ulcer healing among men, but not among women.
The same trials have shown little impact on lesional and genital HIV-1 shedding among HIV-1/HSV-2 co-infected individuals.
In this trial, among both men and women in Malawi, there was no impact on ulcer healing of aciclovir 800 mg twice daily added to syndromic GUD management.
Among HIV-1/HSV-2 co-infected individuals, aciclovir reduced the frequency of lesional HIV-1 shedding and of seminal plasma HIV-1 detection among men, but not the frequency of cervico-vaginal HIV-1 shedding among women.
Acknowledgments
We would like to thank all men and women who participated in this study, clinical staff at Kamuzu Central Hospital STI clinic and all staff involved in the study from University of North Carolina (UNC) Project teams, both at the Tidziwe Centre in Lilongwe and at Chapel Hill, NC. We also thank members of the Data Safety and Monitoring Committee (Chair: Professor Simon Cousens from the London School of Hygiene and Tropical Medicine, Dr Peter Leone from UNC, Chapel Hill, and the late Dr George Joaki from the UNC Project, Lilongwe). We would like to express our gratitude to the Malawi National STI Task Force chaired by the Reproductive Health Unit of the Ministry of Health who commissioned and supported this study.
References
Footnotes
This work was presented as an oral presentation at the XVII International AIDS Conference, Mexico City, Mexico, 3–8 August 2008: Phiri S, Hoffman I, Weiss HA, et al. Impact of aciclovir on ulcer healing and HIV-1 lesional and genital shedding among patients with genital ulcer disease in Malawi: a randomised controlled trial. (Oral THAC0303).
Funding The study was funded by the UK Department for International Development (DFID) through the Malawi National AIDS Commission, and by grants from the University of North Carolina at Chapel Hill, NC, USA. The views expressed are those of the authors and cannot be taken to reflect the official opinions of DFID, or of the US Centers for Disease Control and Prevention (CDC).
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; not externally peer reviewed.
Linked Articles
- Whistlestop tour