Article Text

Abstract
The healthcare sector stands to benefit most from frugal innovation, the idea that more can be done for less for many more people, globally. As a first step for health systems to leverage new approaches to offset escalating health expenditures and to improve health outcomes, the most relevant frugal innovations have to be found. The Institute of Global Health Innovation was commissioned by the US-based Commonwealth Fund to identify frugal innovations from around the world that could, if transferred to the USA, offer approaches for expanding access to care and dramatically lower costs. Our global scan was motivated by the need to extend the list of frugal innovations in healthcare beyond the impressive but oft-repeated examples such as GE’s MAC 400, a US$800 portable ECG machine, Narayana’s US$1500 cardiac surgery and Aravind’s US$30 cataract surgery. Our search involved (1) scanning innovation databases, (2) refining frameworks to identify frugal innovations and evaluate their reverse potential and (3) developing in-depth case studies. From 520 possible innovations, we shortlisted 16 frugal innovations that we considered as frugal and with potential for reverse diffusion into high-income country health systems. Our global search was narrowed down to three care delivery models for case analysis: The Brazilian Family Health Strategy around community health workers; Singapore-based GeriCare@North use of telemedicine and Brazil’s Saude Crianca community involvement and citizenship programme. We share core features of the three frugal innovations and outline lessons for practitioners, scholars and policymakers seeking to lower healthcare costs while increasing access and quality.
Statistics from Altmetric.com
Introduction
The healthcare sector stands to benefit most from frugal innovation, the idea that more can be done for less for many more people, globally. Our study coincided, though independently, with the BMJ Innovations launch in 2015 and promise that ‘frugal medical technologies are poised to disrupt the healthcare economy and will hopefully meet the unmet clinical needs of the world’.1 We see frugal innovations as products, processes or policies that leverage means and ends to do more with less for many and therefore have potential to increase value and provision of healthcare. Such innovations have traditionally been associated with low-income and middle-income countries or emerging markets,2 3 but are increasingly being found everywhere and explored for global use, as reverse innovations that flow from low-income to high-income settings.4 In healthcare particularly, unsustainable growth in healthcare expenditure is forcing global healthcare systems to learn from affordable technologies and models.5 6
Increasing healthcare costs are contributing to unsustainable spending globally, but most crucially in the USA and the UK. The US Centers for Medicare and Medicaid Services forecasts the National Healthcare Expenditure in 2017 will be more than US$3.5 trillion (approx $10K per capita), increasing by 5.4% from the previous year. The UK NHS Confederation estimates health expenditure for 2017-8 could be £124 billion (US$164 billion; approx £2K or $2.7K per capita), increasing by 3.3% from the previous year. Although in many Organisation for Economic Co-operation and Development (OECD) countries, healthcare costs are growing faster than gross domestic product, the positive news is that attention is being afforded to bending the growth cost curve.7 The US Department of Health and Human Services claims that since the Affordable Care Act became law, healthcare prices have risen at the lowest rate in 50 years. And the UK NHS Five-Year Forward View is aiming for £22 billion (US$35 billion) in savings by 2020.
As part of The Imperial College London and Lancet Commission in August 2012, some of our co-authors called for the development of ‘frugal technologies’—cost-effective technologies that are developed to cope in local conditions.8 In more than four years since, we find frugality is much more complicated than just affordability, that the source and relevance of frugal models in healthcare are not limited to low-income or middle-income countries and that the pace of global adoption of frugal innovations is lagging behind universal need. Many perspectives have been debated about frugal innovation or technologies in business and strategy with one key lesson: frugality is not simply about cost. Frugality is about affordability, but in moving beyond early perspectives of frugal innovations as simply ‘good-enough’ or ‘no-frills’ products, we must recognise frugality or affordability is also about adaptability and accessibility.9 10 Adaptability in healthcare encompasses ‘fit’ for use in the local and clinical setting and accessibility in healthcare relates to universal coverage and scale. Our assessment identified innovations as frugal based on these three key constructs, that is, affordability, adaptability and accessibility.
As a first step for health systems to leverage, according to the Commonwealth Fund, ‘approaches for expanding access to care and dramatically lower costs’, the most relevant innovations have to be found. The next step is to diffuse the innovations. Our global scan and research of frugal innovations, and their potential as reverse innovations, was commissioned by the Commonwealth Fund and was motivated by the need to extend the list of frugal innovations in healthcare beyond the eye-catching and oft-repeated examples such as Narayana’s US$1500 cardiac surgery,11 Aravind’s US$30 cataract surgery12 and General Electric’s US$800 MAC 400 portable ECG machine.13 Narayana Health took on the technical challenge to decrease the cost of one of the most expensive surgeries in the world, cardiac bypass, to approximately US$1500 per operation versus US$144 000 in the USA, US$27 000 in Mexico and US$14 800 in Colombia, while at the same time, upholding quality. Its patients enjoy a 1.3% 30-day mortality from coronary artery bypass surgery versus an average of 1.9% in the US in 2008.11 Aravind’s social mission is to provide ‘sight for all and to see everyone as one’ by providing cataract surgeries to millions at a cost of as little as US$30 per patient in 2013, compared with around US$3000 for a similar procedure in the USA. The hospital’s Aurolab pioneered the production of high-quality, US$5 low-cost intraocular lenses producing 700 000 lenses a year, of which three-quarters are exported all over the world.12 General Electric’s handheld MAC 400 was originally developed for the rural Indian healthcare market and miniaturises a sophisticated ECG machine to be easily transportable and useable by healthcare workers at a fraction of the cost when compared with high-end machines costing as much as 10 times more and only available for use in hospitals by highly trained healthcare professionals.13
We implemented our search strategy to find and evaluate hundreds of less well-known innovations with similar potential from unlikely places, such as, but not limited to, low-income and middle-income countries or social entrepreneurs.10 14 Detailed findings were showcased at the Commonwealth Fund 2015 International Symposium on Healthcare Policy in Washington DC to a global panel of health ministers and policymakers with the aim to offset the unsustainable growth in health expenditures and to improve health outcomes. We share lessons from the global frugal innovations in healthcare we shortlisted and suggest measures for practitioners, scholars and policymakers to help leverage new models in innovation for affordable, adaptable and accessible healthcare globally.
Methods
An exploratory and non-experimental descriptive mixed methods research design was chosen15 using a combination of quantitative and qualitative data analysis approaches to search for, assess and analyse innovations.
Between February and March 2015, we carried out desk research, literature review and online survey of 50 global leaders drawn from the Institute of Global Health Innovation (IGHI) network to identify potential sources of relevant innovations. We landed across several ‘innovation curator’ organisations. These organisations search out and collate healthcare innovations to provide usually publicly accessible information to healthcare professionals who are seeking new policies, products or practices to improve the quality of their work.16 We identified nine global databases (see figure 1) of which the most comprehensive resource was the non-profit US based Center for Health Market Innovations (CHMI), which has been used in several prior studies of innovations.17 18 After we had catalogued thousands of innovations listed in the innovation databases, we focused on 520 which had data we deemed to be sufficient for evaluation. We systematically evaluated and shortlisted the hundreds into 85 found to match our frugal identification criteria. In prior work, we attained an inter-rater agreement in excess of 70% in using our frugal assessment tool (see Prime et al19 for further information). Between April and May 2015, we then tested, revised and applied a reverse innovation assessment tool from the Toronto Health Organization Performance Evaluation (T-Hope) group,20 to settle on 27 cases that were both frugal and had potential to be transferred to the USA, which we deemed to have the greatest relevance and potential to be diffused into the US healthcare market. Criteria included need, novelty, receptivity and compatibility with regulation and infrastructure. Pairs of assessors performed independent evaluations using the innovation descriptions on innovation databases sources, as well as information from the specific innovation websites and any relevant innovation-related publications. Between May and June 2015, a panel of five health policy experts from the IGHI network, who have experience or deep understanding of the US healthcare system, was convened with the IGHI team to assess the 27 shortlisted innovations. The panel identified 16 innovations for presentation to the Commonwealth Fund. The Fund then held internal advisory feedback that led to a shortlist of three. Between July and September 2015, we collected and collated evidence on these three cases through desk-based research, fieldwork, site visits to Brazil and Singapore and analysis of interviews and document analysis. Two researchers travelled to home contexts in different cities and villages and spent around a week on each case to conduct between 10 and 12 interviews of stakeholders representing founders, policy leaders, managers and frontline health staff. Between September and October 2015, we developed 3–4000 word cases for the adoption of these innovations into the USA. Development of the case studies was based on triangulation of several sources of data such as review of the primary and secondary data on the innovations and detailed document analysis including financial reports and business cases, as well as field site observations and interviews to facilitate a deeper contextual understanding of the innovations under investigation.

Institute of Global Health Innovation global scan of frugal innovations in healthcare.
Results
Our assessment of 520 innovations from nine innovation databases revealed 85 examples of frugal innovations in healthcare from both low-income and high-income countries. The top ranked 27 innovations with potential for reverse diffusion or translation into the USA were selected for further investigation. From this shortlist, the Commonwealth Fund selected three of the most promising for case study development. The 16 selected innovations are described in table 1.
Sixteen selected innovations
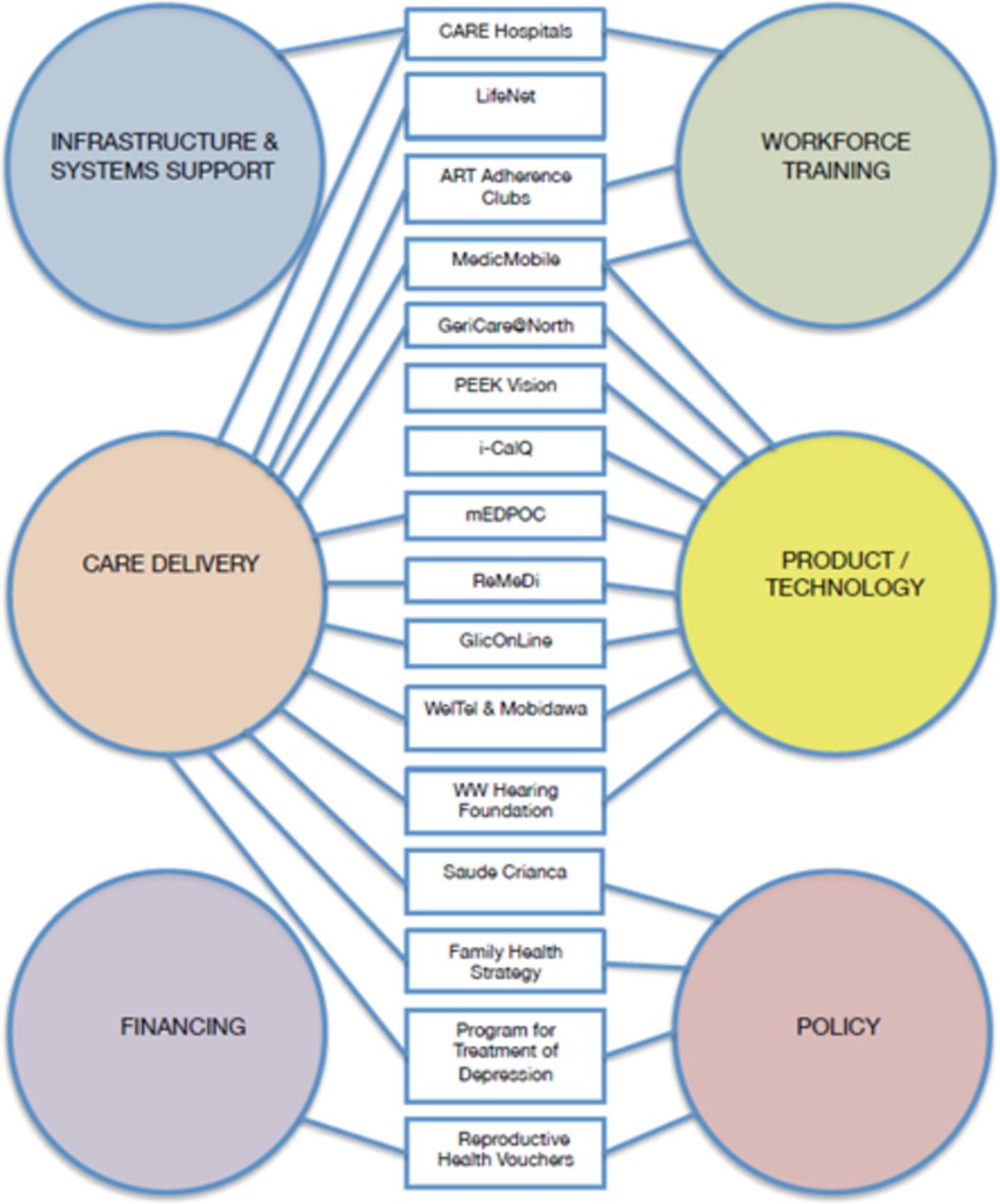
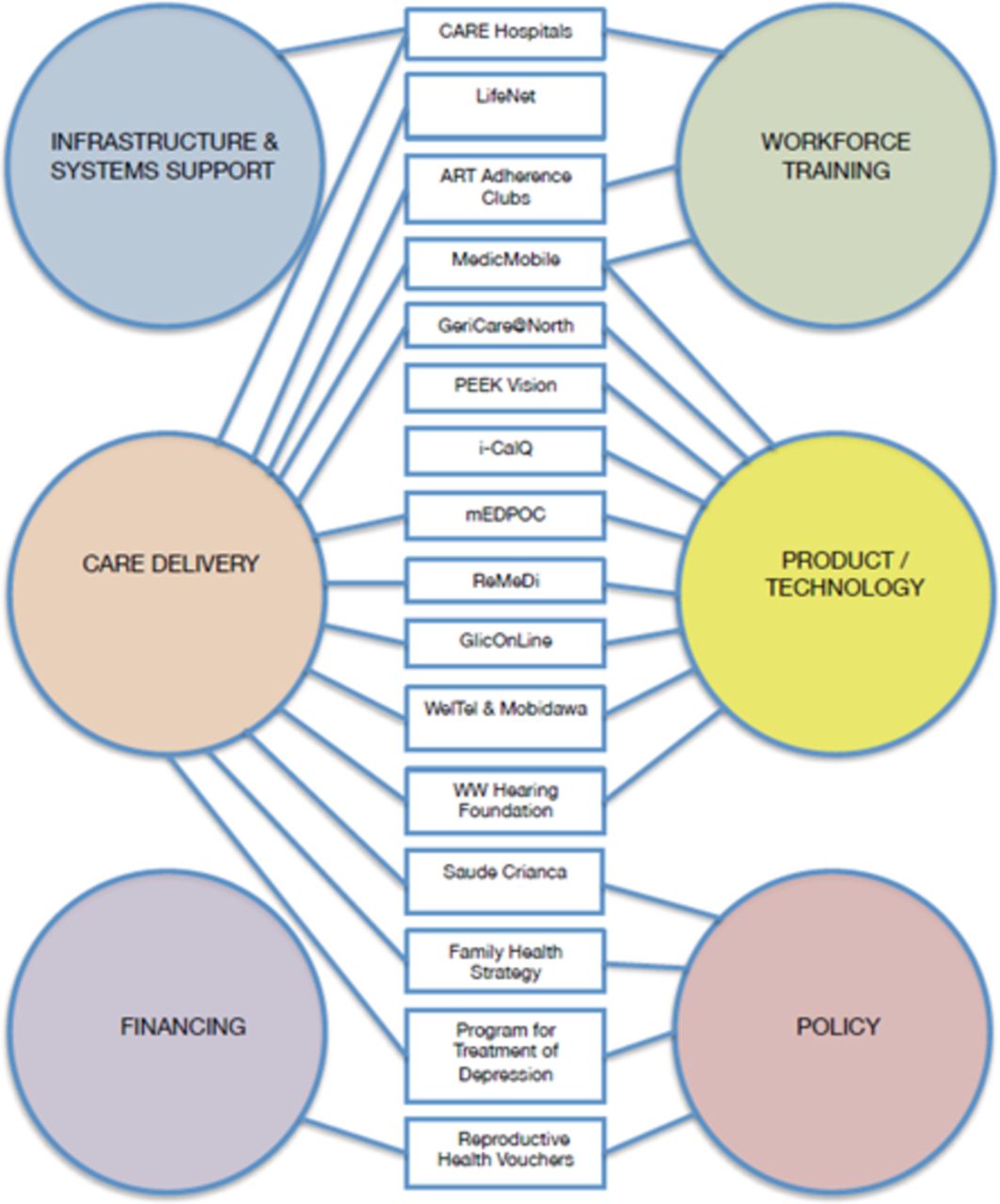
The scanning exercise revealed a wide range of frugal innovations around the world for different applications and contexts. However, many of the innovations had similar objectives, are addressing the same problem, have common operating models, or leverage mobile technologies. We thematically analysed and through consensus grouped the 16 cases into six categories of innovation: care delivery, product or technology, policy, workforce training, infrastructure and system support and financing (figure 2). The most common category was care delivery followed by product or technology. This may be because the Commonwealth Fund had communicated most interest in care delivery models during our expert panel shortlisting phase. The least popular categories were financing and infrastructure and systems support, both of which were supported by one innovation each, Care Hospitals and Reproductive Health Vouchers, respectively. Many innovations composed of multiple ways and means through which better healthcare is offered. Thirteen innovations fit in multiple categories whereas three — Peek Vision (vision tests through smartphone), i-calQ (portable diagnostic laboratory based on smartphone) and LifeNet (healthcare delivery through faith-based partners) fit in one category.
{kind=link}
{kind=link}
Grouping of the 16 innovation categories.
Based on perceived relevance and applicability in the USA context, we visited, studied and drafted the following extensive case studies: (1) Family Health Strategy in Brazil; (2) GeriCare@North in Singapore and (3) Saude Crianca in Brazil.
The Family Health Strategy (FHS) was created in 1994 by the Brazilian Ministry of Health as part of a wider reform to the primary healthcare system. It represents a fundamental change in the healthcare delivery model, from the traditional curative and procedure-centred approach that passively relies on patients coming to hospitals and health centres in times of need, to one that actively reaches out to the population in need of care, through community outreach and home visits. A key feature of the FHS is the extensive deployment and integration of community health workers, of which there were 263 000 in service as of July 2017 in 31 000 Family Health Strategy Teams, covering approximately 67% of the population.21 They provide home-based basic primary care to families and serve as a liaison to rural and tertiary clinics by relaying on-the-ground information back to healthcare teams. In the process, the reliance on home-visits by integrated teams helps to catch issues early and has circumvented reliance on more expensive care providers and reduced hospital bed occupancy. This is an intervention that is relatively cheap and technologically simple and that can be used to extend access to basic and preventative healthcare to a large proportion of the population. In terms of affordability, the strategy marks a shift in the provision of basic healthcare in Brazil, away from higher cost hospitals and health clinics. The programme costs just US$50 per person per annum, in Brazil, and is regarded as extremely cost effective as it helps to provide comprehensive, longitudinal care at the household level, integrated into primary care teams.22 In terms of adaptability, the strategy has proven to be a powerful tool to improve individual and population health outcomes through home-based month-to-month screening and monitoring for preventive care. And in terms of accessibility, the FHS has scaled to over 67% of the population, most of which is lower income.21 Support for community health workers has diffused mostly to less developed settings. See, for instance, the PACK programme that has spread from South Africa to Botswana, Malawi, the Gambia, Mexico and Brazil.23 But it can have much potential for Western settings too. Even in high-income countries, adopting the deployment of CHWs in particularly rural and underserved communities and those where disparities in health are high, could help alleviate capacity constraints of local health systems by addressing a range of health needs, including the prevention and control of chronic diseases.
GeriCare@North’s telemedicine for geriatrics allows medical professionals to provide diagnosis, monitoring and treatment remotely to the elderly using assisted video-link technology between acute hospitals and nursing homes. In Singapore, Khoo Teck Puat Hospital (KTPH), run by the Alexandra Health System, has pioneered the use of tele-geriatrics in collaboration with the St Josephs Nursing Home, a renowned elderly care home. The trial was commissioned and supported by the Agency for Integrated Care, the Ministry of Health’s implementation partner that strives to achieve an integrated healthcare system for Singapore. In terms of affordability, in Singapore, the average cost of a tele-consultation using GeriCare@North’s telemedicine offering is approximately US$106; in comparison, a private patient travelling to the hospital via ambulance and seeing a doctor costs US$140 and the cost per consultation of a doctor travelling to the nursing home is US$193. The system is deemed to reduce cost of individual consultations through improved efficiency, for example, by reducing travel time for doctors, freeing up resources to treat more patients. In terms of adaptability, it enables more timely care and early interventions by training nurses to act as the ‘hands’ of the consultants, reducing unnecessary admissions and visits to acute hospitals, Emergency Departments and outpatient clinics. In terms of accessibility, it improves delivery of care for the elderly and enables elderly to age in place. Consultations take place three times a week, compared with four times a month for physical visits prior to introduction of tele-geriatrics. The innovation was successfully piloted at KTPH and has since been scaled to encompass three other nursing homes in the North health cluster with plans to expand the programme to three more homes. For Western settings, the growth in ageing populations and longer lifespans is increasing burden of visits to multiple specialist doctors due to comorbidity of diabetes, hypertension, and cardiovascular diseases, and other ailments such as dementia. It is expected that there will be one geriatrician for every 379 875 or older Americans in 2030 down from one for every 262 075 or older Americans as of March 2011.24 Remote consultations can increase provision of healthcare to the ageing population via regulated long-term care service providers.
Saúde Criança is a non-profit social enterprise founded in 1991 in Rio de Janeiro to break the cycle in which poverty and illness lead to hospital admission, subsequent readmission and/or death. Saúde Criança espouses a model of healthcare that addresses all factors that contribute to overall well-being. It targets the families of children who have recently been released from public hospitals and creates tailor-made Family Action Plans which aim to lift families out of poverty by treating the root of the problem. Saúde Criança has the potential to reduce the cost of healthcare delivered to low-income families. In terms of affordability, the average cost of the programme incurred by Saúde Criança for each family is US$362 per month and on average US$7200 at the end of the 24-month programme. Hospitalisation duration has fallen from an average of just under 62 days at entry to the programme to less than 9 days on graduation from the programme. With an average cost of hospitalisation of US$500 per day for public hospitals, Saúde Criança’s intervention results in vast savings for both patients and public hospitals. In terms of adaptability, independent evaluations have shown Saúde Criança’s beneficiaries have opportunities for education, housing, citizenship and earning levels that are on par with more affluent families. Research by Georgetown University has shown positive medium-term and long-term impact on the health and quality of life of the families assisted by the Saúde Criança Association.25 In terms of accessibility, Saúde Criança serves lower income families and reaches out to underserved groups having assisted over 50 000 people in Brazil since its inception. For Western settings, SC can better address the complex, multidimensional problem of poverty and self-sustainability of low income families at social risk. New payment models—including bundled payments, shared savings arrangements and penalties for hospital readmissions—can hold providers financially accountable for patient health and provide economic incentives to incorporate social interventions into their approach to care.
Discussion
Current academic literature touts the potential of frugal innovations in healthcare for low-income, middle-income and high-income countries such as with Narayana Healthcare,11 Aravind12 or the GE Mac 400.13 All three began in India and there are several reasons that makes the Indian context conducive for healthcare innovations.26Globally, the early growth in research and development of frugal devices in healthcare has been led by companies setting up RnD centres in emerging markets, for instance, General Electric, Philips and Zhongxing, and by social enterprises working in developing and emerging markets, as with the Jaipur foot or knee, a prosthetic for amputees or eRanger, a durable rural ambulance. Consequently, many of the examples of frugal innovations are focused on medical technologies, products and devices.27 But we found that the adoption of products or technology is complicated when healthcare innovation starts with a technology searching for an application, such as with i-calQ or ReMeDi (data communication platform for rural areas). Healthcare starts with needs not solutions and with means to deliver better healthcare. Therefore, we extended our search to process and policy innovations including care delivery models. Our global search has revealed less well known healthcare delivery frugal innovations from around the world that have had positive effect on service delivery, quality of care and improved access.
Two of our cases, the Brazilian Family Health Strategy and the Singaporean Gericare@North, were developed at the national policymaking level and have scaled nationally, the Brazilian model having done so at much larger scale. Saude Crianca, instead was developed at the grassroots in response to the holistic needs of families beyond healthcare interventions. Although grassroots can be a source of innovations that are uniquely fit for local needs, they have the additional challenge of scaling up beyond local use. Saude Crianca was piloted in neighbouring Argentina without much success.
On the practical side, by taking out costs and increasing efficiency, transforming care delivery, expanding access to quality care, improving patient outcomes and increasing the sustainability of the health system, frugal innovations have the potential of disrupting inefficient health system practices. In general, we found that frugal innovation can improve healthcare access and outcomes by (1) redesigning institutional and organisational structures by, for instance, in Brazil employing nationwide use of community health workers or teams of volunteers that assist families to escape the underlying socioeconomic causes of ill health; (2) leveraging technologies as platforms for further innovations such as in Singapore through telemedicine and video conference consultations and (3) reshaping work by enabling self-diagnostics and task-shifting, as in the case of PEEK Vision and i-calQ.
On the theoretical side, there is much that innovation scholars can learn from empirical studies of frugal innovation in the healthcare sector. For instance, our work has found that (1) frugal innovations could be low-tech, simple and mundane such as in the case of the Brazilian community health worker programme, but also high-tech, scientifically complex and esoteric, as in the case of i-calQ; (2) frugal innovations can improve the lives and livelihoods of patients beyond health outcomes measured out of direct medical interventions or hospitalisation, as in the case of Saude Crianca which treats socioeconomic ailments of families rather than diseases; (3) healthcare delivery models can be used as conduits to harness the power of multiple frugal technology innovations, as in the case of GeriCare@North which is exploring use of smartphone technologies to diagnose remotely; and (4) frugal innovations are not limited in relevance, sourcing and development to low-income and middle-income countries, indeed many frugal innovations have been ideated or developed in high-income settings such as PEEK Vision with its main founders based in the UK.28
On the policy side, there needs to be awareness that despite the potential in hundreds of frugal and reverse innovations, there remain cognitive barriers among professionals in high-income settings who usually view innovations from low-resource settings with scepticism.29 Part of the problem has been the difficulty in assessing quality through randomised clinical trials. And where there are few instances that have established empirical evidence of equivalent outcomes for affordable healthcare interventions, the relevance of frugal models or technologies are usually espoused as relevant to mainly low-resource settings. See, for instance, two recent articles in the Lancet, one for affordable vaccines,30 and the other for the affordable assessment of haemoglobin,31 as well as one article in New England Journal of Medicine on mosquito mesh for hernia surgery.32 The NEJM paper concludes: ‘In summary, this study showed that a low-cost mesh can be used in hernia repair with excellent clinical outcomes that do not differ significantly from those achieved with commercial mesh. These results support the use of low-cost mesh for hernia repair in resource-scarce settings, after appropriate training of the staff performing the procedures’(Online).
Despite there being growing clinical evidence of the efficacy of such alternative frugal innovations, their relevance is often limited to low-resource settings. If there is an affordable innovation of equivalent quality, why limit its use only in low-resource settings? We find that frugal innovations face similar challenges of global diffusion as those faced by mosquito mesh (also known as low cost or LDPE mesh) for hernia surgery. Literature on diffusion, implementation or change management will have us believe, rightfully so for the most part, that it would be necessary for potential adopters to evaluate the technical features of any innovation; adapt them to local needs, funding mechanisms and regulations; institute change management processes and gradually delayer existing services.33–41 However, we argue that there are two social issues that need attention even before the technical ones can be managed. There are many institutional barriers to accelerating the global adoption of frugal innovations and in our other complementary stream of work, we are only beginning to understand the extent of some of the associated social and cognitive barriers.29 In the innovation development and diffusion continuum, the largely social motivations42 of the frugal innovators have to be understood and negotiated to make it favourable for the source innovators to want to share information and time with potential global adopters, particularly with those in high-income settings. At the same time, the largely reticent perceptions of the potential adopters in different contexts43 44 have to be managed better, in part through collection of evidence of use but also through curation or brand management of source.
Finding these potential innovations that are affordable, adaptable and accessible quality of care for worldwide marginalised or underserved patients is easy, diffusing them locally and globally for both rich and poor is hard. Part of the challenge is to narrow down the innovations to their core offering, which we have tried, such that it might be considered for translation. The other part of the challenge is that healthcare professionals often do not look to adopt frugal innovations and policy makers have yet to introduce incentives for frugal innovators and adopters. Add to this, the challenge that innovation scholars have yet to fully understand what makes frugal innovations models and strategies successful and how to diffuse them globally.45 Nevertheless, this effort by the Commonwealth Fund to find and showcase less well-known examples of frugal innovations in healthcare is a necessary step in progressing to pilot and carry out further studies to overcome challenge of adaptation and implementation.
Limitations
We discovered many innovations, out of which only a handful were studied in-depth through case studies. The Commonwealth Fund did not identify specific sites or systems for IGHI to study. Therefore, it was not possible to develop traditional, economic business cases, with site-specific recommendations for implementation. As the Commonwealth Fund preferred an assessment of adoptability across the USA, the case studies were rather generic in terms of implementation. We conducted telephone interviews with a range of potential US providers, carried out an analysis of economic potential for transferability to the USA and proposed a limited business case for possible US adopters. If provided with a steer about exactly when and where innovations could be piloted, a more detailed business case can be made. In our in-progress follow-up work to explore the potential of piloting frugal innovations in the NHS, we have revised our strategy by spending considerable effort to generate buy-in from potential pilot sites before developing site-specific cases.
Although we were able to identify several innovations as having potential to be frugal based on self-reported evidence or claims by innovators, we were not able to explain exactly why an innovation is frugal unless we conduct extensive case study investigation as we did with the three shortlisted healthcare delivery innovations. But given the scale and scope of these innovations, a full system-wide cost and economic analysis is unwieldy. We continue to evaluate the innovations as to why the innovations are frugal and for whom and which level of analysis. And given that some of the most highly acclaimed frugal innovations are surgical based, Narayana and Aravind, we are investigating the role of frugal innovations in surgery. And in assessing potential for reverse diffusion, our database suggests very few of these have successfully reversed. Our next research stream is looking at identifying innovations that have in fact diffused across contexts particularly from low-resource to high resource settings and why, that is, they have become reverse innovations. And we seek to improve how best to predict which innovations have potential for diffusion in other contexts.
Conclusion
There are growing efforts to look for and learn from successful cases of frugal innovations. The Institute of Global Health Innovation was tasked by the Commonwealth Fund to recommend innovations that could potentially translate from abroad to the USA. Our shortlisted innovations showed that a systematic search for frugal innovations can reveal many less well known examples some of which have potential for translation to the USA and indeed to the world. However, finding and showcasing these innovations is just a first step. With a view to delivering better health and at the same time bending the growth cost curve by learning from such examples of frugal innovations in healthcare, clinicians, academics, policymakers and entrepreneurs need to work together and learn about new innovations and practices that inform theory, practice and policy, and more importantly, to shun prejudices that impede our learning.
Acknowledgments
We are grateful to the innovators and stakeholders who made themselves available for interviews and case study development and to colleagues at Innovations in Healthcare, Duke University and at The Commonwealth Fund for their feedback on draft reports and cases.
References
Footnotes
Contributors All co-authors contributed equally to different aspects of the study, including research, review and revision of paper. Specifically, YB wrote the first draft of article and submitted; YB, MP, JMQ and GP planned the study; MP, HW, HP and AC conducted field trip data collection and YB, MP, MH, HW, HP, AWC, GP and AD wrote the case studies. AD was the Principal Investigator and led the study.
Funding This research was funded by the Commonwealth Fund, USA.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.