Article Text

Abstract
Objectives: To explore epidemiological evidence about the interaction of herpes simplex virus (HSV) 1 and HSV-2 infections.
Methods: A systematic review was undertaken of published epidemiological studies describing the pattern of HSV-1 or HSV-2 by age, and the coincidence of the two viral infections.
Results: In cross sectional studies the unadjusted odds of HSV-2 are greater in those with HSV-1 infection in study populations categorised as “low risk” (p = 0.06) and across European populations (p = 0.001). This was not evident in “high risk” populations or in the United States. This increased risk of HSV-2 in those with HSV-1 infection does not agree with the results of prospective studies where there is a non-significant trend towards a lower risk of HSV-2 infection associated with previous HSV-1 infection.
Conclusions: “Low risk” and European populations have a relatively low HSV-2 seroprevalence and infection is more concentrated in those with characteristics putting them at high risk for both HSV-1 and HSV-2. This confounding could mask any protective effect of HSV-1, which is hinted at, but not demonstrated, in prospective and adjusted studies.
- herpes simplex virus
- prevalence
- epidemiology
Statistics from Altmetric.com
Herpes simplex virus (HSV) exists as two types, 1 and 2 (HSV-1 and HSV-2), and causes a lasting infection with recurrent lesions. Generally, HSV-1 has been associated with oro-labial disease, with most infections occurring during childhood, and HSV-2 with genital disease with infection following sexual debut.1 However, it is possible for HSV-2 to cause oro-labial herpes and HSV-1 to cause genital herpes.2 Indeed, though the public health impact of oro-labial herpes caused by HSV-2 is probably small, recent studies have shown that HSV-1 infections account for a substantial proportion of genital herpes infections, particularly in Europe,3–7 where, in some settings, HSV-1 has become the most common cause of genital herpes. This crossover may be a result of increased oral-genital contact combined with lower rates of childhood oral HSV-1 infection and hence lower immunity to genital HSV-1 infection.6,7 Genital infection with HSV-1 is associated with less severe disease and fewer recurrences than genital infection with HSV-2,8 although may be more likely to result in neonatal infection.9 Initial transmission of genital HSV-1 probably results from oral-genital contact though subsequent transmission from the infected individual may occur via genital-genital contact. That a concomitant rise in oral HSV-2 has not been seen suggests that either HSV-2 is less capable of causing cross site infection, it is diagnosed less often because of a lack of concern over adult oro-labial herpes, or previous HSV-1 infection is preventing oro-labial infection or disease with HSV-2.
Given that these viruses are closely related antigenically it is possible that previous infection with one HSV type may protect against subsequent infection with the other type. Evolutionary theory would predict selection of viruses sharing the same host so as to avoid cross protection. However, the normally distinct niches provided by oral and genital sites of infection may allow for local cross protection when the viruses invade the same site. The changing risks of neonatal herpes and genital disease associated with increases in genital HSV-1 and the potential for suppressive therapy10 or vaccination11 to alter the epidemiology of the viruses are dependent upon the patterns of infection within communities that can be explored using serological tests.12
The worldwide seroprevalence of HSV-1 and HSV-2 was the subject of a recent thorough review,13 which treated the two viruses separately and found that their epidemiology varied considerably between geographic locations. Studies investigating the interaction between HSV-1 and HSV-2 infection have produced conflicting results, and other studies have collected the relevant data but not investigated this interaction. Here we present a systematic review focusing on Europe and the United States, updating the earlier published review and exploring the effect of previous infection with HSV-1 on the likelihood of subsequent infection with HSV-2 at the individual level.
METHODS
Search strategy
PubMed (1966-present) and EMBASE (1980-present) were used to search for relevant cross sectional studies published since 2002 (it was assumed that all previous cross sectional studies were included in the earlier review13) and prospective studies published in any year. The MeSH terms used in PubMed (date of search 23 June 2003) included “Antibodies, Viral/(analysis/blood/immunology),” “Incidence,” “Prevalence,” “Herpes simplex/(complications/epidemiology/immunology/pathology),” and “Simplexvirus/(immunology/pathology).” Key terms used for the EMBASE search (date of search 19 June 2003) included “Seroepidemiology,” “Incidence,” “Prevalence,” “Herpes Simplex Virus,” “Genital Herpes/epidemiology,” and “Herpes Labialis/epidemiology.” No language restrictions were placed on the searches. Reference lists of prospective studies and recent issues of key journals were also searched. Approximately 2800 references were identified, including those identified in the original seroprevalence review. The abstract of each study was checked in order to discard those clearly not relevant. The full text of the 259 remaining studies (save one unavailable in the United Kingdom14) was obtained.
Inclusion and exclusion criteria
Studies were eligible for the seroprevalence review if they presented cross sectional data on HSV-1 and/or HSV-2 seroprevalence and for the interaction review if they contained prospective data on the number, or proportion, of HSV-1 seropositive (“exposed”) individuals who seroconverted to HSV-2 compared to HSV-1 seronegative (“unexposed”) individuals or cross sectional data on the proportion, or number, of people seropositive for HSV-1 and HSV-2 and the overlap. Additional data were sought where they were only presented graphically or where incomplete data on the association between HSV-1 and HSV-2 were given.15–20 We limited our approach to identifying published studies. The process of peer review should help avoid poorly designed and executed studies, where sampling methods and laboratory tests are sources of error, but this may have led to some publication bias.
Studies were included only if they used type specific antibody assays and (with the exception of prospective studies) provided some indication of subjects’ age. Studies were generally excluded if the study population had been selected on the basis of having a chronic condition (except HIV). In addition, one study was excluded from the seroprevalence review because the proportion of equivocal results was unusually high.21 Sample sizes were required to be at least 20 for inclusion in the seroprevalence review, and at least 10 in each of the exposed and unexposed groups for the interaction review. Studies were excluded from the interaction review if individuals were all seropositive or all seronegative for HSV-1 or HSV-2 in both exposed and unexposed groups. However, if this applied to only one of the groups 0.5 was added to each cell in the 2×2 table of HSV-1 infection versus HSV-2 infection.22,23 For data tables see online supplementary material (www.stijournal.com/supplemental).
Data extraction and analysis
Analysis of the data was carried out using Stata (version 7.0). Study populations were defined as being either “low risk” or “high risk,” as in the earlier review, where “high risk” denotes factors thought to be directly associated with HSV-2 infection, such as seropositivity for HIV, attendance at an STD clinic, commercial sex work, or sex between men and “low risk” includes all populations with no obvious risk of HSV-2 infection. If seroprevalence was recorded over an age range then the midpoint of that range was used to allow for comparisons across studies with different age ranges.
Seroprevalence data were analysed graphically. In comparisons we assumed that age specific seroprevalence was independent of study year, which may not be entirely valid, but to understand changes in patterns of incidence with respect to age and time requires cross sectional seroprevalence data at multiple time points. For graphs, unspecified age specific sample sizes were estimated from the overall sample size and the fraction of all study ages covered by the specific age range. In subsequent analyses only samples with known sample size and finite age limits were included and the proportion infected was recoded as 0.001 (0.1%) and 0.999 (99.9%) for samples with 0% and 100% seroprevalence respectively.24–28 Sample age was categorised as 0–14; 15–19; 20–24; 25–29; 30–39; 40–49; and 50–75 years (40–75 years for the United States), and the meta-regression command used to calculate the overall age categorised seroprevalence of HSV-2 by population risk level and the overall age categorised seroprevalence of HSV-1 with 95% confidence intervals (for n⩾3), using the log odds of infection weighted by the standard error of the log odds.
Data describing the interaction between viruses were analysed using the meta command to calculate unadjusted odds ratios for cross sectional studies and risk ratios for prospective studies, with 95% confidence intervals, using the log ratios and the standard error of the log ratios. Adjusted odds ratios, and their 95% confidence intervals, were used as published. These ratios were presented as forest plots by the mid-point of the study year (or publication year if unknown).29 Because the studies describe the epidemiology of infection which could vary between populations we used random effects models to calculate combined effects. Sources of heterogeneity were investigated by stratifying the unadjusted odds ratios by study location and “risk” of population, easily assessed potential sources of heterogeneity. A stratified analysis was not done for the risk ratios or adjusted odds ratios owing to the small number of samples. Publication bias in the unadjusted odds ratios was investigated using Begg’s funnel plot.
RESULTS
The seroprevalence of HSV-1 and HSV-2
As has been described before there is a clear age dependency in the seroprevalence of HSV-1 and HSV-2 in both Europe and the United States (see online supplementary material). Across all ages the seroprevalence of HSV-1 was generally higher than that of HSV-2, and the seroprevalence of HSV-2 was generally higher in “high risk” populations than in “low risk” populations. These patterns can be seen more clearly in the average age categorised seroprevalence (fig 1). Slight fluctuations in the seroprevalence of HSV-1 in the United States with age are probably the result of the small combined sample sizes in some age categories. The seroprevalence of HSV-1 rises to a plateau at older ages whereas HSV-2 in most populations (the exception being “high risk” US populations) rises to a peak and then declines with increased ages. Unless detectable antibodies are lost at older age this must mean that older individuals during their lifetime have been exposed to HSV-2 less often than subsequent cohorts indicating an increase in HSV-2 over time. Comparing data for Europe and the United States shows similar patterns of HSV-1, whereas the seroprevalence of HSV-2 for both “low risk” and “high risk” populations is considerably higher in the United States.

Overall age categorised seroprevalence of HSV-1 and HSV-2 in “low risk” and “high risk” populations, weighted by the inverse of the study variance, in Europe (A) and the United States (B).
Interaction between HSV-1 and HSV-2 infection
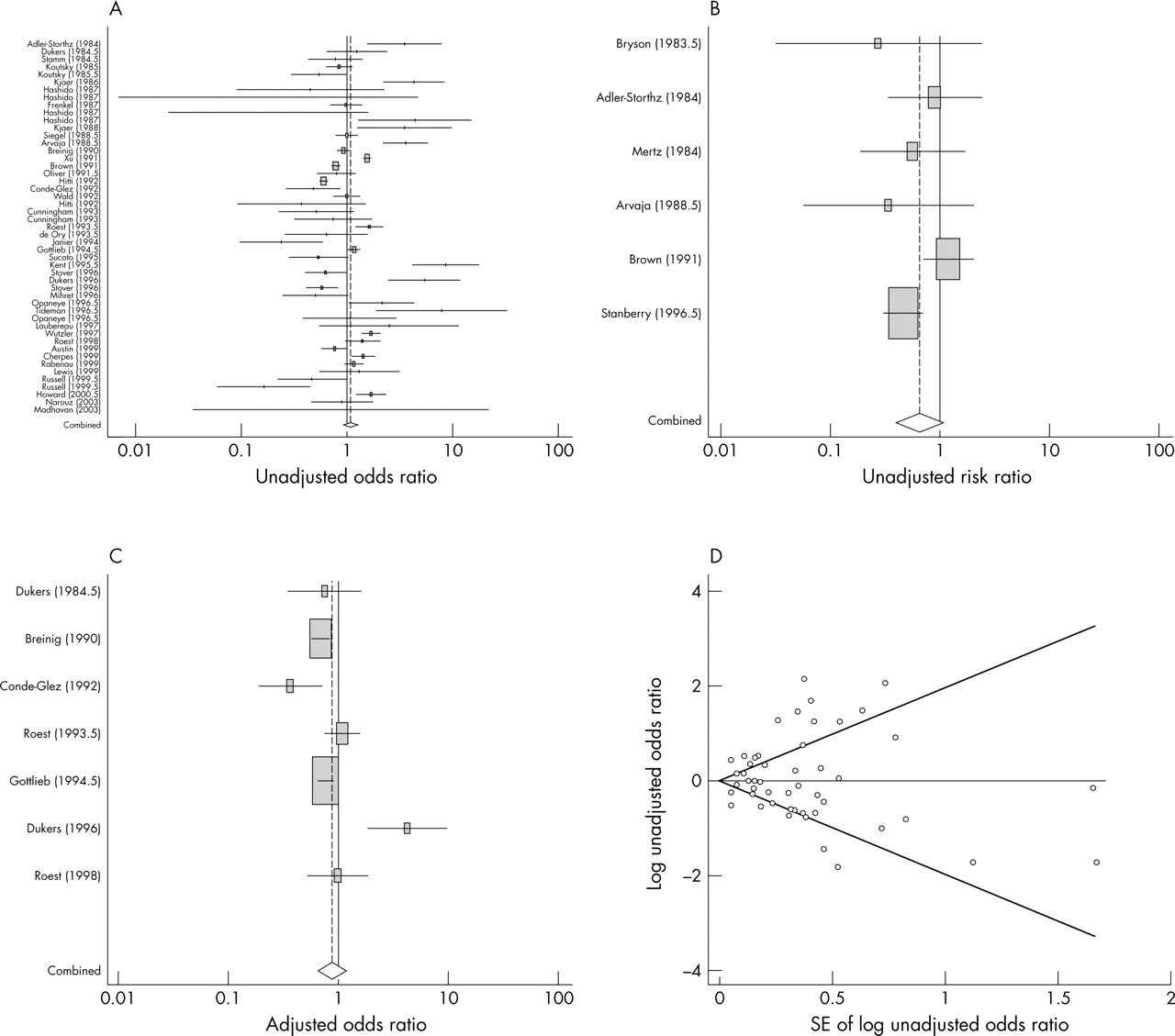
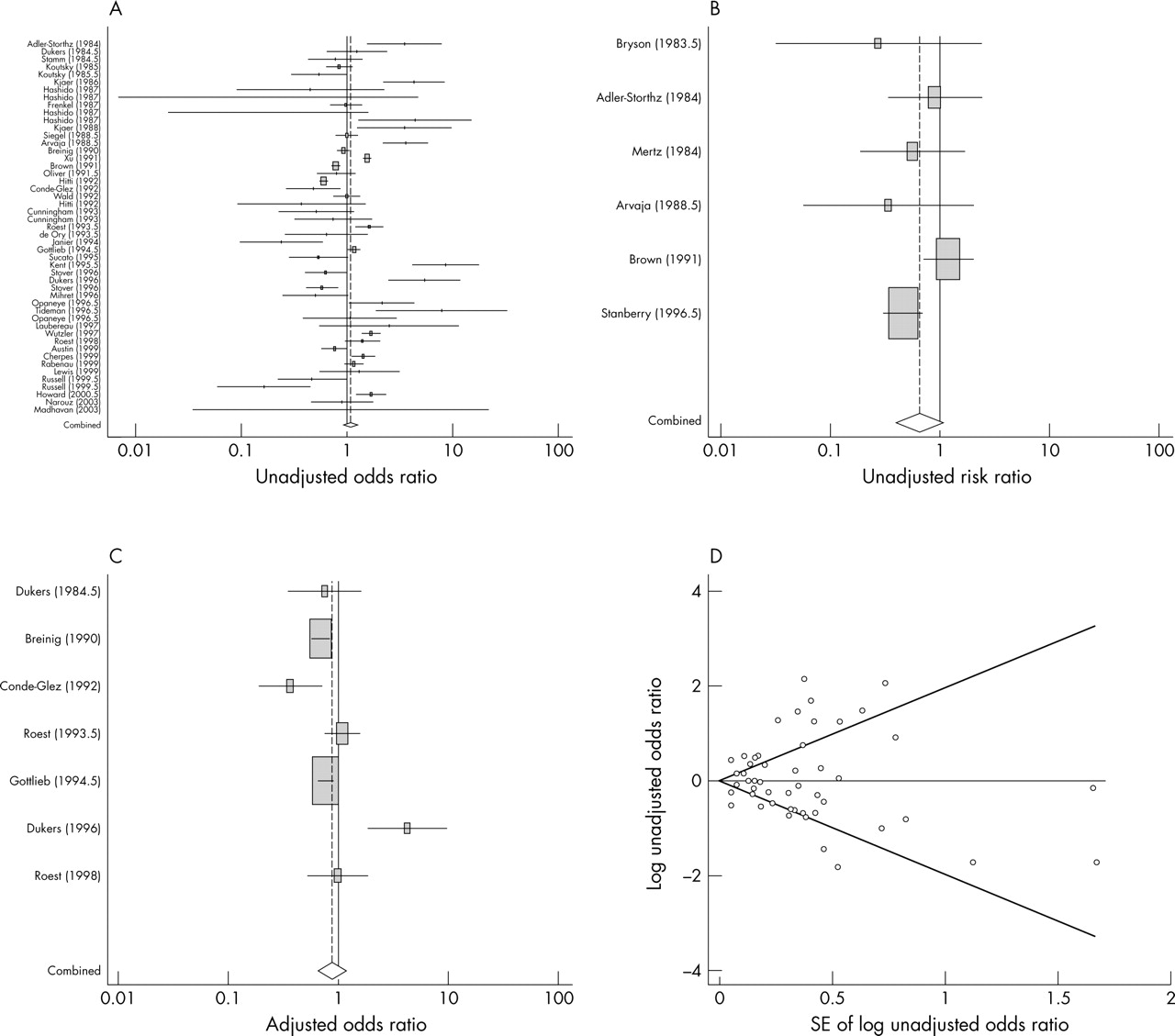
There is statistically significant heterogeneity in the unadjusted odds ratios for the interaction between HSV-1 and HSV-2 infection (fig 2A) with no clear pattern discernible from the unstratified plot (pooled OR for HSV-2 among those HSV-1 seropositive compared to those HSV-1 seronegative, 1.1; 95% CI: 0.9 to 1.3). Stratification by population risk level removes some of the heterogeneity (assessed in stratified forest plots, results not shown), but much remains, with the test for heterogeneity still significant for both “high risk” and “low risk” populations (p<0.001). Here the combined effect is 1.2 for “low risk” populations (95% CI: 1.0 to 1.5; p = 0.06), suggesting that HSV-1 infection is associated with increased odds of HSV-2 infection in this setting, and closer to 1 for “high risk” populations (OR = 0.95; 95% CI: 0.7 to 1.2), suggesting no association. Stratification by study location removes more heterogeneity but again fails in preventing the null model of homogeneity from being rejected in a statistical test. The combined odds ratio for Europe is 1.6 (95% CI 1.2 to 2.2; p = 0.001), suggesting increased HSV-2 in those HSV-1 infected, while the odds ratio in the United States is 0.9 (95% CI: 0.8 to 1.1).
{kind=link}
{kind=link}
The influence of HSV-1 infection on the presence of HSV-2 infection. (A) Forest plot of the unadjusted odds ratios from cross sectional studies for the association between HSV-1 and HSV-2 infection by study year, together with the pooled effect across all studies. (B) Forest plot of unadjusted risk ratios from prospective studies for the risk of infection with HSV-2 among HSV-1 seropositive individuals compared to HSV-1 seronegative individuals by study year. (C) Forest plot of adjusted odds ratios from cross sectional studies for the association between HSV-1 and HSV-2 infection by study year. (D) Begg’s funnel plot for publication bias using the unadjusted odds ratios with pseudo 95% confidence intervals.
In prospective studies the unadjusted risk ratios for HSV-2 as a function of previous HSV-1 generally suggest that HSV-1 is protective (fig 2B). These risk ratios are more homogeneous than the odds ratios with a non-significant test for heterogeneity (p = 0.10). It is important to note that this test has low power, particularly when the number of samples is small. The combined relative risk is 0.6 (95% CI: 0.4 to 1.1; p = 0.08). A non-significant effect is seen from an analysis of the adjusted odds ratios (fig 2C) (OR 0.9; 95% CI: 0.7 to 1.2). One rate ratio was presented which found no effect for HSV-1 on the rate of HSV-2 acquisition (RR 1.0; 95% CI: 0.7 to 1.3).30
The presence of publication bias in the unadjusted odds ratios was investigated using Begg’s funnel plot (fig 2D). For standard errors greater than 1 (corresponding to small sample sizes) there is some evidence of publication bias, as there are three points below the pooled effect and none above it, suggesting that small studies may have been more likely to have been published if they presented odds ratios which showed a negative association between HSV-1 and HSV-2 infection. However, the log odds ratios are generally evenly distributed above and below the pooled effect, and Begg’s test for publication bias is non-significant (p = 0.7).
DISCUSSION
Our review of epidemiological studies identified extensive data on the pattern of herpes simplex virus infections by age and the interaction of type 1 and type 2 infections. However, these studies fail to provide a clear understanding of the relation between the two viruses. Hypothetically, previous infection with one type could lead to cross protection against the other. Less likely, but also possible would be a facilitation of infection with one type by the other. Also likely is there being no direct mechanism for one infection influencing the other. HSV-2 is likely to have evolved so that it is not influenced by previous HSV-1 infection. Since the risk behaviours associated with HSV-1 infection occur at a younger age than those associated with HSV-2 infection, selection for HSV-1 to avoid cross protection from HSV-2 will be less intense. Detecting direct interactions in epidemiological data will be hampered by other risk factors associated with both infections. These could be genetic susceptibility of hosts to both viruses, behaviours which expose individuals to both viruses, or separate risk behaviours for each virus which are correlated. In our review we attempted to avoid such confounding variables by stratifying the population into “high” and “low” risk, but residual confounding is always likely. This is especially true for unadjusted measures of association, but is also true with adjusted measures since risk behaviours are unlikely to be completely measured and there will be heterogeneity between studies. Given such intractable difficulties our analysis was never likely to provide clearcut evidence. However, through combining all available studies we illustrate the limits of available data, and show that if one virus is protective for the other the effect is not obvious.
Combining the unadjusted odds ratios suggests that HSV-1 infection is associated with slightly increased odds of HSV-2 infection in “low risk” populations and in Europe. In contrast, the adjusted odds ratios and unadjusted risk ratios suggest that previous infection with HSV-1 is associated with a slightly decreased, but non-significant, risk of infection with HSV-2. The positive association between the two types was found for populations where the prevalence of HSV-2 was comparatively low. It is likely that “low risk” is a poor description and that these populations include some who are at increased risk of both infections. Since HSV-2 is associated with sexual behaviour and HSV-1 with childhood infection it is likely that risk behaviours are correlated rather than identical, and that sociodemographic or economic variables lead to increased non-sexual and sexual contacts. Factors which could confound the interaction include age, gender, sexual behaviour, ethnicity, socioeconomic status, injecting drug use and HIV status. In the United States and high risk populations HSV-2 is more widely spread and may not be limited to those whose earlier histories put them at risk of HSV-1. Positive associations between the viruses when detected are not strong indicating that any correlation between risk behaviours or innate susceptibility is not strong. At the population level confounding variables could hide a negative association at the individual level. The problems of confounding are enhanced by combining many studies of varying quality in a meta-analysis.
Some variables identified as potentially confounding could actually be effect modifiers. For example, in a recent trial of a vaccine against HSV-2 it was found that previous infection with HSV-1 conferred protection against symptoms of subsequent genital HSV-2 infection among women rather than men.11 A protective effect for HSV-1 infection may also depend on the route of acquisition of HSV-1 and HSV-2 infection, since the immune response could be concentrated at the site of initial infection.31
Our study illustrates some of the difficulties of applying the methods of systematic review and meta-analysis away from clinical trials where uniform standards of study design are expected. In observational studies there can be great heterogeneity between study populations as detected here. For example, the populations categorised as “low risk” included non-institutionalised civilians, pregnant women, hospital patients and blood donors, while study populations which were categorised as “high risk” included STD clinic attendees, commercial sex workers, HIV positive homosexual men, HIV negative homosexual men, and HIV negative women demographically matched to HIV positive women. The three largest samples (one a control group) were all from the United States and were all categorised as samples from “low risk” study populations.32–34 Two of these studies showed that HSV-1 infection was significantly associated with decreased odds of HSV-2 infection while, conversely, the third showed that HSV-1 infection was significantly associated with increased odds. The samples associated with a protective effect were composed solely of pregnant women from Washington State,33,34 while the third was a national sample of non-institutionalised civilians aged over 12 years.32 There is likely to have been a large degree of confounding of the association between HSV-1 and HSV-2 infection in the third sample, because of the very broad nature of the study population. However, while the more closely controlled studies in Washington may provide more convincing cross sectional data, the cohort study derived from one of them failed to demonstrate a protective effect.34 Methods can also make comparisons difficult. For instance, different studies used different assays for HSV-1 and HSV-2 antibodies, which may have differed in their specificity and sensitivity.35 In the cohort studies the length of follow up and degree of exposure to HSV-2 differed between the studies which may have generated differences in the individual effects between these studies.
This systematic review of epidemiological data shows the inherent difficulties in testing hypotheses about the interaction between two viral types. Future studies require very careful designs to measure confounding variables and identify the site and sequence of infections. The current findings indicate that no interaction between the viruses is most likely, but that analyses should explore the sensitivity of results to a range of assumptions. The trend towards a protective effect found from combining unadjusted risk ratios from prospective studies is interesting and should be given more weight than the result from cross sectional studies because of the importance of the temporal sequence of infection in any association between HSV-1 and HSV-2. A stronger protective effect may be detectable in a prospective study of HSV-2 incidence in those of known HSV-1 serostatus, if other behavioural risk factors are controlled for, or in odds ratios from cross sectional studies where risk factors are accurately controlled for. The interaction between HSV-1 and HSV-2 infection is important in models of the impact of interventions, particularly when HSV-1 has a direct impact on the intervention as appears the case with the candidate HSV-2 vaccine.
Key messages
-
Combining data from cross sectional studies shows a positive association between HSV-1 and HSV-2 infection. However, this association is likely to be erroneous because of confounding
-
Conversely, combining data from prospective studies show a trend towards a protective effect for previous HSV-1 infection against infection with HSV-2
-
The relation between HSV-1 and HSV-2 infection is not clearcut with large interstudy variation
Two international seroprevalence studies have been published since the review was carried out. The first analysed samples from selected populations in Brazil, Estonia, India, Morocco, and Sri Lanka.36 The second analysed samples from general populations in eight European countries.37 Both studies found a trend towards increasing HSV-1 and HSV-2 infection with age, and higher rates of HSV-2 infection among women than men. The first study found significantly higher odds of HSV-2 infection among those HSV-1 seropositive compared to those HSV-1 seronegative. A positive association between HSV-1 antibodies and HSV-2 antibody status was also found for four countries in the European study, which did not remain after adjustment for age and sex. These studies were not included in our graphs and meta-analysis since they were published after the literature search was carried out and were therefore not part of the systematic review.
Acknowledgments
We thank GlaxoSmithKline for research support and MJ Cannon (Centres for Disease Control and Prevention, Atlanta, USA), A Fontanet (Institut Pasteur, France), M Howard (McMaster University, Canada), HF Rabenau (Johann Wolfgang Goethe University of Frankfurt am Main, Germany), L-G Robinson (Harlem Hospital Center, New York, USA) and P Wutzler (Friedrich-Schiller University of Jena, Germany) for providing additional data.
CONTRIBUTORS KJL carried out the review and statistical analysis and GPG helped with study design and interpretation; the manuscript was written by KJL and redrafted by GPG; GPG and KJL were jointly responsible for the manuscript revision.
REFERENCES
Supplementary materials
The tables, figures and references are available as downloadable PDFs (printer friendly files).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - Table 1. HSV-1 and HSV2 seroprevalence by age published since 2002
- [view PDF] - Table 2. Coincidence of HSV-1 and HSV-2 infection by age
- [view PDF] - Figure A. Age-specific seroprevalence of HSV-1 and HSV-2 in �low-risk� and �high-risk� populations in Europe.
- [view PDF] - Figure B. Age-specific seroprevalence of HSV-1 and HSV-2 in �low-risk� and �high-risk� populations in the USA.
- [view PDF] - Table references
Footnotes
-
Conflicts of interest: GPG is a consultant for GlaxoSmithKline. GPG and KJL both receive funding from GSK.