Article Text

Abstract
Background and objectives Vaginal breech delivery (VBD) is known to be associated with more perinatal and maternal complications. Very few studies on the subject have been carried out in poor-resource settings. The aim of this study was to determine maternal and neonatal outcomes in carefully selected cases of VBD for singleton term pregnancies in a tertiary centre in Cameroon.
Design A retrospective cohort study.
Setting A tertiary hospital in Yaounde, Cameroon.
Participants Cases of VBD of newborns weighing 2500–3500 g were matched in a ratio of 1:4 to consecutive vaginal cephalic deliveries (VCDs) of newborns weighing 2500–3500 g over a 5-year period. Both groups were matched for maternal age and parity. We excluded cases of multiple gestations, footling breech, clinically inadequate maternal pelvis, preterm delivery, post-term pregnancies, fetal demise prior to the onset of labour, placenta praevia and fetal anomaly incompatible with vaginal delivery.
Outcome measures Neonatal and maternal adverse outcomes of VBD observed till 6 weeks after delivery analysed using Bonferroni correction.
Results Fifty-three (53) VBDs were matched against 212 VCD. Unlike women who had VCD, those who underwent VBD were more likely to have prolonged labour (OR 8.05; 95% CI 3.00 to 11.47; P<0.001), and their newborns were more likely to suffer from birth asphyxia (OR 10.24; 95% CI 4.92 to 21.31; P<0.001).
Conclusion The study infers a strong association between VBD of singleton term pregnancies and maternofetal morbidity when specific protocols are applied. This, however, failed to translate into higher differences in perinatal mortality. This finding does not discount the role of VBD in low-income countries, but we emphasise the need for specific precautions like close monitoring of labour and adequate anticipation for neonatal resuscitation in order to reduce these complications.
- breech
- vaginal delivery
- cephalic presentation
- singleton term pregnancies
- outcome
- Cameroon
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The use of guidelines to select cases of vaginal breech delivery in order to decrease the risk of selection bias in the findings obtained.
Bias was further reduced by calculating Bonferroni adjusted P values.
The study had a retrospective nature of data collection, which was subject to a potential risk of incorrectly completed records.
The study was carried out in a single centre with standards of a tertiary level of care, which implies cautious generalisation of results to health facilities not having the same level of care.
Introduction
Breech presentations represent 3%–4% of all fetal presentations at term.1 Vaginal breech deliveries (VBDs) are associated with a 10-fold increase in perinatal mortality when compared with vaginal cephalic deliveries (VCDs).2
The safest mode of delivery in case of breech presentation has long been a debate in obstetrics.3 It is recommended to carry out elective caesarean section rather than vaginal delivery for singleton term breech pregnancies when there is fetal distress, macrosomia, footling breech presentation, clinically inadequate maternal pelvis, growth-restricted baby, placenta praevia or fetal anomaly incompatible with vaginal delivery, or if an experienced clinician is absent or the clinician lacks adequate expertise for VBD.4–6 Evidence abounds that unlike VBD for singleton term pregnancies, elective caesarean section reduces perinatal mortality and morbidity, as well as maternal morbidity (urinary incontinence and postpartum perineal pains) in developed countries.7 However, in resource-limited countries, the outcomes of both VBD and elective caesarean breech delivery appear comparable,7 possibly due to the prevailing expertise of birth attendants in VBD in these resource-challenged settings.3 Furthermore, it has been shown that as much as 39 caesarean sections are required to prevent one neonatal death or adverse neonatal outcome in low-income countries compared with seven caesarean sections needed in high-income settings.3 Hence, a health policy generalising the indication of caesarean section to all breech presentations in low-income countries would require significant additional investments in their healthcare systems. Also, the presence of a scarred uterus puts subsequent pregnancies at increased risk of complications such as placenta praevia, placenta accreta and placenta abruption, uterine rupture, repeat caesarean section and repeat breech presentation.6 8–11 Likewise, elective caesarean section for breech presentation cannot be performed in all resource-limited settings due to its financial cost and the prevalent inadequate surgical infrastructure in most health facilities.7
As such, external cephalic version for singleton term pregnancies has been recommended as a safe and cost-effective means to revert breech to cephalic presentation and avert the resort to either VBD or caesarean sections.12 However, external cephalic version is not routinely performed in clinical practice because many health personnel lack its mastery or unduly perceive it to be associated with adverse perinatal outcomes.13 Thus, vaginal delivery is still the main route of delivery in resource-limited environments. Data on VBD for singleton term pregnancies in sub-Saharan Africa is scarce, thus, explaining the lack of consensus on the management of this fetal presentation in the continent. The aim of this study was to elucidate the maternal and neonatal outcomes of vaginal delivery of singleton term fetus in breech presentation following strict selection criteria in a tertiary centre of Cameroon.
Materials and methods
Study design and setting
In this cohort study, we reviewed case notes of all pregnant women at term who had a VBD and pregnant women at term with VCD at the maternity unit of the Yaounde Gynaeco-Obstetric and Paediatric Hospital (YGOPH) between 1 January 2012 and 31 December 2016. The YGOPH is a tertiary hospital located in Yaoundé, the political capital of Cameroon. This health facility serves as a major referral centre for mother and child care in Yaounde and its environs. Its annual number of child births varies between 2000 and 2500 deliveries. The YGOPH is equipped with modern equipment and personnel to provide comprehensive Emergency Obstetric and Neonatal Care services. The maternity unit is managed by 12 obstetricians–gynaecologists and 21 midwives. The hospital has a neonatology unit whose staff comprise 5 paediatricians, 2 general practitioners and 14 nurses.
Participants, sampling and follow-up
The cases were selected based on the guidelines of the Obstetricians and Gynaecologists of Canada,4 the International Federation of Obstetricians and Gynaecology5 and the Royal College of Obstetricians and Gynaecologists.6 Using a ratio of control to cases of 4, a 95% CI, minimum power to detect a difference of 80%, and assuming a minimum OR of 2 for differences to be detected, the formula for difference in proportions14 was used to calculate the minimum sample size. Therefore, the number of VBD required for the study was 41 and the number of controls (VCD) was 164. Each case of VBD of newborn weighing 2500–3500 g was matched for maternal age and parity to four consecutive VCD of newborns weighing 2500–3500 g. We excluded all pregnant women with multiple gestations, footling breech presentation, clinically inadequate maternal pelvis, preterm delivery (less than 37 weeks of gestation), post-term pregnancies (≥41 weeks of gestation) and known cases of fetal demise prior to the onset of labour. Additional exclusion criteria were the presence of a major fetal congenital anomaly (like anencephaly, congenital heart diseases and hydrocephalus), or if there was a contraindication to vaginal delivery such as placenta praevia. In both VBD and VCD groups, we excluded cases of vaginal delivery converted to caesarean delivery. Data was retrieved from case files on important variables in both groups for women and their newborns.
Management of delivery
In this hospital, it is a policy for an experienced obstetrician to be present for every VBD and to augment breech labour only with oxytocin in cases of dynamic dystocia. All deliveries occurred with women lying in the recumbent position with legs in holders. Fetal heart monitoring during labour is done electronically by means of a cardiotocography machine.
Data collection and variables
We identified the records of all women–newborn dyads for term singleton breech deliveries using the delivery registers. Their medical records were then retrieved from the hospital archives for data extraction. The variables studied were:
Maternal demographic data: maternal age, marital status and profession.
Obstetric history: parity and number of antenatal care (ANC) visits.
Details of labour: fetal presentation, fetal heart rhythm, premature rupture of membranes, umbilical cord prolapse, uterine contractions, colour of amniotic fluid, duration of labour, episiotomy, perineal tears, Apgar score at the fifth minute and birth injuries, perinatal deaths.
Postpartum complications: postpartum haemorrhage (PPH), urinary or faecal incontinence in women, and perinatal mortality for newborns.
Definition of terms
Brachial plexus injury was defined as any paralysis of the muscles of the shoulder girdle, arm, forearm of the newborn and occurring after dystocia (difficult childbirth). It was diagnosed by the attending obstetrician or midwife at birth and confirmed by a paediatrician during the first physical examination of the newborn within 24 hours of birth. Birth asphyxia was diagnosed based on the Modified Sarnat-Sarnat Score15 and a 5 min Apgar score ≤3 associated with neurological signs such as hypotonia, coma or convulsions.16 The duration of labour was the estimated time period from 4 cm cervical dilatation to expulsion of the fetus. For all deliveries, this time interval was monitored and recorded on a partogram. Fetal distress was defined as the occurrence of fetal tachycardia (fetal heart beats >160 beats/min) or fetal bradycardia (<110 beats/min).17 PPH was defined as an estimated blood loss greater than 500 mL within 24 hours after vaginal delivery.18
Data management and statistical analysis
Data was entered in Epi Info V.7.1.3.3 software. Comparison of variables between pregnant women who had VBD and VCD was done using the χ2 test or Fisher’s exact test where appropriate. ORs and their corresponding 95% CIs were calculated in order to measure associations. The original alpha value was set at 0.05. In order to reduce the chance of obtaining a type 1 error from the multiple analyses performed on the same dependent variable, Bonferroni-adjusted P values were calculated by dividing the alpha value by the number of comparisons. Hence, any comparison was statistically significant if it was inferior to the Bonferroni-adjusted P value.
Results
Demographic and obstetrical characteristics
During the 5-year review period, a total of 13 695 deliveries were recorded. Among these deliveries, 364 breech deliveries occurred, giving an incidence of 26.6/1000 deliveries. After strict application of our eligibility criteria, we retained the files of 53 women with singleton term VBDs of babies weighing between 2500 and 3500 g (figure 1). Of the 53 VBDs, 12 (22.6%) were unexpected breech births diagnosed during labour and 9 (17%) vaginal breech births required forceps delivery mainly as a result of delayed expulsion of the after-coming head. These women were matched to 212 women with singleton term VCD of newborns weighing between 2500 and 3500 g during the same study period. There were 35 frank breech presentations (66%) and complete breech in 18 cases (34%). The maternal ages ranged from 15 to 45 years and the most frequent age group was 20–30 years (54.7%). Half had attended at least four ANC visits, 54.7% were unemployed and 45.3% were married. Both VBD and VCD groups showed similarities in maternal age, parity, marital and employment status (table 1).
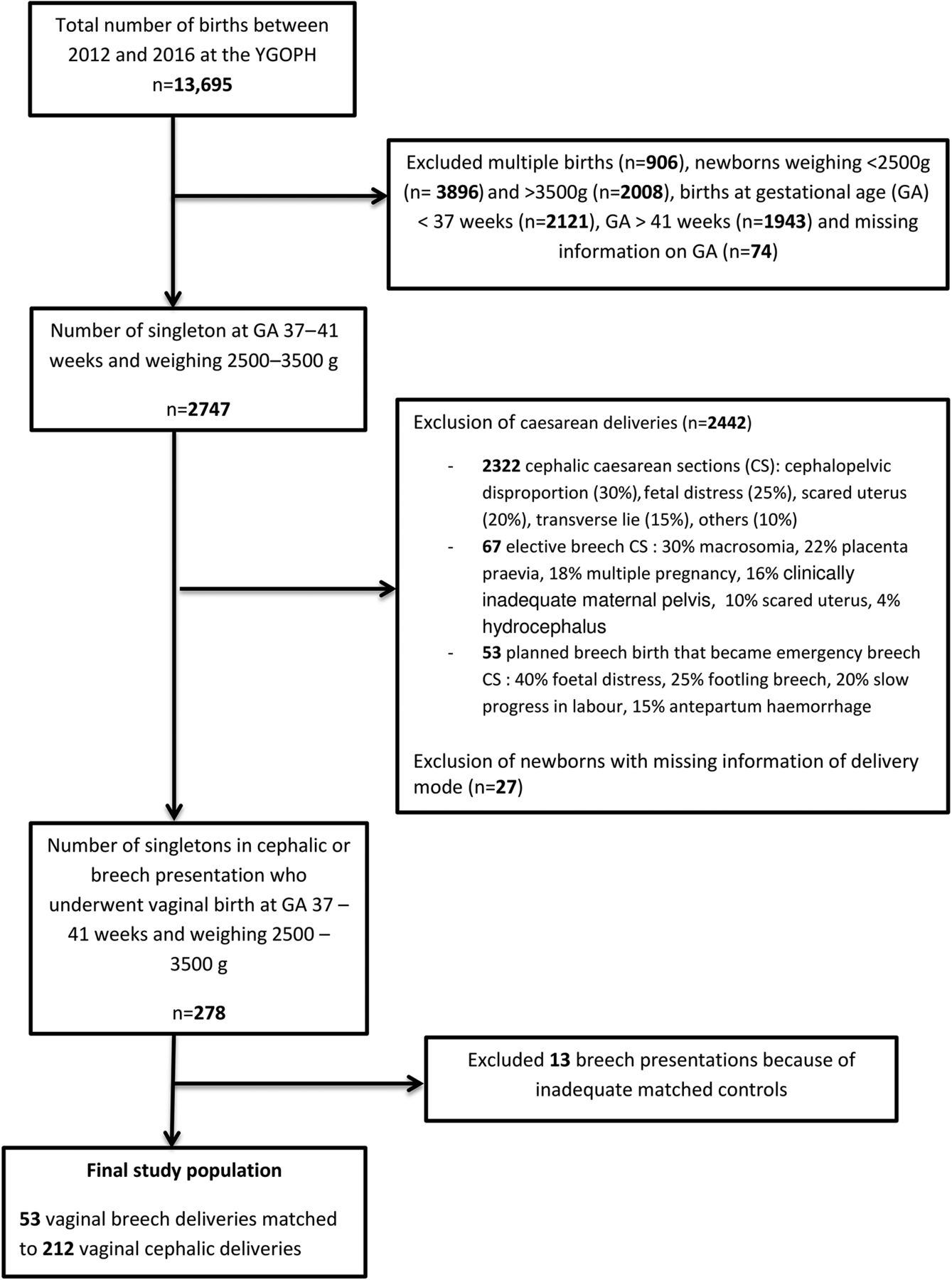
{kind=link}
Flow chart depicting selection of vaginal breech and cephalic delivery cases. YGOPH, Yaounde Gynaeco-Obstetric and Paediatric Hospital.
Sociodemographic characteristics and obstetric history of mothers
Maternal outcomes
Unlike parturients who had VCD, those who underwent VBD were more likely to have prolonged labour (OR 8.05; 95% CI 3.00 to 11.47; P<0.001), premature rupture of membranes (OR 2.14; 95% CI 1.02 to 4.48; P=0.04) and PPH (OR 3.07; 95% CI 1.11 to 8.50; P=0.03). After Bonferroni adjustment (P<0.006), only prolonged labour, meconium-stained amniotic fluid and delivery by a midwife were retained as determinants of adverse maternal outcomes of VBD (table 2).
Maternal outcomes of vaginal breech delivery
Neonatal outcomes
Compared with babies born of VCD, counterparts (VBD group) were more likely to have fetal distress (OR 2.05; 95% CI 1.14 to 3.67; P=0.0153), brachial plexus injury (OR 3.91; 95% CI 2.11 to 7.26; P=0.0262) and about fivefold as likely to suffer from birth asphyxia (OR 4.74; 95% CI 3.09 to 7.26; P<0.001). Only birth asphyxia was retained as an adverse neonatal outcome after Bonferroni correction (P<0.0125) (table 3).
Analysis of neonatal outcomes associated with vaginal breech delivery
Discussion
This study aimed at determining the maternal and neonatal outcomes of VBD for singleton term pregnancies in a tertiary mother and child hospital in Yaounde, Cameroon. Despite the application of the aforementioned guidelines,4–6 VBD was found to be significantly associated with prolonged labour (OR 8.05; 95% CI 3.00 to 11.47; P<0.001) and birth asphyxia (OR 10.24; 95% CI 4.92 to 21.31; P<0.001). This observation could be the result of the high incidence of dystocia associated with this presentation.19
The findings indicate that the perinatal mortality in VBD was comparable to that of VCD (2% vs 0%; P=0.2). This may be attributed to the fact that the study was carried out in referral hospital with an experienced obstetric team and with means of electronic fetal monitoring (cardiotocography) to timely detect warning signs of non-reassuring fetal status during vaginal breech birth. These results are consistent with the studies reporting no difference in the perinatal mortality following breech delivery in resource-limited settings.20 21 On the other hand, Kemfang Ngowa et al 22 in a similar study setting in Cameroon reported a significant perinatal mortality (P<0.01) for breech deliveries, which could be due to the absence of well-defined selection criteria for VBD in their series. Their observed perinatal mortality was in cases of macrosomia, nuchal extension, dystocic labour and placental abruption, which were all excluded in the current cohort.
Neonates delivered through breech birth were more likely to have birth asphyxia than those who had a vaginal cephalic birth (47% vs 8%; P<0.001), corroborating previous studies from both high-income3 23 and low-income settings.20 21 24 This could be related to the fact that breech fetuses are predisposed to an increased risk of hypoxic–anoxic events from head entrapment, rapid decompression of the head and other birth trauma.7
The main limitation of this study was that being a retrospective study, data collection was subject to the potential risk of reviewing incorrectly completed records. Furthermore, less than four ANC visits were attended in 68% of VBD compared with 43% of VCD studied (P=0.002). ANC attendance was not a matching variable between the VBD and VCD groups. Hence, the VBD cases were a higher-risk group from the onset of the study and 22.6% of VBD were unrecognised before the onset of labour. Also, the study was conducted in an urban centre with standards of a tertiary level of care, which implies cautious generalisation of our results to health facilities not having the same level of care. Nevertheless, based on careful selection criteria of singleton term VBD and the statistical analysis used to eliminate bias, we reviewed a 5-year period to assess the outcomes of VBD in a low-income country where caesarean delivery cannot be generalised as the mode of delivery for all breech presentations because of its financial cost and the prevalent inadequate surgical infrastructure in most health facilities. The findings are a significant contribution to the ongoing debate on the safety of VBD in sub-Saharan Africa.
Conclusion
The findings suggest that even when breech delivery guidelines are applied, VBD of singleton term pregnancies is still associated with a high incidence of maternal and perinatal morbidity. This finding does not discount the role of VBD in resource-poor settings, but emphasises the need for rigorous monitoring of labour, timely decision and adequate anticipation for neonatal resuscitation in order to reduce these complications. Also, external cephalic version should be practised and promoted in this resource-limited setting as a means to convert breech to cephalic presentations and reduce the perinatal and maternal morbidities associated with VBD. Refresher courses for the management of breech birth should be organised for health personnel in order to minimise risk of brachial plexus injury. Based on the limitations of the study, there is a need to carry out large multicentre clinical trials in our resource-limited settings.
Acknowledgments
The authors express their gratitude to the administrative authorities of the Yaounde Gynaeco-Obstetric and Paediatric Hospital for granting them permission to conduct this study.
References
Footnotes
Contributors JSD, PF and EM: study conception and design, acquisition of data, data analysis and interpretation, manuscript writing and critical revisions. FM: study conception and design, acquisition of data, data analysis and interpretation, and manuscript writing. JNT, MNT, RT and VA: acquisition of data, data analysis and interpretation, manuscript writing and revisions. All authors read and approved the final manuscript.
Competing interests None declared.
Ethics approval This study was approved by the Institutional Review Board of the Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Yaounde, Cameroon.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.