Article Text

Abstract
Context Limited information is available of effects of rural-to-urban within-country migration on cardiovascular (CV) risk factors in low- and middle- income countries (LMIC).
Objective A systematic review of studies evaluating these effects was performed with rural and/or urban control groups.
Study selection Two teams of investigators searched observational studies in Medline, Web of Science and Scopus until May 2011. Studies evaluating international migration were excluded.
Data extraction Three investigators extracted the information stratified by gender. Information on 17 known CV risk factors was obtained.
Results Eighteen studies (n=58 536) were included. Studies were highly heterogeneous with respect to study design, migrant sampling frame, migrant urban exposure and reported CV risk factors. In migrants, commonly reported CV risk factors—systolic and diastolic blood pressure, body mass index, obesity, total cholesterol and low-density lipoprotein—were usually higher or more common than in the rural group and usually lower or less common than in the urban group. This gradient was usually present in both genders. Anthropometric (waist-to-hip ratio, hip/waist circumference, triceps skinfolds) and metabolic (fasting glucose/insulin, insulin resistance) risk factors usually followed the same gradient, but conclusions were weak as information was insufficient. Hypertension, high-density lipoprotein, fibrinogen and C-reactive protein did not follow any pattern.
Conclusions In LMIC, most but not all, CV risk factors are higher or more common in migrants than in rural groups but lower or less common than in urban groups. Such gradients may or may not be associated with differential CV events and long-term evaluations are necessary.
- Emigration and immigration
- cardiovascular system
- risk factors
- income
- meta-analysis as topic
- EBM
- epidemiology
- risk stratification
- growth factors, endothelial function
- hypertension
- HIV
- smoking
- public health
- clinical trials
- metabolic syndrome
Statistics from Altmetric.com
- Emigration and immigration
- cardiovascular system
- risk factors
- income
- meta-analysis as topic
- EBM
- epidemiology
- risk stratification
- growth factors, endothelial function
- hypertension
- HIV
- smoking
- public health
- clinical trials
- metabolic syndrome
Introduction
Non-communicable diseases (NCDs) kill people mostly in low- and middle-income countries (LMIC).1 The Grand Challenges report highlights the need to study the impact of poverty and urbanisation on NCDs.2 Urbanisation is occurring at a fast rate in LMIC, which may be associated with less physical activity, poorer nutritional habits and rapidly growing prevalence of cardiovascular (CV) risk factors, CV disease (CVD) and other NCDs.3 Rural-to-urban migration is one of the key larger drivers of urbanisation in LMIC. Thus, the evaluation of the impact of rural-to-urban migration on CV risk factors is relevant owing to its huge public health consequences.
The effect of international migration to developed countries on CV risk factors and CVD has been systematically studied.4 As a result of the unique pattern and rate at which migration is occurring within LMIC, international migration results cannot be inferred from these settings. In LMIC, differences in design and patient characteristics make it difficult to reach a definitive conclusion on the effects on CV risk factors.5–9 Also, it is not known whether the effect of rural-to-urban migration is uniform across CV risk factors and across LMIC. Finally, the effect on emerging CV risk factors such as fibrinogen, homeostasis model assessment (HOMA) insulin resistance, or C-reactive protein could also be evaluated in the most recent studies.
We conducted a systematic review of observational studies evaluating the effect of rural-to-urban within-country migration on CV risk factors in LMIC. We hypothesised that migrants would have a worse CV risk profile than rural individuals and better CV risk profile than urban individuals.
Methods
Study selection
A comprehensive literature search using PubMed-Medline, The Web of Science and Scopus until 31 May 2011 was conducted. The following keywords were used: migration, emigration, immigration, residential mobility, transient and migrants, rural population, urban population, CV risk factors and cardiovascular disease. The search strategy of PubMed is available in the appendix (web only). We searched observational studies published in any language, performed in LMIC as defined by the World Bank.10 We excluded studies of international migration or those from high-income countries. A formal protocol was developed for this project.
Rural-to-urban migration was defined as the individual's self-report or objective information of birth in a rural setting and, at the time of the study, self-report or objective ascertainment of urban residence. Three types of control groups were possible: (a) a rural comparison group, where migrants originated from the same area; (b) an urban comparison group, where migrants shared the same urban environment and (c) both a rural and an urban comparison group. This strategy excluded studies focusing only on differences between rural and urban settings. Sampling frames for migrants were classified as: (i) random sample of migrants from an urban population; (ii) cohort of people born in a rural area who moved to an urban area and were traced; (iii) rural individuals selected and their family members followed up in urban area (sib pair) and (iv) population level survey where migration was based on a retrospective question (“Were you born here?”).
A list of retrieved articles was reviewed independently by two groups of investigators based in USA and Peru in order to choose potentially relevant articles, and disagreements were discussed and resolved. When multiple articles for a single study had been published, we used the most relevant publication and supplemented it, if necessary, with data from the other publications.
Data extraction
Data extraction was performed independently by three investigators (AVH, VP, AD). Disagreement was resolved by consensus. Using a standardised data extraction form, we collected information on lead author, year of study or publication year, study design, sample size, sampling frames for migrants, length of urban exposure, age of migration, average age, percentage of male participants and 17 CV risk factors for migrants and control groups.
Outcomes
CV risk factors we collected were systolic blood pressure (SBP), diastolic blood pressure (DBP), hypertension; total cholesterol (TC), low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol; body mass index (BMI), obesity; triceps skinfolds thickness, waist circumference, hip circumference, waist-to-hip ratio (WHR); fibrinogen, C-reactive protein (CRP); fasting glucose, fasting insulin and HOMA scores, a validated measure of insulin resistance. Extracted information was stratified by gender. For repeated measures, information extracted corresponded to the longest follow-up.
Study quality assessment
The order of quality of studies was considered as follows: (1) prospective cohort study; (2) retrospective cohort study; (3) case–control study and (4) cross-sectional study. Also, we systematically assessed other key points of study quality proposed by the MOOSE collaboration.11 These key points were (1) clear identification of the study population; (2) clear definition of outcome and outcome assessment; (3) independent assessment of outcome parameters (ie, ascertainment of outcomes done by researchers other than those involved in the study); (4) selective loss during follow-up and (5) important confounders and/or prognostic factors identified. Each point was rated as ‘yes/no’. If the description was unclear, we considered this as ‘no’.
Statistical analysis
Our systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.12 Differences between migrants and either rural or urban control groups are shown as absolute differences (ie, migrant minus control) and their 95% CIs for both continuous and categorical CV risk factors. Non-normally distributed risk factors were described in some studies as geometric means and we extracted them as published.
A high degree of heterogeneity among studies was expected and therefore we did not combine all studies in a formal meta-analysis. Taking into account the sources of heterogeneity, three subgroup meta-analyses were prespecified: (1) studies with similar characteristics, including cross sectional design, random sampling frame and >5 years of urban exposure; (2) cross-sectional studies and (3) studies published after 1990. Subgroup meta-analyses were stratified by gender, as differences were expected between genders.
DerSimonian and Laird random effects models were used for meta-analyses.13 For dichotomous CV risk factors, we used the Mantel–Haenzel method to calculate pooled ORs and 95% CIs. For continuous CV risk factors, we used the inverse variance method to calculate mean differences (MDs) and 95% CIs. Statistical heterogeneity was evaluated with the Cochran χ2 and the I2 statistics. Funnel plots were used to evaluate publication bias for the meta-analyses. All analyses were stratified by gender. We used Review Manager (RevMan 5.0, Oxford, UK; The Cochrane Collaboration, 2008).
Results
Study characteristics
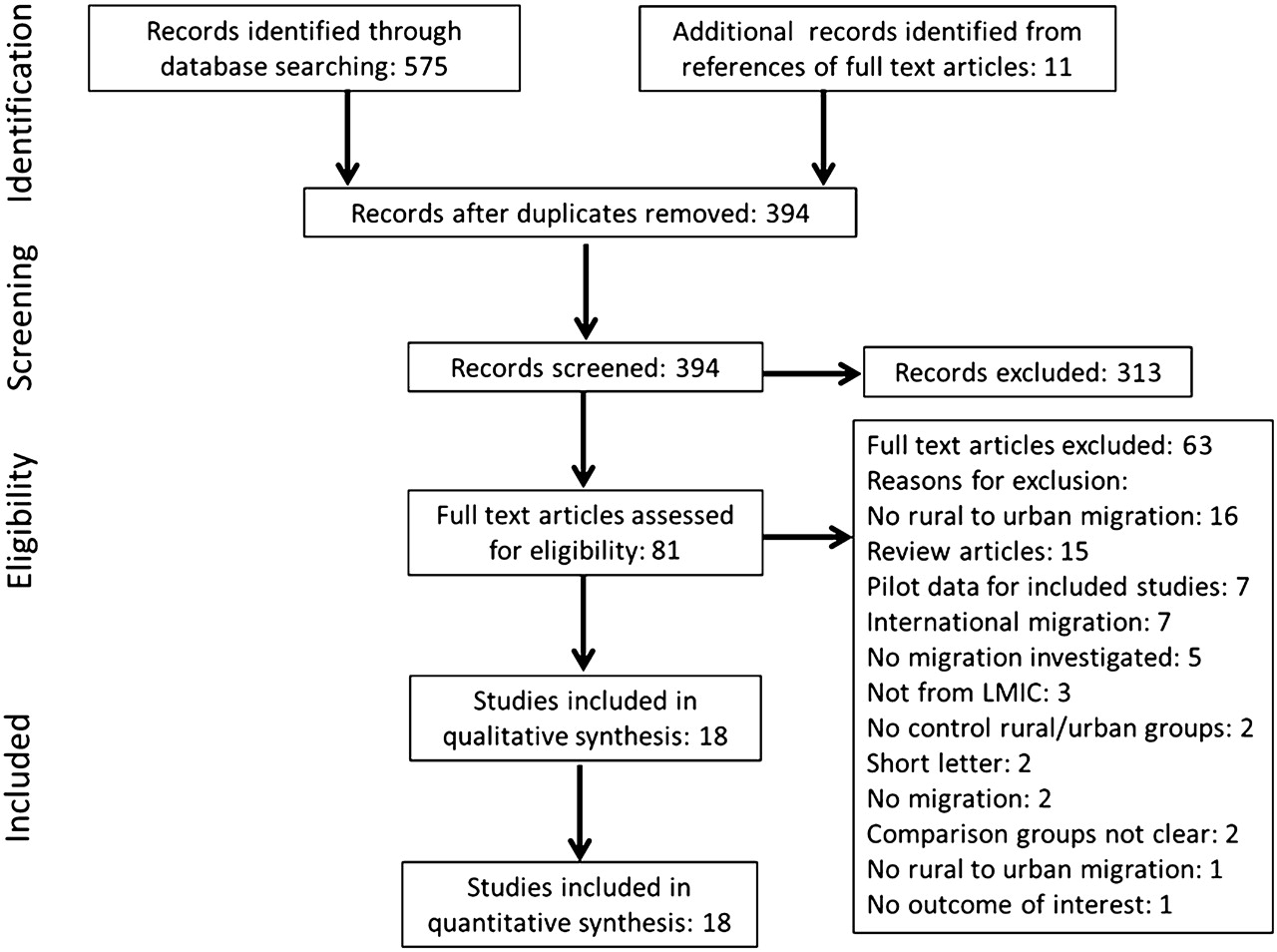
A total of 394 citations were identified and screened, of which 81 were retrieved for detailed assessment. Of these, 63 did not fit our criteria (figure 1). Thus, 18 studies were chosen in the qualitative synthesis,5–9 14–26 including 58 536 individuals (table 1). Studies included mostly adults, with very few individuals aged <15 years.
{kind=link}
Search strategy profile of the systematic review.
Characteristics of studies included in the systematic review
Fourteen studies were cross-sectional, one was a retrospective cohort26 and three were prospective cohorts.7 17 23 Studies were heterogeneous with respect to several characteristics. These studies were reported between 1964 and 2011. Fifteen studies compared the migrant group to the rural control group and nine studies reported the years of urban exposure for the migrant group (urban exposure ≥6 months and mostly >5 years). Sampling frames for migrants were also heterogeneous: random sampling in eight studies, a traced cohort in six studies, a population survey in three studies and a sib-pair strategy in one study.
All studies clearly identified the study population and defined the outcome and outcome assessment (online supplementary table 1w). None of studies independently assessed the outcomes and four studies had a selective loss of patients during follow-up.7 17 23 26 Six studies identified important confounders or prognostic factors6 8 9 18 25 26 and adjusted the association between migration and the CV risk factors.
The most commonly reported CV risk factors were SBP (13 studies), DBP (13 studies), hypertension (11 studies), BMI (11 studies), obesity (four studies), TC (six studies), LDL (five studies) and HDL (four studies). Hypertension was defined as BP ≥140/90 in only six studies, all of them published after 1990. Other CV risk factors including WHR, waist and hip circumference, triceps skinfolds, fasting glucose and insulin, HOMA scores, fibrinogen and CRP, were reported by fewer studies.
Effect of rural-to-urban migration on commonly reported CV risk factors
In most of the studies, values or rates in migrants were higher than in the rural group and lower than in the urban group. Nine out of 12 studies showed higher SBP levels in migrants than in the rural group (range 0.9 to 11.9 mm Hg, significant differences in seven) and five out of six studies shower lower SBP in migrants than in the urban group (range −0.2 to −8.3 mm Hg, significant differences in two) (table 2). Ten out of 12 studies reported higher DBP in migrants versus rural (range 1.5 to 13.9 mm Hg, significant differences in nine) and three out of five studies showed lower DBP in migrants versus urban (range −1.2 to −4.9 mm Hg, significant differences in two) (table 3). Eight out of nine studies showed higher hypertension rates for migrants versus rural (range 2.3% to 25.3%, significant differences in five) and two out of four studies reported non-significantly lower hypertension rates for migrants versus urban (range −0.7% to −16.6%) (table 2w, web only).
Systolic blood pressure (SBP) in mm Hg for the migrant, rural and urban groups
Diastolic blood pressure (DBP) in mm Hg for the migrant, rural and urban groups
Nine out of 10 studies reported higher BMI values in migrants versus rural (range 0.2 to 3.8 kg/m2, significant differences in six) and all of the four studies showed significantly lower BMI values in migrants versus urban (range −0.3 to −1.3 kg/m2) (table 4). Two studies showed higher obesity rates in migrants versus rural (range 0.2% to 18.1%, one with significant difference) and two studies showed significantly lower obesity rates in migrant versus urban (range −3.9% to −13.1%) (table 3w, web only).
Body mass index (BMI) in kg/m2 for the migrant, rural and urban groups
All five studies showed higher TC levels in migrants versus rural (range 4.0 to 35.1 mg/dl, significant differences in four); all of the three studies showed non-significantly lower TC levels in migrants versus urban (range −1.9 to −4.1 mg/dl) (table 4w, web only). Three out of four studies reported significantly higher LDL levels in migrants versus rural (range 5.3 to 30.3 mg/dl); two out of three studies reported non-significantly lower LDL levels in migrants versus urban (range −1.0 to −3.9 mg/dl) (table 5w, web only). Finally, two out of three studies showed lower HDL levels in migrants versus rural (range −0.1 to −1.8 mg/dl, one significant difference); one out of two studies showed lower HDL levels in migrants versus urban (absolute difference 1.2 mg/dl) (table 6w, web only).
Effect of rural-to-urban migration on uncommonly reported CV risk factors
In two studies8 9 WHR values in migrants were significantly higher than in the rural and urban (range 0.01 to 0.06 and −0.01, respectively). Three studies7 9 20 showed larger waist circumference levels in migrants versus rural (range 0.6 to 12.0 cm, significant differences in two); one study9 showed shorter waist circumferences in migrants versus urban (difference −3.3 cm, 95% CI −1.4 to −5.2). In one study,9 a significantly larger hip circumference was shown in migrants versus rural (difference 7.0 cm, 95% CI 6.1 to 8.0) and significantly shorter hip circumference in migrants versus urban (difference −4.5 cm, 95% CI −2.9 to −6.1). Two studies9 16 showed larger triceps skinfold thickness in migrants versus rural (range 0.1 to 10.9 mm, one significant difference); one study reported significantly shorter triceps skinfolds thickness in migrants versus urban (difference −8.9 mm, 95% CI −5.5 to −12.3).
Two out of three studies7 9 20 reported higher mean or geometric mean glucose values in migrants versus rural; two studies9 24 reported lower mean or geometric mean glucose values in migrants versus urban. Three studies8 9 20 showed higher mean or geometric mean fasting insulin levels in migrants versus rural; two of the studies8 9 also showed lower fasting insulin levels in migrants versus urban. The mean or geometric means of HOMA scores were significantly higher in migrants versus rural in two studies9 20; in one study9 the geometric mean of the HOMA score was significantly lower in migrants versus urban. Geometric means of fibrinogen and CRP in migrants were significantly higher versus rural and similar to the values in urban groups.9
The observed gradient for most of the commonly and uncommonly reported CV risk factors among migrants, rural and urban groups was found in both men and women separately.
Meta-analyses in subgroups of studies
Owing to limited availability of CV risk factors, we only included SBP, DBP and BMI in these meta-analyses. Substantial heterogeneity of effects among studies and no evidence of publication bias were seen in all three sets of meta-analyses.
Five studies6 9 20–22 fulfilled our first prespecified criteria of being cross-sectional studies, with a random sampling frame for migrants and with at least 5 years of urban exposure for migrants. No differences were found between migrants and rural individuals for SBP, DBP or BMI. A pattern of significantly lower SBP (MD −3.5 mm Hg, 95% CI −5.6 to −1.4) and lower DBP (MD −3.0 mm Hg, 95% CI −4.2 to −1.72) in migrants versus urban was seen overall and for both men and women.
Fourteen studies were cross-sectional (table 1) fulfilling our second prespecified criterion and 13 studies were published after 1990 (table 1) fulfilling our third criterion. Gradients were similar to the overall results for SBP, DBP and BMI in these subgroups.
Discussion
Main findings
Studies conducted in LMIC evaluating the effect of within-country migration on CV risk factors showed substantial heterogeneity in design, sample size, time of urban exposure, migrant sampling frame and reported CV risk factors between migrants and rural or urban individuals. In general, when observing the absolute differences between migrants and comparison groups, a gradient for most of the commonly reported CV risk factors was noted: higher values or rates in migrants than in rural individuals and lower values or rates in migrants than in urban individuals. This gradient was also seen in most of the studies when evaluating men and women separately. Nevertheless, against our hypothesis, some CV risk factors such as hypertension rates, HDL, fibrinogen and CRP levels did not follow any gradient.
What the current literature reports
The effect of international migration to developed countries on CV risk factors has been systematically studied by McKay et al.4 These migrants are exposed to increased consumption of saturated fats and sugars and sedentary behaviour and also to stressful life conditions. International migrants have poorer health and a worse CV risk factor profile than non-migrants and this profile may worsen with increasing duration of stay in the urban environment.
Rural-to-urban within-country migration is a common phenomenon in LMIC countries,5 largely owing to economic reasons. Its effects on CV risk factors have been poorly studied26; blood pressure/hypertension and BMI/obesity have been mostly examined. Even less information is available for lipid profiles27 or emerging and newer CV risk factors (eg, CRP, fasting insulin, HOMA scores, fibrinogen).9
In LMIC, urban–rural comparisons are of limited relevance in examining the effects of urban migration as the urbanisation process in these countries occurs owing to growth of existing urban populations, expansion of urban boundaries and rural-to-urban migration.28 Also particular genetic, cultural and lifestyle backgrounds of migrants and urban individuals further limit the value of urban–rural comparisons. However, several urban–rural comparisons of CV risk factors have been published. Comparisons of urban and rural areas in sub-Saharan Africa29 and India30 showed higher rates of hypertension, obesity and adverse lipid profiles for urban individuals; however, no differences between urban and rural areas for these risk factors have lately been found in China.31
What our study adds to current literature
We hypothesised that there would be a gradient with worse CV profile for urban individuals than for migrants and worse for migrants than for rural individuals. This was the case for most of the CV risk factors; in most cases reported differences were significant. Some CV risk factors such as hypertension rates, HDL, fibrinogen and CRP levels did not follow any gradient. It seems implausible that these CV risk factors are not modified by migration, given significant modifications of major risk factors, but recent reports, at least for blood pressure levels, suggest that the patterns of change after migration are complex and do not necessarily follow the expected gradient.23 32 An alternative explanation may include the scarcity of studies. Our chosen studies did not evaluate the effect of modified CV risk factors on CV events and the gradients may or may not be associated with differential CV events across groups in the future. Thus, long-term longitudinal evaluations are necessary.
The gradient urban–migrant–rural for most CV risk factors seems relevant in studies with substantial heterogeneity. Recognising the sources of heterogeneity, we secondarily analysed three subgroups of studies. Cross-sectional and after-1990 subgroups of studies showed similar gradients between urban, migrant and rural to those seen in all studies. The subgroup of cross-sectional studies with random sampling of migrants and at least 5 years of urban exposure for migrants showed lower SBP and DBP for migrants than for urban individuals and non-significant differences between migrants and rural individuals. Although subgroup results should be taken with caution as heterogeneity of effects remained significant in all three subgroups of studies, they may highlight potential changes of gradient with longer urban exposure of migrants.
There was a considerable paucity of information on other important anthropometric risk factors (eg, WHR, hip circumference, triceps skinfold thickness) or metabolic and inflammation risk factors (eg, glucose, fasting insulin, insulin resistance scores, fibrinogen, CRP). Our conclusions for these infrequently reported risk factors are weak and require further re-evaluation.
Only six studies6 8 9 18 25 26 provided adjusted values of CV risk factors or adjusted estimates of the differences between migrants and controls. Adjusters included age, BMI, gender, socioeconomic status, education, occupation, marital status, physical activity, initial health status and altitude. Most of these studies were published between 2009 and 2011, with the exception of the Yi Migrant6 and Yi People18 studies. Our main and secondary analyses were based on unadjusted values of CV risk factors and therefore some bias may be present in our association measures between migration groups. Combination of adjusted metrics was not possible given the different sets of confounders adjusted for, the heterogeneity of studies and the limited number of studies.
Limitations
First, we included studies that were heterogeneous with respect to several characteristics and therefore a meta-analysis of all studies was not possible. Prespecified subgroups of more homogeneous studies also showed significant heterogeneity and subgroup results should be taken with caution. Second, we evaluated unadjusted differences between groups, as only unadjusted values were published by authors for most of the studies. Few recent studies provided adjusted values for a few of the CV risk factors we used in our analyses. Third, publication bias is always a concern in a systematic review; however, we decreased this in our study by having no language restrictions, by using a comprehensive study search strategy in four literature engines and by involving two groups of investigators with at least two researchers in each group. Fourth, we expect some differences on the effect of within-country migration on CV risk factors across different countries and continents. We could not explore this hypothesis given the small number of studies available. Finally, the scarcity of reporting of several metabolic and inflammatory risk factors did not allow stronger conclusions to be reached of the effect of migration on them.
Conclusions
Studies investigating the effect of rural-to-urban within-country migration on CV risk factors in LMIC are highly heterogeneous. Most CV risk factors in migrants follow a gradient: higher or more common than in the rural groups and lower or less common than in the urban groups. Furthermore, some CV risk factors, such as hypertension rates, HDL, fibrinogen and CRP levels did not follow a pattern. Such gradients may or may not be associated with differential CV events across groups, and long-term longitudinal evaluations of such associations remain necessary.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
Funding The CRONICAS Center of Excellence in Chronic Diseases at UPCH is funded by the National Heart, Lung and Blood Institute (NHLBI), under contract No. HHSN268200900033C. The funders had no role in study design; data collection, analysis, or interpretation; in writing the report, or in the decision to submit the article for publication. The researchers are all independent from the funding source.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.