Article Text

Abstract
Background The unmet burden of surgical care is high in low-income and middle-income countries. The Lancet Commission on Global Surgery (LCoGS) proposed six indicators to guide the development of national plans for improving and monitoring access to essential surgical care. This study aimed to characterise the Somaliland surgical health system according to the LCoGS indicators and provide recommendations for next-step interventions.
Methods In this cross-sectional nationwide study, the WHO’s Surgical Assessment Tool–Hospital Walkthrough and geographical mapping were used for data collection at 15 surgically capable hospitals. LCoGS indicators for preparedness was defined as access to timely surgery and specialist surgical workforce density (surgeons, anaesthesiologists and obstetricians/SAO), delivery was defined as surgical volume, and impact was defined as protection against impoverishment and catastrophic expenditure. Indicators were compared with the LCoGS goals and were stratified by region.
Results The healthcare system in Somaliland does not meet any of the six LCoGS targets for preparedness, delivery or impact. We estimate that only 19% of the population has timely access to essential surgery, less than the LCoGS goal of 80% coverage. The number of specialist SAO providers is 0.8 per 100 000, compared with an LCoGS goal of 20 SAO per 100 000. Surgical volume is 368 procedures per 100 000 people, while the LCoGS goal is 5000 procedures per 100 000. Protection against impoverishing expenditures was only 18% and against catastrophic expenditures 1%, both far below the LCoGS goal of 100% protection.
Conclusion We found several gaps in the surgical system in Somaliland using the LCoGS indicators and target goals. These metrics provide a broad view of current status and gaps in surgical care, and can be used as benchmarks of progress towards universal health coverage for the provision of safe, affordable, and timely surgical, obstetric and anaesthesia care in Somaliland.
- surgery
- health policy
- public health
- international health services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first nationwide study that comprehensively evaluates the surgical system, including the public and private sectors, in Somaliland.
This study follows the Lancet Commission on Global Surgery indicators to evaluate surgical preparedness, delivery and impact on Somaliland.
Data on perioperative mortality rates were not included as most hospitals in Somaliland do not collect these data.
Our reported surgical workforce density did not include data on non-specialist physicians and non-physician clinicians who may provide surgical care in Somaliland.
Introduction
Over 5 billion people around the world lack safe, affordable and timely access to surgical and anaesthesia care, with the overwhelming burden being among persons in low/middle-income countries (LMICs).1–3 To address this crisis, targeted and accurate measurement of surgical care is a critical first step. However, the misconception that surgery is an expensive intervention has prevented it from playing a significant role in global health for a long time.4 5 Investing in surgery is highly cost-effective and beneficial at a macro-level and micro-level. Surgery promotes the overall scaling up of national health systems and provides financial risk protection to families that otherwise may be pushed into the poverty or have reduced their chances of moving out of poverty.1 4 6 Global surgery has gained recent attention due to paramount events such as the creation of the Lancet Commission on Global Surgery (LCoGS) and the inclusion of four of the six LCoGS indicators among the core 100 WHO and World Development indicators.1 7 8
The 2015 LCoGS proposed six surgical indicators through an extensive and iterative process led by experts from various disciplines, surgical specialties and countries.1 These six indicators and associated target goals define the preparedness for surgical and anaesthesia care (access to essential surgery and workforce density), delivery of care (quantifying the surgical volume and perioperative mortality rates) and impact of care (protection against impoverishing and catastrophic expenditures).1 These indicators have been used as a template to assess surgical care in several countries, which in turn have supported the development of National Surgical, Obstetrical and Anesthesia Plans (NSOAPs).9 10
Somaliland is a low-income country in sub-Saharan Africa with significant health and economic challenges. After emerging from the civil war in 1991, the government of Somaliland focused on rebuilding its hospitals, clinics and health posts, and devoted 3% of the national budget to rebuild its health sector.11 12 Somaliland has a gross domestic product (GDP) of $348 per capita (making it the fourth poorest country in the world), has a population of approximately 4 million people and some of the poorest health outcomes in the African region.13–19 Our previous work and that of others have characterised the surgical infrastructure for children in the country.6 19 20 The goal of the current study was to characterise the Somaliland surgical health system according to the LCoGS surgical indicators.
Methods
Setting
This cross-sectional study took place in Somaliland, a country in the Horn of Africa which achieved relative stability and has an autonomous government since separation from Somalia in 1991. The population estimate from the 2014 Somali census is 3.5 million people.21 Somaliland is made up of six regions—Awdal, Maroodi Jeex (containing the capital city of Hargeisa), Sahil, Sanaag, Sool and Togdheer—with 40% of the population living in Hargeisa.22 The public health system is comprised of primary health units, health centres, referral health centres, regional hospitals and one national referral hospital. Specialty hospitals include seven tuberculosis hospitals, one female fistula hospital, one children’s hospital and one mental health hospital. An estimated 60% of health services are provided through the private sector, consisting of non-government organisations, private health practitioners and hospitals, and traditional practitioners.12
Hospital selection
Hospitals were included in the study if they had the capacity to perform surgery (defined as the presence of at least one operating room), yielding 16 hospitals. We were not able to obtain data from one private hospital, resulting in a final study cohort of 15 hospitals. Our in-country research manager asked permission from each hospital director or senior administrator for participation in the study, and presented the study’s letter of approval from the Ministry of Health.
Data collection
Our current study is built on data collected by our team and reported in previous studies.6 19 20 We assessed hospital capacity at each facility using the WHO’s Surgical Assessment Tool–Hospital Walkthrough and the Global Initiative for Children’s Surgery Global Assessment in Pediatric Surgery tool.23 24 The survey included data on service delivery, the number of admissions and surgical procedures per month, whether the facility tracked perioperative in-hospital mortality, and the number of laparotomies, caesarean sections and open fracture repairs (ie, the three LCoGS ‘bellwether’ procedures). To assess each facility’s workforce, the survey quantified the number of staff, including surgeons, anaesthesiologists, non-physician anaesthetists, obstetricians, nurses and administrative staff. Each staff member was counted only once even if they worked across multiple health facilities. To assess each facility’s infrastructure, the survey asked about the availability of essential resources (ie, electricity, running water, oxygen), the number of hospital beds and operating rooms, and the number of anaesthesia machines and ventilators.
Indicator assessment
The LCoGS indicators include 6 items pertaining to surgical care preparedness (indicators 1 and 2), delivery (indicators 3 and 4) and impact (indicators 5 and 6) (table 1). We did not assess whether each hospital tracked perioperative mortality rates, as this metric is generally not collected in Somaliland. Thus, indicator 4 was not included in the analysis. Data tabulation and analyses were performed using Microsoft Excel and SAS V.9.3. Geographical mapping and analyses were performed using ArcGIS (Environmental Systems Research Institute 2012, Redlands, California, USA).
Lancet Commission on Global Surgery indicator definitions and targets.1
Indicator 1
Access to timely essential surgery. Geographical locations of the 15 surgically capable hospitals, defined by the presence of an operating room, were recorded using a smart phone Global Positioning System application. Locations of the 15 hospitals were mapped and used as destination points from which distance calculations were made. Network service area analysis was used to determine the per cent of the population within a 2-hour radius of the surgically capable hospitals throughout the country. A travel rate of 30 km/hour was used to determine the geographical area within a 2-hour drive of surgically capable hospitals using available Somaliland road infrastructure data. Population estimates within each geographical area were made using data from the 2014 Somalia census.21 Surgical capacity was defined as the existence of an operating room within the hospital. This geospatial method did not account for transportation wait time or topography of the land. However, travel times were reviewed by the in-country data team to confirm validity of the estimated travel times between locations. The service area map was combined with a dot density map to depict the relations between surgical care coverage and population distribution at the regional level.
Indicator 2
Surgical workforce density. The surgical workforce density was defined as the number of specialist surgeons, anaesthesiologists and obstetricians (SAO) per 100 000 population. Surgeons included specialties available within Somaliland (general surgeons, colorectal surgeons, neurosurgeons and otolaryngologists). Anaesthesiologists did not include nurse anaesthetists. The surgical workforce density was calculated as the number of SAO per 100 000 population. In addition to the national SAO workforce density, region-specific densities were also estimated.
Indicator 3
Surgical volume. Surgical volume was obtained through the country-wide hospital assessment. We included all procedures recorded in hospital logbooks between 1 January 2017 and 31 December 2017 using previously described methods.20 Exclusion criteria included procedures performed outside of the operating rooms. We collected data on demographics, surgical diagnosis and surgical procedure(s) performed. Data did not include admission information, comorbidities, complications or outcome. We quantified the number of the LCoGS-defined bellwether procedures (open fracture repairs (all types), caesarean section deliveries and laparotomies).1
Indicator 5
Protection against impoverishing expenditure. Protection against impoverishing expenditure was defined as 100 % population at risk of impoverishing expenditures. Impoverishment was defined as any income below the poverty line after out-of-pocket (OOP) payments, including medical and non-medical costs, for surgery. The threshold for impoverishment expenditure for Somaliland was defined as any income below a value of:
(% OOP expenditure)*(average cost of surgery)+(Somaliland poverty line).
For costs per operation, we used $200 as a proxy due to lack of information of operative costs for each hospital. The $200 value was chosen as it represents the mean value between costs per surgical procedure in a low-income country ($179) and a lower middle income country ($219) calculated as previously described.25 The $200 costs cover all direct costs, including preoperative and postoperative hospitalisation, as well as the recurrent costs of running a surgical service such as salaries, utilities, equipment, medical supplies and medicine for the procedure itself. We confirmed this amount based on OOP expenses from one private hospital in Somaliland, which used an average of $200 per procedure. Non-medical expenses, such as transportation and lodging, were estimated at $60 based on previous literature.26 The expected proportion of OOP costs for healthcare was provided by the hospital administration during the survey data collection. The threshold for the poverty line in Somaliland was set at $220 based on previous literature.13
Indicator 6
Protection against catastrophic expenditure. Protection against catastrophic expenditures was defined as 100%—population at risk of catastrophic expenditure.1 Catastrophic expenditure was defined as direct OOP expenses greater than 40% of the GDP per capita, excluding subsistence costs. The risk of catastrophic expenditure for each hospital and region was determined by dividing all direct and indirect OOP expenses by $348, Somaliland’s GDP per capita.26
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
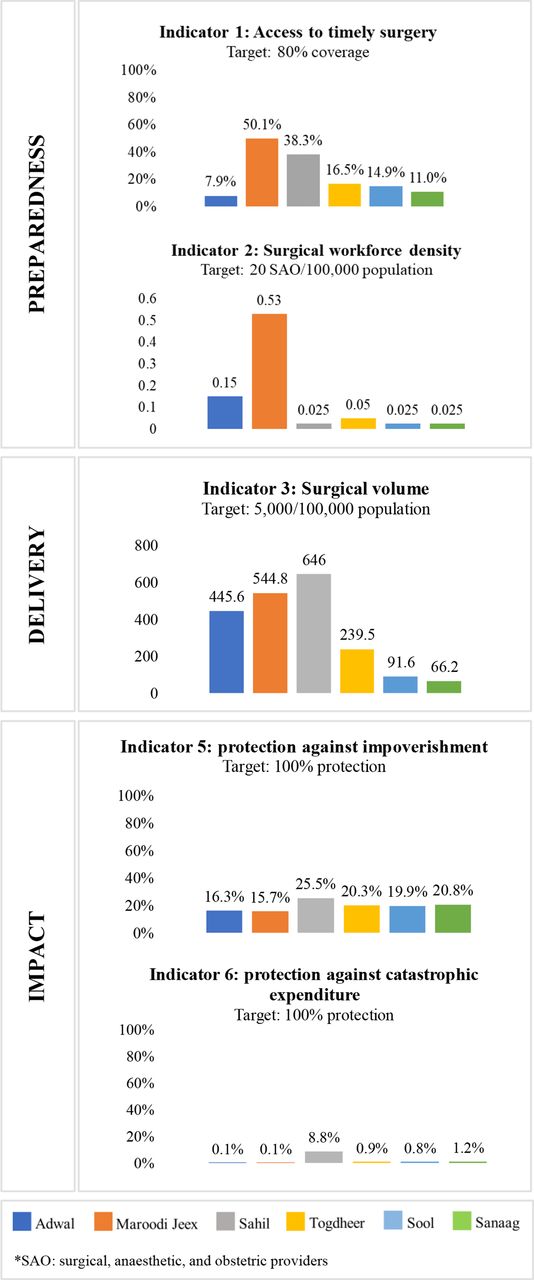
The surgical system in Somaliland did not reach any of the target indicator goals as defined by LCoGS, with each indicator lagging behind its target by 76% or more (figure 1). The greatest need was for protection against catastrophic expenditure and inadequate SAO density.

Somaliland indicators compared with the Lancet Commission on Global Surgery (LCoGS) targets. SAO, surgeons, anaesthesiologists and obstetricians.
Preparedness
Only an estimated 19% of persons in Somaliland live within a 2-hour access to a surgically capable facility, translating to 24% of the LCoGS goal of at least 80% population coverage (figure 2). The number of specialist SAO physicians was 0.8 per 100 000 population, or 4% of the LCoGS goal of 20 SAO per 100 000. Access to surgery ranged from 36% in Maroodi Jeex to below 6% in Awdal, Sool and Sanaag. Of the total workforce of 32 SAO in the country, 15 were surgeons, 3 were anaesthesiologists and 14 were obstetricians (table 2). The number of surgeons ranged from 10 in Maroodi Jeex to 0 in Sool, Togdheer or Sanaag, while the number of obstetricians ranged from 8 in Maroodi Jeex to 0 in Sahil. Of the three anaesthesiologists, all three were located in Maroodi Jeex (the capital city).
Surgeon, anaesthesia and obstetrics workforce density and procedures by region

Catchment population within a 2-hour travel time from the closest surgically capable hospital.
Delivery
The surgical volume was 368 procedures per 100 000 people, that is, less than the 7% of the LCoGS goal of 5000 procedures per 100 000 population. Surgical volume ranged from 646 per 100 000 population in Sahil to 66 per 100 000 population in Sanaag (figure 3). Total volume of procedures ranged from 681 in Maroodi Jeex to 250 in Awdal (table 2). Of these procedures, laparotomies ranged between 1 and 20 per month (in Sahil or Sool and Awdal, respectively), caesarean sections between 6 and 100 per month (in Sool and Maroodi Jeex, respectively), and open fracture repairs between 0 and 40 per month (in Sahil, Sool, or Togdheer and Awdal, respectively).

{kind=link}
{kind=link}
{kind=link}
Lancet Commission on Global Surgery indicators for Somaliland, stratified by region.
Impact
Protection from impoverishment was only 18% of the LCoGS goal of 100% protection by 2030. Risk of impoverishment was high throughout the country and ranged between 74.5% in Sahil and 84.3% in Maroodi Jeex (figure 3). Protection against catastrophic expenditures was 1% of the LCoGS goal of 100% protection by 2030. The risk of catastrophic expenditure was greater than 90% throughout the entire country.
Discussion
As surgical care is increasingly recognised as an essential component of a functional healthcare system, understanding the surgical landscape of a country is vital for healthcare scale-up plans contextualised to that country. The LCoGS indicators measure several domains of surgical care related to preparedness, delivery and impact of care. These indicators are increasingly used around the world as a framework to scale up surgical care in the country through a comprehensive, system-level perspective.27 We found that Somaliland’s surgical system achieves only a small fraction of these target goals, with the greatest need found in rural areas.
Our study found large gaps in surgical care preparedness, delivery and impact. Preparedness, including access to surgical care and workforce density, are far below the LCoGS targets, consistent with other sub-Saharan African countries.3 9 27–37 The reasons for lack of access to surgical care in Somaliland are multifactorial, but are largely due to the limited number of locally accessible surgically capable hospitals and existing road networks. The majority of surgically capable hospitals are within the urban Maroodi Jeex region, with only one hospital located in the more rural regions. Although the concentration of hospitals and SAO providers correspond with population density, overall, the surgical care coverage remains limited in all regions, particularly in the northwest and southeast areas of the country. After almost a decade of civil conflict (1982–1991), the country was left with severe damage and deterioration to road networks and healthcare infrastructure,38 and only 15% of the primary roads in urban areas and networks connecting rural to urban areas are considered to be in good condition.39 Workforce density is also low in the more rural parts of the country, with most of the SAO concentrated within urban areas. Delivery of surgical care as measured by the volume of procedures was low particularly in rural areas and is likely related to the workforce density within each area. For example, 57% of all procedures per month occurred in the urban Maroodi Jeex region which has 65% of all SAO. However, high surgical volume, as in Sahil, may be explained by the response of other health professionals to the high demand of emergency surgical care in the absence of specialised SAO providers.20
The financial impact of surgical care is evident through the high rates of financial strain on families, which limits Somaliland’s capacity to attain universal health coverage (UHC) as advocated by the World Bank, United Nations and WHO. The provision of surgery in Somaliland is largely dependent on a person’s financial means to pay for OOP expenses, similar to high rates of OOP spending in many LMICs.40 The risk of being pushed into poverty or having reduced opportunities to move out of poverty due to OOP expenses for surgical care in Somaliland is one of the highest compared with other LMICs,6 which is particularly challenging as Somaliland is the fourth poorest country in the world, with an estimated 35% of households living under $100 per month.6 36–40 Our findings highlight the need for inclusion of surgical care in the country’s UHC scheme in order to prevent impoverishing and catastrophic expenditure due to OOP expenses, especially among at-risk communities.5 41 42
As a post-conflict country, the healthcare system of Somaliland experiences many structural challenges, with just 3% of the national budget designated to the healthcare. In this context, outlining a strategic national healthcare plan to improve access to surgery is required. Such a plan should address deficiencies in the surgical system as defined by the LCoGS indicators, including preparedness, delivery and impact. Each LCoGS indicator should be interpreted in conjunction with other indicator metrics to fully understand how gaps in care are inter-related.43 Evaluating surgical capacity begins with accessibility. However, geographical coverage is just one dimension of access and does not ensure that people receive proper surgical care.27 44–49 Patients that eventually reach healthcare facilities might not be able to receive surgical care due to deficits in infrastructure and workforce.20 50 Thus, interpreting each indicator independently of the others will only provide a limited understanding of the surgical needs within a country.
One way to comprehensively evaluate surgical systems and gaps in care on a national level is through country-specific NSOAPs. The purpose of NSOAPs is to improve surgical care through the six major building blocks of a health system: infrastructure, workforce, service delivery, information management, finance and leadership/governance.1 One of the first steps in developing a country-specific NSOAP is identifying gaps for each building block.10 Although Somaliland does not have an NSOAP, our paper provides critical data regarding infrastructure, workforce, service delivery, and the need for financing schemes to protect individuals from catastrophic and impoverishing expenditures.
Somaliland may be able to benefit from lessons learnt in other LMICs during enactment of NSOAPs. The Republic of Zambia was one of the first countries to conduct a baseline assessment of the LCoGS indicators and use those in a quality improvement plan within an NSOAP.51–53 To date, other countries including Ethiopia,51 54 India51 55 and Tanzania51 56 have adopted a similar process to develop their NSOAPs. These experiences suggest that Somaliland may benefit from upgrading geographically strategic facilities and allocating resources to high-impact healthcare facilities to ensure equity and reinforce existing surgical capacity.57–59 Task shifting and task sharing, partnerships with other countries and the private sector, culturally embedded training and increase of incentives are other ways to efficiently scale up workforce density.1 60 We encourage continuous data collection as part of an NSOAP anchored within the overall country’s national health strategic plan, and driven by the Somaliland Ministry of Health to ensure standardisation, integration and sustainability over time.10 27 Furthermore, engagement of local champions and healthcare workers on the ground from the early stages will be pivotal to ensure success and continuity.51 61–63
Successful implementation of NSOAPs also requires involving strong governmental leadership and other stakeholders, establishing surgical priorities, and allocating funding from partnerships and non-traditional sources.51 54 One example which will be helpful for Somaliland is that of the Saving Lives Through Safe Surgery in Ethiopia, which has shown the value of an established comprehensive system of educational/training packages, leadership/mentoring programmes, national perioperative guidelines, implementation of the WHO Surgical Safety Checklist, and requirements for functional operating rooms, standardised equipment, supplies and purchasing.54 In Tanzania, the NSOAP emphasises the coverage of essential surgical care in national health insurance schemes, implementation of electronic medical records for surgery-related data, simultaneous strengthening of lower-level and higher-level hospitals to reinforce referral pathways, and implementation of regional training to improve local retention of SAO providers.56
Limitations
Our study has several limitations. First, our reported surgical workforce density might under-represent the entire surgical workforce in Somaliland as we did not collect data on non-specialist physicians and non-physician clinicians who may provide surgical care. Second, most hospitals in Somaliland do not collect data on perioperative mortality rates. This indicator is the most widely adopted measurement for surgical outcomes and highlights delays to receiving care.27 There are still few studies that have successfully measured perioperative mortality rates without relying on modelling data.64 Similarly, we did not measure quality of care within the hospital settings, nor were able to assess the impact of surgical capacity on mortality. A facility assessment tends to pick up on one of the three aspects of the Donabedian framework elements—that of structure and not process and outcome.65 However, the presence of an operating room does not indicate a comprehensive analysis of hospital capacity. Therefore, it was only used as an initial selection criterion on which the LCoGS indicators were applied. Third, our data on impoverishing and catastrophic expenditures may have been based on inaccurate surgical costs. Few studies in other countries have accurate primary data on surgery related costs and OOP expenditures, as most are based on modelling.26 29 64 66 Although we collected limited primary data on financial costs, these reported costs likely underestimate the total costs of procedures, including indirect costs of lost earnings. However, we attempted to account for the wide range of surgical costs depending on the procedure by including lower and upper limits in our expenditure calculations. Fourth, measuring household income is challenging for many households in LMICs as many do not work in the formal sector or have a consistent income.67 68 Therefore, our attempts to calculate the impact indicators for Somaliland may be limited as this average might be overestimated for the poorest regions of the country. These findings emphasise the need for improved primary data collection regarding OOP surgical costs in LMICs.
Probably the most important limitation to our analysis is the challenge among the LCoGS indicators to correctly measure their respective components. The LCoGS indicators were originally defined using data from nationally representative 194 WHO member states. However, all indicators, except for surgical workforce, included data from less than half of WHO member states.27 In addition, many countries had differing definitions of indicators, hindering comparability and potentially leading to erroneous estimates.27 Taking access to care as an example, geographical proximity is only one dimension of access and does not necessarily account for the impact of road conditions or type of transportation. Similarly, the definition of surgical volume did not take into account varying population needs depending on the specific country. Perhaps the most potentially biased indicator is expenditure, as this indicator was defined solely on modelling estimates with no national-level data. Although these challenges may have affected our estimates, our data can serve to drive collection of country-wide surgical data in the future.
Conclusion
As Somaliland continues to rebuild its healthcare infrastructure, incorporating surgical care as an essential component of its national healthcare plan is critical. We found large limitations in the overall surgical system using the LCoGS indicators. Implementation of efforts to scale up surgery using these target goals can help Somaliland progress in improving safe, affordable, and timely surgical, obstetric and anaesthesia care, and achieve UHC for its population.
Acknowledgments
We want to thank the Global Initiative for Children’s Surgery (GICS) for its support of this work. GICS (www.globalchildrenssurgery.org) is a network of children’s surgical and anaesthesia providers from low-income, middle-income and high-income countries collaborating for the purpose of improving the quality of surgical care for children globally.
References
Footnotes
SD and CFC-C are joint first authors.
SD and CFC-C contributed equally.
Collaborators Naomi Wright, Guy Jensen, Etienne St-Louis, David Grabski, Yasmine Yousef, Neema Kaseje, Laura Goodman, Jamie Anderson, Emmanuel Ameh, Tahmina Banu, Stephen Bickler, Marilyn Butler, Michael Cooper, Zipporah Gathuya, Patrick Kamalo, Bertille Ki, Rashmi Kumar, Vrisha Madhuri, Keith Oldham, Doruk Ozgediz, Dan Poenaru, John Sekabira, Lily Saldaña Gallo, Sabina Siddiqui, Benjamin Yapo, Francis A Abantanga, Mohamed Abdelmalak, Nurudeen Abdulraheem, Niyi Ade-Ajayi, Edna Adan Ismail, Adesoji Ademuyiwa, Eltayeb Ahmed, Sunday Ajike, Olugbemi Benedict Akintububo, Felix Alakaloko, Brendan Allen, Vanda Amado, Shanthi Anbuselvan, Theophilus Teddy Kojo Anyomih, Leopold Asakpa, Gudeta Assegie, Jason Axt, Ruben Ayala, Frehun Ayele, Harshjeet Singh Bal, Rouma Bankole, Tim Beacon, Zaitun Bokhari, Hiranya Kumar Borah, Eric Borgstein, Nick Boyd, Jason Brill, Britta Budde-Schwartzman, Fred Bulamba, Bruce Bvulani, Sarah Cairo, Juan Francisco Campos Rodezno, Massimo Caputo, Milind Chitnis, Maija Cheung, Bruno Cigliano, Damian Clarke, Tessa Concepcion, Scott Corlew, David Cunningham, Sergio D'Agostino, Shukri Dahir, Bailey Deal, Miliard Derbew, Sushil Dhungel, David Drake, Elizabeth Drum, Bassey Edem, Stella Eguma, Olumide Elebute, Beda R Espineda, Samuel Espinoza, Faye Evans, Omolara Faboya, Jacques Fadhili Bake, Tatiana Fazecas, Mohammad Rafi Fazli, Graham Fieggen, Anthony Figaji, Jean Louis Fils, Tamara Fitzgerald, Randall Flick, Gacelle Fossi, George Galiwango, Mike Ganey, Maryam Ghavami Adel, Vafa Ghorban Sabagh, Sridhar Gibikote, Hetal Gohil, Sarah Greenberg, Russell Gruen, Lars Hagander, Rahimullah Hamid, Erik Hansen, William Harkness, Mauricio Herrera, Intisar Hisham, Andrew Hodges, Sarah Hodges, Ai Xuan Holterman, Andrew Howard, Romeo Ignacio, Dawn Ireland, Enas Ismail, Rebecca Jacob, Anette Jacobsen, Zahra Jaffry, Deeptiman James, Ebor Jacob James, Adiyasuren Jamiyanjav, Kathy Jenkins, Maria Jimenez, Tarun John K Jacob, Walter Johnson, Anita Joselyn, Nasser Kakembo, Phyllis Kisa, Peter Kim, Krishna Kumar, Charlotte Kvasnovsky, Ananda Lamahewage, Monica Langer, Christopher Lavy, Taiwo Lawal, Colin Lazarus, Andrew Leather, Chelsea Lee, Basil Leodoro, Allison Linden, Katrine Lofberg, Jonathan Lord, Jerome Loveland, Leecarlo Millano Lumban Gaol, Pavrette Magdala, Luc Kalisya Malemo, Aeesha Malik, John Mathai, Marcia Matias, Bothwell Mbuwayesango, Merrill McHoney, Liz McLeod, Ashish Minocha, Charles Mock, Mubarak Mohamed, Ivan Molina, Ashika Morar, Zahid Mukhtar, Mulewa Mulenga, Bhargava Mullapudi, Jack Mulu, Byambajav Munkhjargal, Arlene Muzira, Mary Nabukenya, Mark Newton, Jessica Ng, Karissa Nguyen, Laurence Isaaya Ntawunga, Peter M Nthumba, Alp Numanoglu, Benedict Nwomeh, Kristin Ojomo, Maryrose Osazuwa, Emmanuel Owusu Abem, Shazia Peer, Norgrove Penny, Robin Petroze, Vithya Priya, Ekta Rai, Lola Raji, Vinitha Paul Ravindran, Desigen Reddy, Henry Rice, Yona Ringo, Amezene Robelie, Jose Roberto Baratella, David Rothstein, Coleen Sabatini, Soumitra Saha, Saurabh Saluja, Lubna Samad, Justina Seyi-Olajide, Bello B Shehu, Ritesh Shrestha, David Sigalet, Martin Situma, Emily Smith, Adrienne Socci, David Spiegel, Peter Ssenyonga, Jacob Stephenson, Erin Stieber, Richard Stewart, Vinayak Shukla, Thomas Sims, Faustin Felicien Mouafo Tambo, Robert Tamburro, Mansi Tara, Ahmad Tariq, Reju Thomas, Leopold Torres Contreras, Stephen Ttendo, Benno Ure, Luca Vricella, Luis Vasquez, Vijayakumar Raju, Jorge Villacis, Gustavo Villanova, Catherine deVries, Amira Waheeb, Saber Waheeb, Albert Wandaogo, Anne Wesonga, Omolara Williams, Sigal Willner, Nyo Nyo Win, Hussein Wissanji, Paul Mwindekuma Wondoh, Garreth Wood, George Youngson, Denléwendé Sylvain Zabsonre, Luis Enrique Zea Salazar, Adiyasuren Zevee, Bistra Zheleva, Kokila Lakhoo, Diana Farmer
Contributors TC, EAI, HER and ERS contributed to the conceptualisation of the project. EAI and DP contributed to the conceptualisation of the project and writing of the manuscript. SD, TC and MM oversaw all data collection efforts. HER and ERS oversaw the project. CFC-C, TC, HER and ERS conceptualised the design, analysed the data, and contributed to the writing and revising of the manuscript. AJML contributed to data analysis, interpretation and revision of the manuscript. All authors contributed to the revision and approved the final version of the manuscript.
Funding Funding for the original study on which this article is based was provided by Duke University’s Duke Global Health Institute (ERS) and by Baylor University’s Robbins College of Health and Human Sciences (ERS).
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests For the original study on which this article is based, TC and ERS received grants from Duke University’s Duke Global Health Institute and grants from Baylor University.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Institutional Review Board (IRB) approval was granted from Duke University. Since Somaliland does not have a national IRB, a letter of approval for the study was obtained from the Somaliland Ministry of Health.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Data are available by request by emailing Emily_r_smith@baylor.edu.