Article Text

Abstract
This paper is a record of the UK Defence Medical Services (DMS) contribution to the UK response to the Ebola crisis in West Africa from the start of planning in July 2014 to the closure of the Ministry of Defence Ebola Virus Disease Treatment Unit at the end of June 2015. The context and wider UK government decisions are summarised. This paper describes the decisions and processes that resulted in the deployment of a DMS delivered Ebola Treatment Unit in conjunction with the Department for International Development and Save the Children. It covers arrangements for medical care for disease and non-battle injury, the Air Transportable Isolator and Force Health Protection policy, and finally, considers the medical lessons from this deployment. The core message is that the UK DMS are the only part of the UK health sector that is trained, equipped, manned and available to rapidly deploy and operate a complete medical unit as part of an international response to a health crisis.
- PUBLIC HEALTH
Statistics from Altmetric.com
Key messages
The Defence Medical Services’ contribution to the UK response to the Ebola crisis was a major deployment of military medical capability, covering Role 1–3 capabilities.
The Defence Medical Services designed, organised, trained and deployed an Ebola Treatment Unit as an inter-agency, a multinational medical unit within the UK national response to the Ebola crisis.
The Defence Medical Services also trained a significant number of Sierra Leonean healthcare workers, provided disease and non-battle injury medical support and operated the Air Transportable Isolator for strategic medical evacuation.
This operation showed the organisational competence of the Defence Medical Services to adapt to completely new medical challenges and deploy medical units trained for this new mission.
Introduction
This paper is a record of the UK Defence Medical Services’ (DMS) contribution to the UK response to the Ebola crisis in West Africa from the start of planning in July 2014 through to the closure of the Ministry of Defence (MOD) Ebola Virus Disease Treatment Unit (EVD TU) at the end of June 2015. It presents neither the clinical results nor the Force Health Protection (FHP) measures taken, which will be reported separately. The DMS contribution was nested into the wider MOD mission which was part of the UK cross-government crisis planning involving the Foreign Office, the Department for International Development (DFID), the Department of Health (DoH), the Home Office, the Department for Transport and the devolved administrations and was known as Op GRITROCK. This response was predicated on reducing the risk of Ebola being imported into the UK, establishing a response if a case of Ebola arrived in the UK, and making a significant contribution to the international response to the global crisis. The outbreak originated in Guinea and rapidly spread to neighbouring countries and as the international response emerged, the UK took the lead in supporting Sierra Leone with the USA undertaking the same for Liberia and France covering Guinea.
Initial planning
Early estimates of the epidemic suggested case numbers were doubling every 30 days. This was assessed to be a significant risk of transmission beyond the immediately affected countries into the wider African continent and the inter-connectivity of international air travel posed a significant risk of global transmission.
Initial UK Governmental efforts were focussed on establishing border entry screening for passengers from at risk countries and supporting African countries to establish exit screening procedures for air travellers; this risk was reduced when most airlines cancelled services to and from the affected countries. Point of entry screening was established by Public Health England (PHE) in support of the Border Agency and the DMS were closely involved in these discussions, particularly over the application of the policies in regard to MoD healthcare workers returning from supporting the Ebola response. A key early decision was to apply the ‘precautionary principle’ rather than ‘as low as reasonably practicable’ and to exclude healthcare workers involved in caring for Ebola victims from clinical work for 21 days after their last exposure in order to maintain public confidence that there was no risk of contagion in NHS hospitals.
It was clear from the outset that controlling the Ebola epidemic could only be achieved through population-level public health measures in the affected countries, which would require a co-ordinated international response as all three countries were among the poorest in the world with already fragile health systems. There were a high number of cases of Ebola among healthcare workers, principally those that were working in Ebola-facing healthcare facilities highlighting inadequate infection-control practices. Cases needed to be identified, isolated and treated with close contacts quarantined and burial of the dead done in a safe and dignified manner, which would require a command and control capability not present in Sierra Leone. Establishing this capability became the priority closely followed by the requirement to expand isolation and treatment capacity to remove infected cases from the community, mobilise the public to present themselves if symptomatic and to adopt safe burial practices, which proved to be one of the biggest challenges as the requirement to ensure the rites of the dead were carried out according to cultural practice is deep seated in the Sierra Leonean psyche.
With no intrinsic healthcare resilience, there would need to be a surge of international volunteers to support the government and health systems with the presumed significant risk of transmission of Ebola to these volunteers. This was compounded by the fact that there were a small number of infectious disease containment beds in the UK, and the UK MOD was the only organisation with the ability to safely conduct aeromedical evacuation of Ebola cases. In the early stages of planning, the government's medical advice was to retain Ebola cases in the country to reduce the risk of transmission in the UK. It was also agreed that this would require the best available hospital services to be deployed to provide reassurance to volunteers and their families that they would receive care at the standard comparable to that which would be delivered in the UK.
Based on this analysis, DFID committed to a six-point action plan to defeat Ebola in Sierra Leone: command and control, treatment centres, training international and national health workers, healthcare for international staff, infection control services and co-ordination of international donations.1
While not usually the preferred choice for humanitarian response, the MOD provided DFID with a range of rapidly deployable capabilities that could be guaranteed without the risk of volunteer staff withdrawing due to the threat. The MOD would provide the earliest effect and catalyst for the mobilisation of the international community to deliver detailed technical expertise and the expansion of national and international capacity to bring the crisis under control. The tactical MOD response was initially led by 104 Logistic Brigade and nested into the Combined Joint Inter-Agency Task Force (CJIATF). This was built around the Provincial Reconstruction Team model from Afghanistan and was led by a senior official from DFID. The CJIATF had a specific medical branch with a senior-ranked Commander Medical (Comd Med) to reflect the centrality of the health and medical function in delivering the MOD mission. The initial Comd Med had extensive prior experience in Sierra Leone that proved invaluable in forming early relationships with key medical opinion leaders. Subsequent Comds Med have had a specific education in public health or health services management.
The DMS strategic contribution was co-ordinated by the Medical Operations and Capability (MedOpCap) team, reinforced with planning and public health expertise, working to the Operations Directorate in the MOD. The medical intelligence function within Defence Intelligence was also reinforced which proved to be of special value in the co-ordination of a cross-government common medical intelligence and epidemiology picture. A regular medical operations video teleconference was established for operations and video teleconference were established to ensure unity of medical advice across the DMS enterprise to support the chain of command. There was an early acknowledgement that there should be a strong medical voice as part of the military-planning process as this was a public health crisis rather than the usual DMS role of providing medical support to a military plan. This was especially important in the cross-government meetings where only the DMS representatives had practical experience of the force generation and the deployment and operation of medical units. As the plan matured, it became evident that DMS would be acting in the same way as other implementing partners, which required an agreed mechanism for DFID to reimburse the MOD for the direct costs of this operation.
The organisational design for the international worker EVD TU was the central, early challenge. Using MOD personnel was fundamentally different from seeking volunteers, as individuals were to be ordered to deploy, and would be directly involved in clinical care of Ebola patients and would remain subject to military law. The Surgeon General explicitly considered and supported this as a lawful order. In doing so, it was acknowledged that the MOD had responsibilities as an employer to ensure that any risks to health and safety were fully assessed, mitigated and any residual risk managed to be as low as reasonably practicable; in view of this, the DMS did not wish to deploy more personnel than absolutely essential to achieve the mission. Concurrently, DFID sought an implementing partner to deliver an Ebola Treatment Centre (ETC) to increase Sierra Leonian capacity. The government of Sierra Leone offered a location near Kerrytown, 19 miles from the capital, Freetown, with Save the Children (StC) the only organisation willing to support the DFID plan. The initial plan had StC acting as a managing agent for the Kerrytown site and running an 80-bed ETC (initially using the Medicins sans Frontiers (MSF) ‘symptomatic’ treatment approach of oral rehydration and paracetamol), PHE and the MOD jointly running a public health and diagnostic laboratory and the DMS (22 Field Hospital) running a high-level EVD TU to manage infected healthcare workers (HCWs). The goal for deploying the EVD TU was to demonstrably deliver a level of care to infected healthcare workers and other entitled patients as close as safely practicable to that provided in Western national infectious disease containment facilities.
As the Ebola outbreak developed, the non-Ebola facing health economy of Sierra Leone collapsed resulting in a gap for clinical care for non-Ebola disease and non-battle injuries (DNBI). Most Sierra Leone hospitals stopped conducting invasive clinical procedures such as surgery, meaning that the international community did not have adequate hospital cover from the onset of the Ebola crisis until mid-2015 when most hospital facilities started to return to normal service. Once the decision had been made to commit MOD personnel, the MOD became liable for the provision of medical support to its personnel and, through requests from DFID and the Foreign and Commonwealth Office (FCO), all international personnel supporting the UK effort and UN personnel committed to the Ebola campaign. Thus, a deployed medical system was specifically designed covering pre-hospital care (FHP, primary care, medical evacuation) and deployed hospital care (DHC) for entitled individuals. The initial DHC plan established a small facility in adapted barrack accommodation designated Role 2 Ashore. After it was decided to deploy the Royal Fleet Auxiliary (RFA) Argus with helicopters and assault boats for its mobility support capabilities, it was agreed that the Primary Casualty Receiving Facility on board should be activated as this would represent an opportunity to deliver the highest quality of clinical capability and infrastructure in support of the CJIATF population at risk.
Force Generation of the EVD TU
The Force Generation of the EVD TU highlighted the value of deep organisational learning achieved in the DMS through a decade of deploying hospitals in Afghanistan. The DMS already had a specialist registrar on secondment to the World Health Organization who had been working in the region as part of the initial Ebola response, and who had specific technical knowledge of the operation of ETCs and the critical importance of tight infection prevention and control procedures. A planning team established the organisational design and personnel requirements for the EVD TU and to build liaison with StC and DFID for all aspects of Kerrytown operations. A Memorandum of Understanding was developed for all parties that reflected the previous DMS experience of running multinational medical units in operation. DFID took responsibility for procuring equipment for the EVD TU which required the development of a specific medical equipment schedule to reflect the additional clinical interventions that the EVD TU would offer above the basic supportive care provided in ETCs. This bespoke equipment schedule would be essential in dealing with supply issues that were to develop as the EVD TU, in DFID logistic terms, was a small part of its operation but with the most complex equipment needs.
The training team at the Army Medical Services Field Training Centre (AMSTC), Strensall, developed a package of individual training for the use of personal protective equipment (PPE) and built a simulation of the planned EVD TU to enable collective training for all personnel. Senior members of staff identified to deploy from the UK military hospital and staff from AMSTC collaborated with PHE infectious disease experts and the National Ambulance Resilience Unit to procure the most appropriate PPE ensemble, define donning and doffing drills and establish processes for working in a high-risk zone in PPE. The ‘safe system of work’ designed to control risks of contamination to clinical personnel by Ebola virus was more akin to the planning for a ‘spacewalk’. This involved pre-task planning and rehearsals, gowning up, buddy monitoring of PPE during the mission, recovery, de-gowning and disinfection and post-task debriefing. A system of closed circuit television (CCTV) monitoring was developed to complement the use of PPE buddies for all staff in the ‘Red Zone’. This CCTV system and the use of electronic transfer of photographed images of patients’ records by Bluetooth from the ‘Red Zone’ were deployed to Sierra Leone as a means of reducing the risk of exposure of clinical staff to Ebola. Building on the major trauma data collection record for the Joint Theatre Trauma Registry, the Medical Directorate developed a specific Ebola patient Medical Assessment Form to enable the collation of clinical data for all patients treated. The senior clinicians developed clinical protocols for the management of Ebola, specifically deciding to add central venous access as a clinical intervention to reduce the risk of needlestick injury or blood contamination to clinical staff.
Advice was taken throughout the training development process from UK and international experts to ensure that the DMS was exploiting the best available evidence including the consideration of ethical issues such as the balance between clinician safety and maximal clinical intervention. After the first rotation of clinical personnel through this training system, cross-government partners concluded that no other healthcare organisation in the UK would have had the organisational knowledge to develop such a mobilisation pathway for a medical unit against such challenging timelines. AMSTC also ran the pre-deployment clinical training for the first cohort of healthcare workers mobilised from the NHS and ran a train-the-trainer course to enable UK Med to take over the pre-deployment training for subsequent cohorts of NHS volunteers. Overall, there were only 6 weeks between the issue of the Activation Order by the MOD to the admission of the first patient into the EVD TU in Sierra Leone.
Initial implementation of the plan
The first planning team, including the Comd Med, deployed to Sierra Leone in September 2014. The early conclusion was that the government of Sierra Leone needed considerable assistance in establishing a cross-government crisis planning system. The UK actively supported the creation of a National Ebola Response Centre and supporting District Ebola Response Centres. Military and international staff provided mentoring and staff support to key personnel to lead these organisations. It was also clear that a massive expansion of national capacity to handle Ebola victims was required, and this needed the rapid creation of a system for PPE training. At very short notice, 5 Armoured Medical Regiment were tasked to develop a training system and train-the-trainer package for the use of WHO-approved PPE and then to deploy to Sierra Leone to set up an Ebola Training Academy pending handover to a non-government organisation (NGO) contracted by DFID. The unit received the warning order to deploy at the end of September 2014, deployed on 21 October 2014 and accepted the first student a week later (Figure 1). By the time of handover at the beginning of December 2014 to the International Organisation for Migration (IOM), the unit had trained over 4000 local personnel in the safe use of PPE to protect against Ebola,2 with an unforeseen element of added value in that many of them, in their end of course feedback, said that they would be applying much of what they had learnt in terms of Ebola awareness in their local communities. This saw a considerable potential enhancement to the social mobilisation operations designed to influence community actions against Ebola.

Personnel from 5 Armoured Medical Regiment training Sierra Leoneans in the use of personal protective equipment against Ebola.
In addition to headquarters personnel, the CJIATF included a number of Specialist Teams Royal Engineers who provided design and contract oversight for the building of the ETCs commissioned by DFID. The Kerrytown site was completed first and was ready for occupation by the end of October 2014; its development was complex and served as an important proving ground in the design and build of subsequent ETCs with several lessons learnt and subsequently incorporated. For example, the Kerrytown unit was built using timber frame, polythene walls and corrugated roofing, whereas subsequent treatment centres used more durable materials. The early design for the Kerrytown site had originally been a square allowing for more efficient staff and patient circulation, however, as a result of Sierra Leonean Government pressure to develop the site quickly, a linear design was selected leading to some significant issues in terms of staff and patient circulation (Figure 2). Later iterations delivered a more ergonomically efficient plan. The DMS team for the EVD TU had had the benefit of collective training pre-deployment and were able to undertake final mission rehearsals in full PPE immediately after arriving and taking over their part of the site; as a result, the unit was ready to receive their first patients as soon as the site was declared operational. The StC team was formed in Sierra Leone and included the complexity of local staff and international personnel from countries whose native language was not English, which led to some early operating difficulties. The DMS EVD TU senior leadership provided technical assistance and clinical support to the StC to enable them to achieve full operating capability by the middle of November 2014.

Overhead photo and layout of the Kerrytown site. MOD, Ministry of Defence; StC, Save the Children.
It was evident that the small number of beds available in the EVD TU would mean that Comd Med would require guidance on the criteria for admission, by Medical Rules of Eligibility (MRoE),3 a concept familiar to the military medical community but new to the humanitarian community. MRoE aims to protect medical capacity for the primary mission of supporting the military operation while meeting obligations under international and humanitarian law. The MRoE covered the international community deployed in support of the wider Ebola crisis, which included those facilities contracted under DFID and other international healthcare workers employed in ETCs. The eligibility criteria allowed Comd Med the discretion to accept admissions for Sierra Leonean healthcare workers within capacity. The Comd Med was also authorised to accept other admissions to enable the EVD TU personnel to establish procedures and protocols based on actual clinical exposure. This was a careful balance as local patients tended to be admitted in the more severe stages of the disease which is both much more infectious but with a substantially lower chance of survival and consequent higher risk of exposure for healthcare workers employed in the Kerrytown Treatment Unit (KTTU) Red Zone.
Steady-state and transition
Pre-hospital care was organised on a standard laydown of combat medical technicians supporting small detachments and general duties medical officers base in isolated and larger detachments, overseen by a general practitioner as the CJIATF senior medical officer. The Irish Defence Force contributed key personnel as part of the UK-led multinational prehospital care system. All significant moves of personnel were accompanied by a medic as there was no local ambulance service. The Merlin helicopters on board RFA Argus provided a Maritime In-transit Care response at 30 min notice to move to respond to emergencies (most likely to be a road traffic collision). One major success was the first hosting of the Defence Medical Information Capability Programme medical information system on the theatre information network, HOUSEKEEPER, which allowed regular synchronisation of military electronic patient records between Sierra Leone and the UK.
The EVD TU quickly established itself as a high-quality Ebola medical facility in Sierra Leone. The facility became a multinational medical unit from the second rotation with the incorporation of personnel from the Canadian Armed Forces Medical Services. This proved providing tangible evidence of the significant international reputation of the UK DMS arising from the successful leadership of multinational medical units since the Balkans operations in the 1990s. The Defence Reform Act 2014 enabled DMS Reservists to volunteer for this operation and the first Reserve clinical personnel deployed in December 2014 with 30 medical Reserves eventually being mobilised.
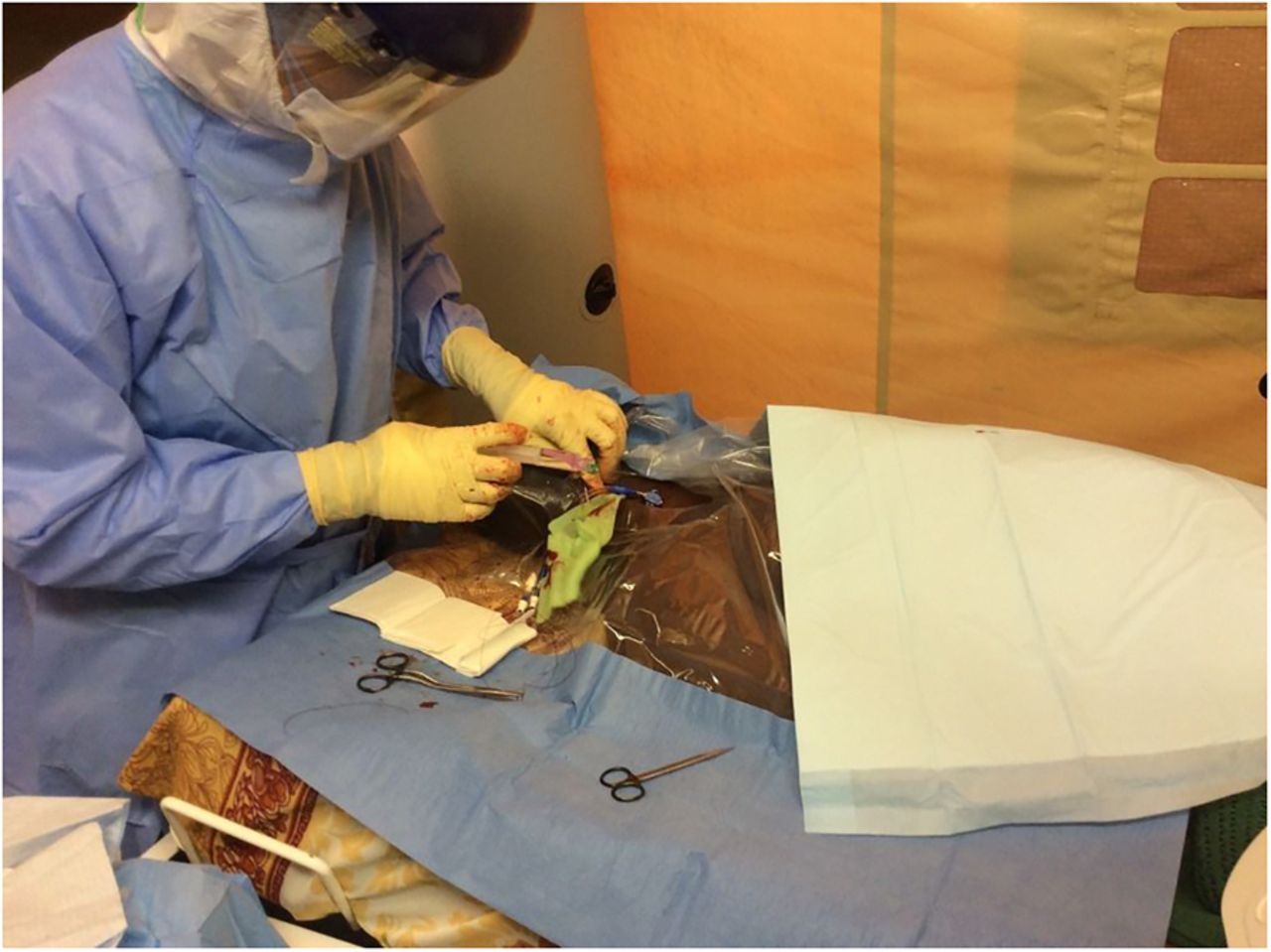
Among UK MoD healthcare workers, there were two needlestick injuries, one from venepuncture and one from an unidentified discarded needle that was found during deep cleaning. One DMS nurse contracted Ebola. This event also directly generated four high-risk exposures. All of these were regarded as significant events and detailed root cause analyses (RCA) involving CJIATF and PHE experts were undertaken to identify all possible measures to reduce the risk of such events being repeated. It was not possible to identify the exposure event that caused the Ebola case, but the RCA emphasised the value of the detailed record keeping associated with operating in the Red Zone and that advanced governance systems were already in place. Figure 3 shows an image of the clinical environment in the ‘Red Zone’.

Clinical care in the Red Zone.
Healthcare governance in theatre was established as a priority with a particular focus on EVD TU practices with every breach of policy and process being deemed a significant event, allowing adverse trends to be identified and remedied quickly. The most frequently reported events were minor breaches of PPE due to snagging in the high-risk zone. However, as exposed nails were either removed or covered by bubble wrap with black and yellow warning tape to alert personnel to enduring snagging risks, the number of PPE breaches reduced.
The weekly Joint Theatre Clinical Case Conference4 continued to act as the critical forum for clinical co-ordination and guidance from the Medical Director and the Defence Consultant Advisers to deployed clinicians, providing the tight feedback loop for rapid clinical organisational learning and feeding directly into the clinical training of the subsequent rotations of clinical personnel. It provided a forum to link global innovations in clinical care directly to practice in the EVD TU. Particular examples included approval for both the use of an experimental Canadian vaccine and the introduction of famciclovir as postexposure prophylaxis for Ebola cases. As the Ebola epidemic came under control, the likelihood of Ebola being the cause of the clinical case definition reduced and other infectious diseases took equal relative importance. It was found that many local patients had comorbidities such as malaria or HIV. The majority of international healthcare workers treated at the EVD TU since its opening were also subsequently diagnosed with other conditions. The DMS component of the Kerrytown laboratory included the first deployment for contingent operations of the Biofire Film Array PCR diagnostic machine; this was a particular benefit when identifying non-Ebola causes of fever which allowed a tiered risk assessment for pyrexia of unknown origin to be introduced which reduced the risk of an unnecessary admission to the EVD TU.
The RFA Argus left Sierra Leonian waters at the end of March 2015, after a light clinical workload but the reassurance effect of the facility was widely recognised to have been an important ‘moral component’ to the effectiveness of the international community.5 The capability and capacity of the Role 2 Ashore was increased to minimise the reduction in the standard of clinical care available. The most challenging decision was the timing of the closure of this facility in light of the significant clinical weaknesses of the local health system. This required an acceptance of the risks associated with this decision with an acknowledgement that it cannot be appropriate for the DMS to represent the majority of a military deployment just to provide medical care for the personnel deployed. For the longer term the DMS will need to consider how to adjust to the function of a cross-governmental ‘medical insurance policy’ and may need to consider the use of high fidelity simulation or other educational techniques to maintain individual and collective clinical skills during periods of low patient throughput in order to maintain clinical performance.
The transformation of the Ebola epidemiological picture from over 200 new cases per day in December 2014 to less than 50 per week by the end of March 2015 and low teens by early April 2015 was truly remarkable and testament to the success of the mobilisation of Sierra Leonean society supported by the international community. The EVD TU capacity was surged to 20 beds for January to February 2015, reduced to 12 beds for March and April and then further reduced to eight beds from May 2015. Fortunately the predicted demand from Ebola-affected healthcare workers did not materialise. The governments of international healthcare workers changed the initial paradigm by arranging aeromedical evacuation for all high-risk Ebola exposure cases plus all diagnosed Ebola patients. This resulted in a changed function to that of rapid diagnosis and aeromedical staging with a short period of stay for international healthcare workers in the EVD TU. It is notable that the EVD TU treated three confirmed positive international healthcare workers, which included the one UK military healthcare worker. Sierra Leonean Ebola cases were important to enable the development of clinical protocols and procedures but became less relevant when the overall ETC capacity was sufficient for all indigenous cases.
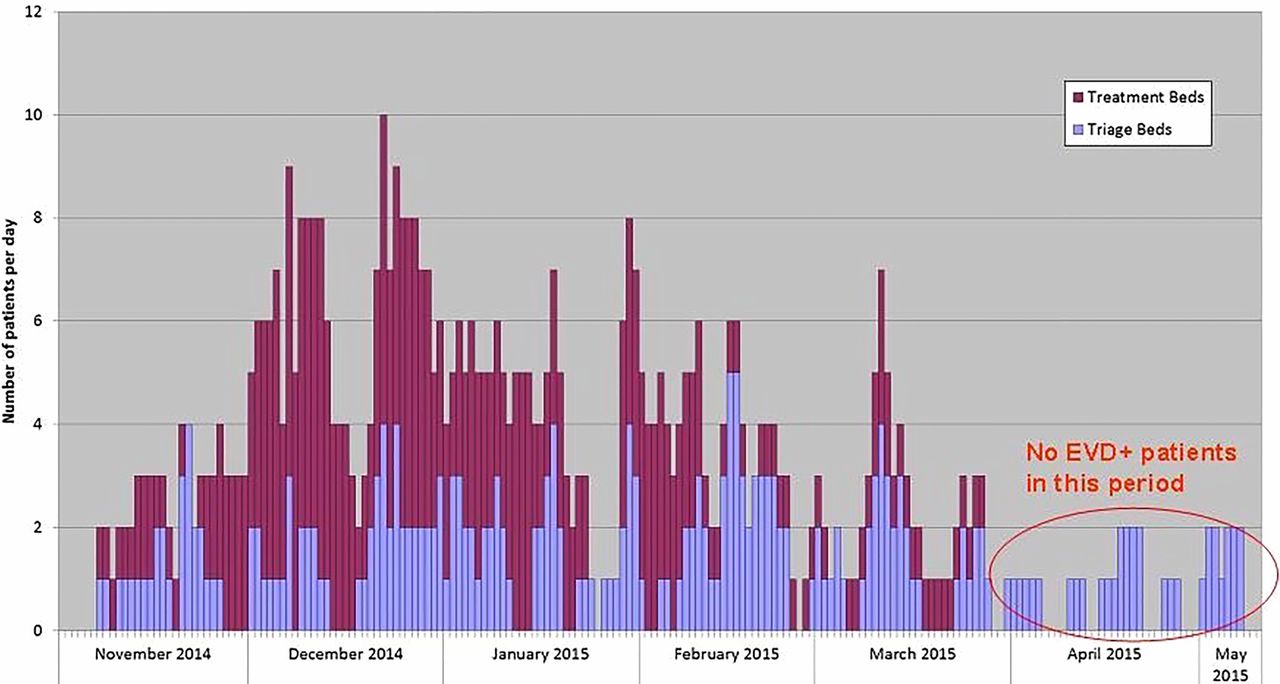
A summary of the clinical workload against the capacity of the EVD TU during its period of operation is shown in Figure 4. All patients meeting the clinical definition for Ebola were initially admitted to triage beds pending laboratory confirmation of diagnosis when they were then admitted to a treatment bed. Overall, there were 21 EVD discharges, 19 EVD deaths, 76 non-EVD discharges, 1 non-EVD death and 3 international EVD cases aeromedically evacuated from Sierra Leone.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kerrytown Ebola Virus Disease Treatment Unit bed occupancy. Patients that occupied both types of bed on the same day are double counted. No more than four triage beds were occupied at any one time, but they were re-used throughout the day as patients spent only a few hours in a triage bed. EVD, Ebola Virus Disease.
Strategic aeromedical evacuation
The RAF Medical Services holds an Air Transportable Isolator (ATI) capability at readiness as a UK national capability. Initially developed in the 1970s, this was one of a few aeromedical evacuation systems for Ebola patients available across the globe. It was designed to enable the safe aeromedical transfer of a clinically stable, highly infective patient in an isolation ‘bubble’ to a receiving hospital in the UK. The MOD has a standing agreement with the DoH for the ATI to be used for non-military patients with the Royal Free Hospital as the receiving hospital of choice. The detailed procedures for the transfer of highly infective patients from the MOD ATI to the NHS (including the use of other receiving hospitals) were refreshed and rehearsed. The MOD procured additional ATI systems and the RAF stood up additional ATI escort teams based on an early assessment of likely demand for ATI capability. An ATI was first used to recover the first UK national case from Sierra Leone on 24 August 2015 and then to move a UK NHS healthcare worker from Glasgow to London when she developed symptoms of Ebola after returning from Sierra Leone at the end of December 2014. It was used on several aeromedical evacuation missions in 2015 when it was considered prudent to escort individuals with high-risk Ebola exposures in a C17 aeroplane equipped with an ATI due to the possibility of the individual developing Ebola symptoms during flight and requiring immediate isolation to protect the escorting aircrew.
Force Health Protection
FHP has been a critical function of the DMS from providing advice to senior personnel and Ministers on health risks associated with deployment, down to the introduction and monitoring of antimalarial and antigastrointestinal disease measures. A full description of the FHP aspects of this operation will be published separately. It was decided at the outset that the MoD would comply with national guidance for Ebola issued by PHE. The DMS established early co-ordination with PHE to ensure that the MOD complied with ‘port of entry’ procedures established for the UK including screening upon arrival into a military port of entry and a tracking system for MOD personnel after their return to the UK.
The DMS has extensive knowledge of the DNBI threat in West Africa and instituted standard risk control and mitigation measures through the publication of specific guidance in the Permanent Joint Headquarters (PJHQ) Medical Directive and a centrally controlled standard pre-deployment briefing package. Specific attention was paid to ensuring authoritative advice on antimalarial prophylaxis. It was clear that there would be considerable scrutiny of the FHP system and a Defence FHP Board was established under the chairmanship of Hd MedOpCap to draw together all stakeholders in the FHP system. Early activity concentrated on the risk assessment and mitigation of the three classes of health threats including audits of all aspects of implementation of control measures. The Defence Public Health Unit established a patient registry of all UK MOD hospital admissions in the UK attributable to Op GRITROCK. The FHP Board provided governance of the MOD ‘port of entry’ screening and oversaw the management of the investigation of the disease outbreaks and Ebola-related significant events; it also reviewed the reporting of Significant Events and provided assurance through the DMS Inspector General that the end-to-end process for healthcare on Op GRITROCK was being properly managed
Overall observations and lessons
As reported by the Commander of 104 Logistic Brigade, the DMS contribution to Op GRITROCK played an essential role in supporting the ‘moral component’ of the international response.6 While not necessarily the first choice for responding to international health emergencies, the DMS is the only part of the UK health sector than can respond in the tight timescales required, adapt to a completely new clinical challenge and deliver a rapidly deployable clinical capability that is collectively trained as a team and operates under a direct command system.
The organisational learning accrued by the DMS during the last decade to develop the world class trauma system translated into the deep competence that provided the foundations to develop a medical system for this mission.7 This was underpinned by the willingness of the Reserves, and Canadian and Irish military partners, to contribute to multinational medical capability under UK Regular DMS leadership. The DMS expertise translated into an effective collaboration with StC for the operation of the Kerrytown site and the hand-off of training systems for PPE training to IOM and healthcare worker training to UK-Med. The whole institutional mobilisation system for the DMS must be nurtured to endure.
The existing DMS relationships across the NHS at levels of seniority far above our organisational size proved invaluable in influencing and co-ordinating with DoH and PHE policies and procedures. This network of influence must be maintained.
The military approach to FHP was a demonstration of the duty of care to DMS employees and seemed to exceed the organisational systems within other partners.8 This is a fragile capability that relies on a small number of deep subject matter experts. The sustainability of this enterprise will need further examination to ensure that the DMS maintains the institutional knowledge to deliver FHP for the many deployments of the Armed Forces across the globe.
The pace of deployment and the austerity of the locations for many personnel showed that the DMS must maintain the appropriate balance between clinical and military skills for its personnel. Placements in the NHS are essential to maintain clinical expertise but time must also be found to ensure DMS personnel are trained on in-service military medical equipment and know how to function as individuals and teams in austere environments. This may include training in extended clinical skills not usually undertaken by junior clinical staff.
Footnotes
Collaborators Colonel Andrew Terrell L/RAMC, Head Defence Public Health Unit, HQ Surgeon General, Coltman House, DMS Whittington, Whittington Barracks, Lichfield, Staffordshire WS14 9PY, UK. Colonel Jeremy Tuck CBE L/RAMC, Commander Medical CJIATF, OP GRITROCK 1, Now at: HQ Surgeon General, Ministry of Defence, 6.E.08, Main Building, Whitehall, London SW1A 2HB, UK. Colonel Patrick John L/RAMC, Commander Medical CJIATF, OP GRITROCK 2, Now at: HQ Support Command, Steeles Road, Aldershot, Hampshire GU11 2DP, UK.
Contributors MB was the primary author and guarantor. The remaining authors all had significant roles in the events described, provided text for the article and reviewed the final version.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.