Article Text

Abstract
Introduction Water fetching for household needs can cause injury, but documentation of the burden of harm globally has been limited. We described the frequency, characteristics and correlates of water-fetching injuries in 24 sites in 21 low-income and middle-income countries in Asia, Africa and Latin America and the Caribbean.
Methods In a survey of 6291 randomly selected households, respondents reported whether and how they had experienced water-fetching injuries. Responses were coded for injury type, mechanism, bodily location and physical context. We then identified correlates of injury using a multilevel, mixed-effects logistic regression model.
Results Thirteen per cent of respondents reported at least one water-fetching injury. Of 879 injuries, fractures and dislocations were the most commonly specified type (29.2%), and falls were the most commonly specified mechanism (76.4%). Where specified, 61.1% of injuries occurred to the lower limbs, and dangerous terrain (69.4%) was the most frequently reported context. Significant correlates included being female (aOR=1.50, 95% CI 1.15 to 1.96); rural (aOR=4.80, 95% CI 2.83 to 8.15) or periurban residence (aOR=2.75, 95% CI 1.64 to 4.60); higher household water insecurity scores (aOR=1.09, 95% CI 1.07 to 1.10) and reliance on surface water (aOR=1.97, 95% CI 1.21 to 3.22) or off-premise water sources that required queueing (aOR=1.72, 95% CI 1.19 to 2.49).
Conclusion These data suggest that water-fetching injuries are an underappreciated and largely unmeasured public health challenge. We offer guidelines for comprehensive data collection on injuries to better capture the true burden of inadequate water access. Such data can guide the design of interventions to reduce injury risk and promote equitable water access solutions.
- maternal health
- public health
- injury
- cross-sectional survey
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Water fetching has been associated with pain, fatigue and perinatal health problems, and is likely a major contributing factor to musculoskeletal disease burden globally.
Systematic documentation of water-fetching injuries has been limited, and experts have recommended empirical analyses of factors that could help explain such injuries.
What are the new findings?
Of 6291 households across 24 sites in 21 low-income and middle-income countries, 13% reported one or more water-fetching injuries.
Significant correlates of water-fetching injuries included being female, rural or periurban residence, higher household water insecurity scores, use of off-premise water sources that increase distance and/or queueing time, and increased time spent collecting water.
What do the new findings imply?
The current global water, sanitation and hygiene (WaSH) burden is likely being underestimated, such that we propose items for systematic data collection on water-fetching injury type, mechanism of injury, bodily location and physical context of injury.
Future research should explore the links between water-fetching injuries and diverse health and well-being outcomes.
Progress towards Sustainable Development Goal 6.1 should include measures of physical safety in addition to traditional WaSH indicators of improved water quality and source proximity.
Introduction
Access to water is essential for ensuring water security, food security, public health, gender equity and economic development.1–5 While access to improved water sources has increased globally,6 millions of individuals must still fetch water every day to meet household needs when there is no reliable or acceptable water on premises.7 Water fetching typically involves travelling to a water access point, queuing for some period of time, filling containers that quickly become heavy and lifting and carrying heavy containers home by foot, bicycle, pack animal or motor vehicle.8 In addition to causing significant opportunity costs, such as time that might otherwise be spent on education or income generation,9 each component of the water-fetching process increases exposure to hazards and risk of injury.
To date, the consequences of suboptimal water access have largely focused on water-related diseases, such as the widely used ‘Bradley Classification’ of waterborne, water-washed, water-based and vectorborne diseases.10–13 However, recent studies and reviews on water carriage have underscored the need to better understand the prevalence of water-fetching injuries and factors that could help explain such injuries.2 8 9 14 15 Such data would help to more accurately determine the public health costs and consequences of poor water access.16 For example, recent estimates suggest that 105 million (3.9%) disability-adjusted life years (DALYs) can be attributed to inadequate water, sanitation and hygiene (WaSH).10 However, these estimates do not account for water-fetching injuries because current data are not disaggregated by mechanism of injury, such that, for example, the proportion of musculoskeletal injuries attributable to WaSH cannot be calculated.10 17 18
Indeed, myriad other injuries have been documented in conjunction with water acquisition. For example, those who fetch water may experience assault or violence en route to or while queueing for water,4 attacks from dangerous animals at the water source,19 musculoskeletal injury when hauling up buckets of water8 20 and road accidents when returning home.16 These risks likely exacerbate social disparities, gender inequality and maternal and child health problems, as women and children typically bear the burden of water fetching.7 21
A more robust documentation and characterisation of water-fetching injuries would also help track progress towards achieving Sustainable Development Goal (SDG) 6, that is, the universal and equitable access to safe and affordable drinking water for all.22 WHO and UNICEF Joint Monitoring Programme’s (JMP)’s drinking water service ladder currently emphasises safety in terms of water quality, but safety of acquisition is a critical and underexplored dimension.6
Therefore, we sought to characterise water-fetching injuries in households from a diversity of sites in low-income and middle-income countries using what we believe to be the largest and most comprehensive global dataset on physical injuries relating to acquiring water. We first describe the frequency and characteristics of water-fetching injuries, including the type of injury, mechanism of injury, bodily location of the injury and physical context in which the injury occurred. Second, we sought to identify potential sociodemographic and water access-related correlates of water-fetching injuries based on the burgeoning literature on the subject. Specifically, we hypothesised that injuries would be positively associated with the following sociodemographic factors: being female, being older, having lower socioeconomic status and residing in rural areas.7 9 16 20 We also hypothesised that injuries would be positively associated with the following water access factors: greater household water insecurity, reliance on water sources located outside the home, longer time spent collecting water and being the person responsible for water collection in the home.9 21
Methods
Study setting and data collection
Data were drawn from the Household Water Insecurity Experiences (HWISE) study, the primary objective of which was the development and validation of a cross-culturally equivalent scale to measure household water insecurity.23 As described elsewhere, a range of cross-sectional data on sociodemographics and experiences with water access and use were collected in 2017–2018 from approximately 250 individuals in each of 29 sites across Central, South and Southeast Asia, sub-Saharan Africa, the Middle East and Latin America and the Caribbean (n=8633).24 Sites were selected to maximise heterogeneity of region, urbanicity, water infrastructure and problems with water. In most sites, households were selected using simple random sampling.23 24 Adults were considered eligible if they ‘were knowledgeable about their household’s water situation.’24
Enumerators sought verbal or written informed consent in the respective local language per local institutional review board agreements. (online supplemental table 1).
Supplemental material
Definitions and variable creation
Two survey questions probed water-related injury in 24 HWISE sites, which we defined as physical harm caused to a person in the process of water acquisition. The first was a yes/no item: ‘Have you ever been injured while fetching water?’ If the respondent affirmed having been injured, the interviewer asked ‘How?’ and recorded as many injuries as the respondent could recall. Injuries that were not directly experienced by the respondent were excluded to increase accuracy and to ensure a standardised denominator. Injury-related questions were not asked in five HWISE sites because principal investigators in those sites did not opt to include those questions in their survey.
To characterise water-fetching injuries, we first exported open-ended response(s) from those who reported injuries into a qualitative data analysis program (Atlas.ti 8). A qualitative coding framework was developed with codes from a prior systematic review on water fetching14 as a starting point. The final codes were harmonised with the International Statistical Classification of Diseases and Related Health Problem-11 codes25 to ensure the use of universal definitions with future applicability. Responses were coded into four injury-related categories: (A) type of injury or injury-related symptoms (pain and fatigue), (B) mechanism of injury, (C) bodily location of injury and (D) physical context in which the injury occurred (see online supplemental table 2 for details). When a respondent reported more than one type of injury, a new observation was created, such that the unit of analysis was the injury, not the individual.
Gender, age and socioeconomic standing were self-reported. Socioeconomic standing was assessed using the MacArthur Scale of Subjective Social Status; participants were asked to select which rung on a ladder they believed their household stood compared with their community (top rung scored as ‘10’ and bottom rung as ‘1’).26 Household urbanicity was determined by enumerators as rural, periurban or urban.
Household water insecurity was measured using the HWISE Scale, which queries 12 different experiences with water access and use over the prior 4 weeks.23 Responses are ‘never’ (scored as 0), ‘rarely’ (1), ‘sometimes’ (2) and ‘often’ or ‘always’ (3). An earlier version of the HWISE Scale that contained only 11 of the 12 final HWISE items was administered in the first 17 sites.24 Regression analyses of the scores for the 11 HWISE items asked across all sites against scores for those sites for which 12 items were available showed that the 11 items accounted for 99.3% of the variation (p<0.001). We, therefore, used the 11-item HWISE indicator (0-33) as a proxy for the validated 12-item HWISE Scale to leverage data across all 24 sites.
Data about water source types, number of trips to source per week and round-trip time to water source were collected per JMP guidelines.6 Although these three variables are often combined to generate the single ‘JMP drinking water service level’ variable, there is reason to think that distance to water source poses a distinct risk of injury from type of water source.2 Therefore, we first created a variable for hours spent collecting water per week by multiplying the number of trips to source per week by the round-trip time to a household’s primary drinking water source. We then reclassified primary drinking water sources into four types in increasing order of hypothesised risk of injury: (1) on premise (source on premise or neighbouring plot); (2) small vended quantity (eg, bottled water, sachet water or from small vendors); (3) off-premise with queueing (off-premise wells, off-premise standpipes or off-premise tanker trunks where the risk of injury or violence while queuing may be higher) and (4) surface waters (surface water, springs or small dams that may require carrying heavy loads across greater distances).
Potential answers to questions about who was responsible for water collection were ‘self,’ ‘spouse, child other family’, or ‘shared,’ where at least one other household member was involved with water collection including the respondent.
Statistical analysis
We summarised categorical variables as percentages, normally distributed continuous variables as means and skewed data as medians. For our first objective, we summarised injury frequency and characteristics by site. We also tested for differences by gender using Pearson’s χ² test.
Next, to identify correlates of water-fetching injury, we first estimated the odds ratio (OR) of injury for each covariate of interest. We then fitted a multilevel, mixed-effects logistic regression model of injury occurrence with random effects to control for study sites and within-site sampling clusters. We included theoretically plausible independent variables identified a priori, namely gender, age, socioeconomic standing, urbanicity, household water insecurity, water source by injury risk, time spent collecting water per week and responsibility for water collection. Stata V.15.1 was used for all statistical analysis.
Patient and public involvement
This research was done without patient involvement. It was not appropriate or possible to involve patients or the public in this work.
Results
Of the 7401 respondents in the 24 HWISE sites where the injury question had been asked, 6291 (85.0%) reported on personal experiences with water-fetching injuries, and thus comprised the analytic sample for our first objective.
Nearly three-fourths of respondents were female (72.3%), and the mean age was 37.6 years (SD 13.5) (table 1). Forty-three per cent of respondents lived in rural settings and 18.4% reported using on-premise drinking water sources. The mean water insecurity score was 7.2 (SD 7.7), indicating a relatively low level of water insecurity across the sample. Respondents reported spending a median of 1.5 hours (IQR 7.0) per week collecting water. Half of the respondents said they bore the primary responsibility of making sure there was enough water in the house.
Characteristics of 6291 individuals from 24 sites included in the analytic sample for water-fetching injury, by region
The prevalence of any reported injury was 13.4% (n=845). A total of 879 injuries were reported, as 30 individuals each reported two injuries, and two individuals each reported three injuries. Sites with the greatest proportion of respondents reporting injuries included Gressier, Haiti (38.4%); Kisumu, Kenya (31.9%); Chiquimula, Guatemala (29.1%); Punjab, Pakistan (29.1%) and Accra, Ghana (23.8%) (table 1). The mean age of respondents reporting water-fetching injuries was 37.7 years (SD 13.7).
Of the injuries for which “type” was specified (n=185), fractures or dislocations (29.2%), pain (22.2%) and lacerations (20.0%) were the most common (figure 1A). Most injury types were of an unspecified nature (65.4%) or missing (13.5%), even when other details were provided, for example, ‘Hit my foot and hurt my hand while carrying the water’ (Gressier, a 24-year-old woman).
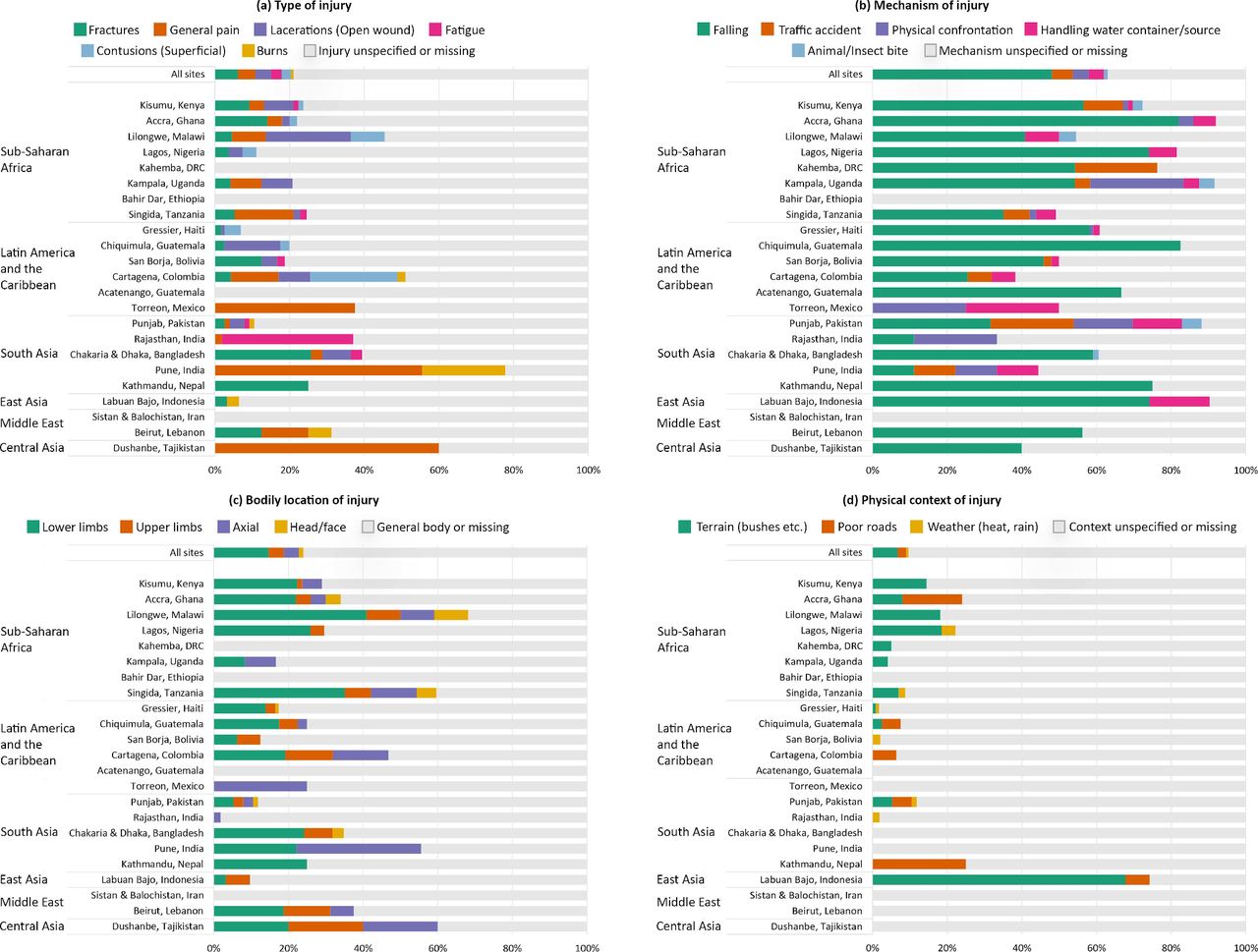
Characteristics of the 879 reported water-fetching injuries by (A) type of injury, (B) mechanism, (C) bodily location and (D) physical context across 24 HWISE sites in 21 low-income and middle-income countries. Note: sites are ordered within each geographical region by descending proportion of any reported injuries. Bars are stacked by descending proportion reported within each category across all sites. Colours represent different categories in each panel. Respondents in Honda, Colombia did not report any injuries and are not shown in this figure. HWISE, Household Water Insecurity Experiences.
Where the “mechanism” of injuries was specified (n=554), falls were the most common (76.4%) (figure 1B). People described slipping or tumbling while queuing or carrying water, as well as falling into wells or bodies of water. For example, in Malawi, a respondent ‘was running to be first in line and fell in the process’ (Lilongwe, a 22-year-old woman), and in Ghana, someone reported that they ‘broke (their) leg due to falling on hilly rocks (and) slipped’ (Accra, a 37-year-old woman). Traffic accidents, which included vehicular accidents, bicycle accidents or those incurred while riding an animal during water fetching, contributed to 8.7% of specified injury mechanisms, with nearly all in Punjab, Pakistan (n=17), Kahemba, Democratic Republic of Congo (DRC) (n=13) and Kisumu, Kenya (n=8) (figure 1B). Physical confrontation led to 6.9% of all specified injury mechanisms (figure 1B). Typical confrontations included quarrelling or fighting with neighbours or while waiting in the queue for water: ‘One time when the standpipe wasn’t working, I went to the well instead and people fought and beat me’ (Kampala, a 39-year-old woman). There were also intimations of sexual assault: ‘The caretaker of the pre-paid meter wanted to fall in love with me, but I told him that I am married and have children which led him to hate me and he has hit me before’ (Kampala, a 46-year-old woman). Injuries occurring from carrying water containers or collecting water from wells accounted for 6.5% of specified injury mechanisms and were reported in more than half of all sites.
“Bodily location” was specified for 211 reported injuries. Nearly two-thirds of these were injuries to the lower limbs (61.1%) (figure 1C).
Information on “physical context” was available for 85 (9.7%) injuries (figure 1D). Of the specified contexts, 69.4% occurred due to dangerous terrain (eg, falling into bushes, stepping on nails), 23.5% due to poor roads, and 7.1% due to weather, for example, heat or rain.
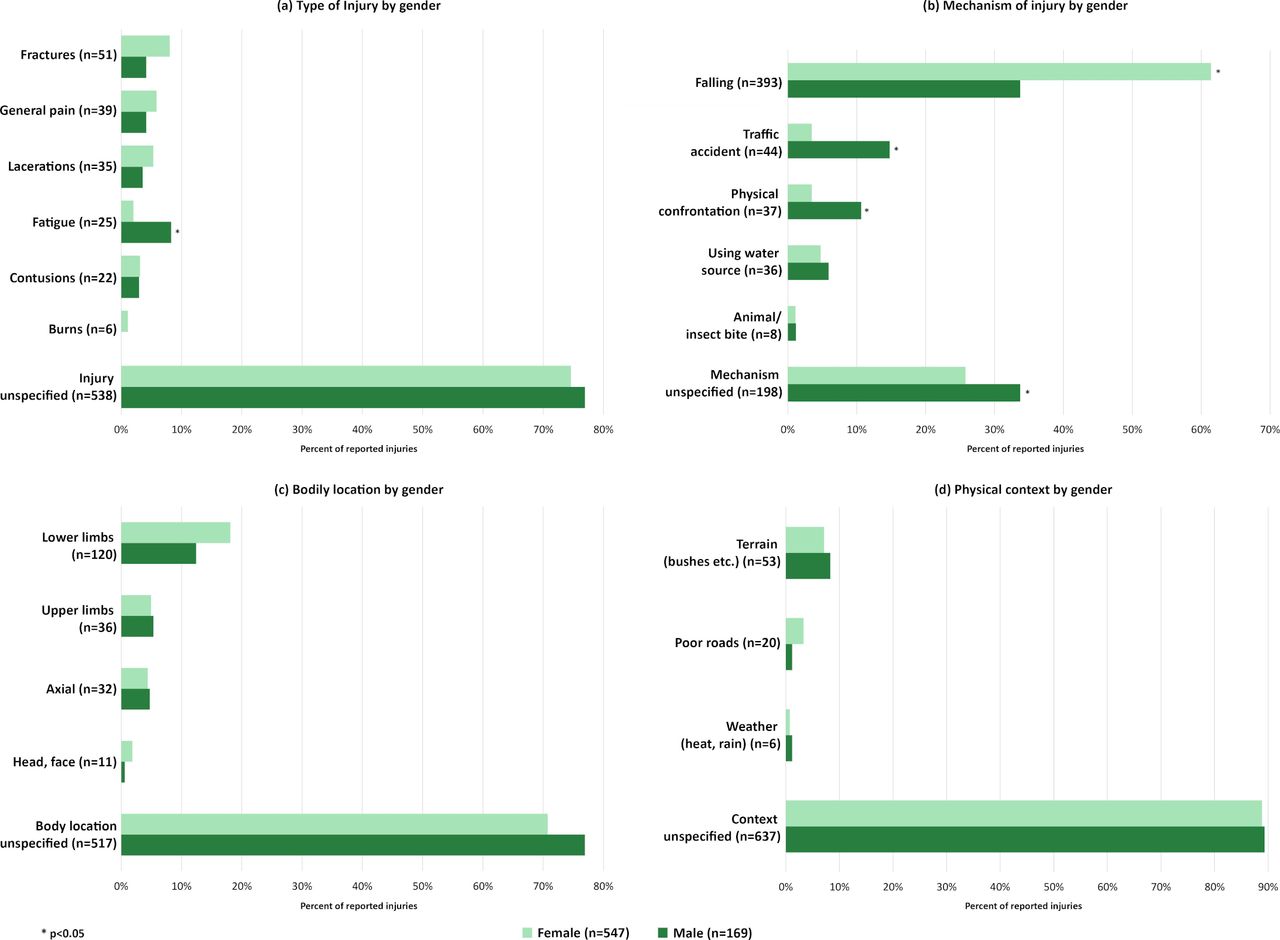
In bivariate analyses, there were several significant gender differences in characteristics of injuries. Men were significantly more likely than women to report fatigue (8.3% vs 2.0%) (figure 2A) and traffic accidents (14.8% vs 3.5%) (figure 2B). Women were nearly twice as likely to fall as men (61.4% vs 33.7%) (figure 2B). Men were also significantly more likely than women to report injuries from physical confrontation (10.7% vs 3.5%) (figure 2B).
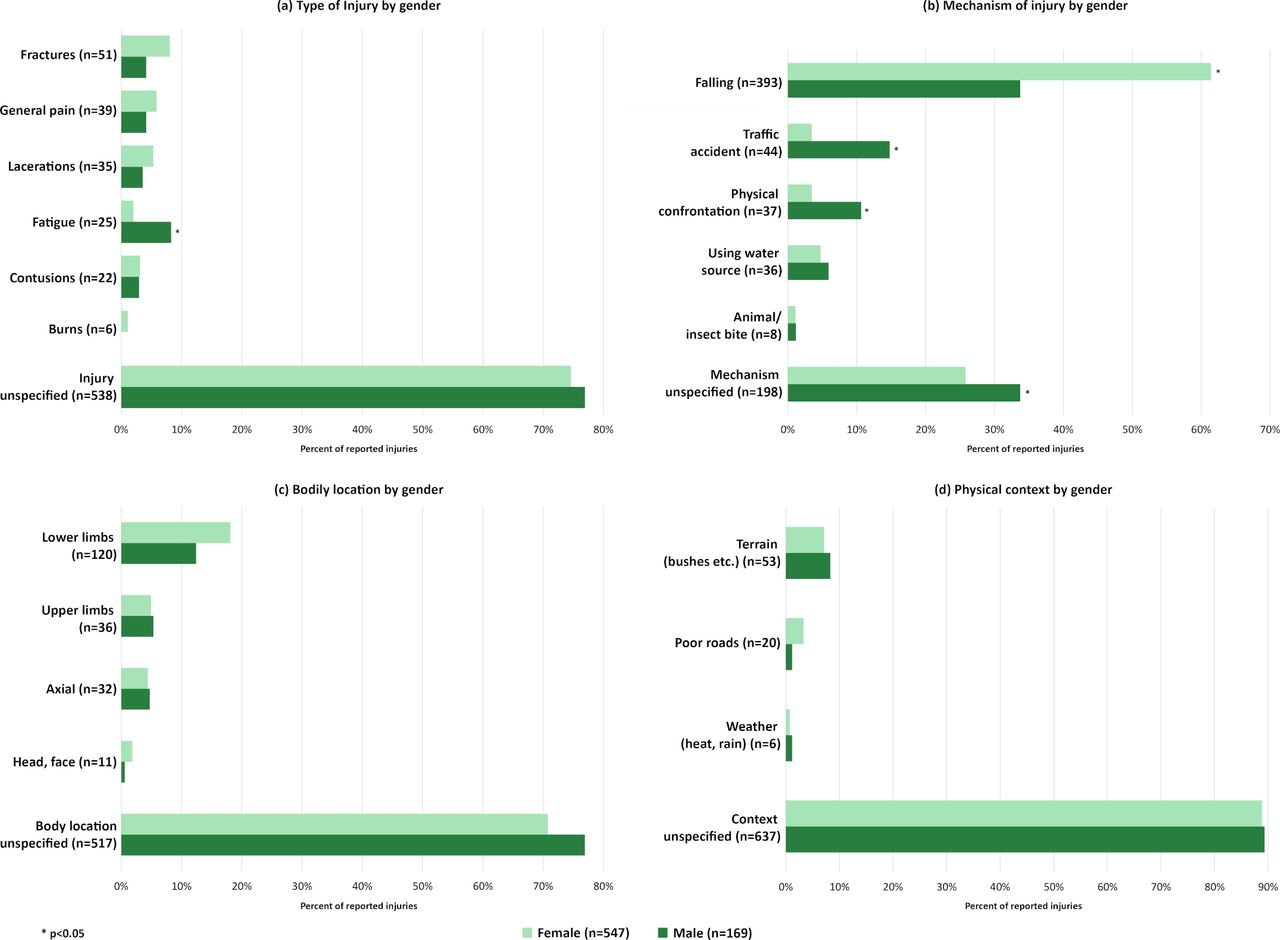
Gender differences in reported water-fetching injuries by (A) type of injury, (B) mechanism, (C) bodily location and (D) physical context across 24 HWISE sites in 21 low-income and middle-income countries (n=716). HWISE, Household Water Insecurity Experiences.
We began investigating our second objective, understanding the covariates of any injury, using single-predictor regression analyses [table 2 (1)]. Most characteristics of those who reported injuries were significantly different from those who did not. Notably, women were significantly more likely to report injuries than men (OR 1.35; 95% CI 1.05 to 1.74).
Odds of injury during water fetching in single-predictor and multivariable models among 4169 respondents
Our fully adjusted model [table 2 (2)] comprised 4169 observations with full information on all covariates. Individuals excluded because of incomplete data were similar in age to those included, but were significantly more likely to be female, live in rural or periurban areas, have a higher household water insecurity score, report water-fetching injuries, and use off-premise water sources (online supplemental table 3).
In the full model of predictors of any injury, women had 1.50 (95% CI 1.15 to 1.96) times greater odds of injury than men [table 2 (2)]. The odds of injury for rural dwellers and periurban dwellers were 4.80 (95% CI 2.83 to 8.15) and 2.75 (95% CI 1.64 to 4.60) times higher, respectively, than for urban dwellers.
Greater household water insecurity was significantly associated with greater odds of reporting a water-fetching injury (adjusted OR (aOR)=1.09, 95% CI 1.07 to 1.10). For example, a person with a household water insecurity score of 10 out of 33 would have a 90% greater odds of reporting injury than someone with a household water insecurity score of zero.
Off-premise water sources requiring queuing (aOR=1.72, 95% CI 1.19 to 2.49) and surface waters (aOR=1.97, 95% CI 1.21 to 3.22) were associated with greater odds of injury than on-premise sources. Each additional hour spent collecting water per week was associated with a two percent increase (95% CI 1.01 to 1.03) in the odds of water-fetching injury.
Reporting that someone else was responsible for ensuring sufficient household water (aOR=1.32, 95% CI 1.01 to 1.73), or that the responsibility was shared (aOR=1.39, 95% CI 1.07 to 1.81) were both associated with increased odds of injury.
Discussion
Using some of the most comprehensive global data on physical injuries relating to acquiring water, we described the frequency and characteristics of water-fetching injuries and identified several significant sociodemographic and water access-related correlates. We found that 13% of respondents across 24 sites in low-income and middle-income countries reported at least one injury. As hypothesised, significant correlates of injury included being female, residing in rural settings, household water insecurity, time spent collecting water and accessing off-premise water sources. These findings demonstrate that water-fetching injuries are an important and under-appreciated consequence of inadequate water access and contribute to the true burden of inadequate WaSH.
Notably, women were 1.5 times more likely to report injury than men, adjusting for other sociodemographic and water access-related covariates (table 2). Our finding supports existing literature that strongly emphasises the link between gender and suboptimal water access.4 7 This may be a result of social norms (women are more likely to be the primary water fetchers), unequal access to modes of transporting water and physiological differences. For example, the relatively slender spines of young women and girls are more vulnerable to injury from axial loading (eg, carrying water on one’s head).27 Therefore, water interventions that aim to address issues of gender equity have the added potential to reduce incidence of water-fetching injuries. Our analysis also indicates that prioritising such interventions in rural and peri-urban settings are likely to have an even more substantial impact on harm reduction.
We also found that each point increase in household water insecurity was associated with a nine per cent increase in the odds of water-fetching injury. These results demonstrate that injuries are yet another manifestation of water insecurity beyond singular measures of water scarcity or access to water infrastructure.28 The association between water-fetching injury and household water insecurity adds to the emerging literature on other correlates of household water insecurity, including food insecurity, depression, diarrhoea and less resilience to cholera.3 29–31
Time spent collecting water and using off-premise drinking water sources (‘off-premise with queueing’ and ‘surface waters’ categories) were also significantly associated with water-fetching injury. As hypothesised, ‘surface waters’ had the highest odds of injury, likely due to people walking longer distances to fetch water.6 Although those accessing off-premise sources such as wells, standpipes and tanker trucks may walk shorter distances and spend less time collecting water than those accessing surface waters, we had hypothesised that they would be more likely to face a higher risk of injuries through conflict while queueing for water.2 Indeed, nearly all the physical confrontation reports occurred among those primarily using off-premise wells, standpipes and tanker trucks. By categorising water sources based on potential injury risk rather than potential water quality, and by disaggregating source type and time spent collecting water, our findings suggest that the globally used aggregate indicator of ‘safely managed water’ monitored by the JMP does not entirely capture the risks that people face during water acquisition for various household needs.
One unexpected result was that having the sole responsibility for water collection was not associated with higher risk of water-fetching injury, as we had hypothesised. It is possible that the sharing of responsibility reflects a coping strategy, where previously injured individuals—or those with any physical limitation that increases the risk of injury—delegate water fetching to another household member or require help to fetch water.9 It may also indicate that such households are so water insecure that multiple people are required to fetch enough water for household needs. Furthermore, responsibility may be shared unequally, such that for some, water-fetching may be an infrequent activity, whereas for others, it may approach their maximum loading injury tolerance. This may occur in settings with unreliable water supplies where women try to collect as much water as possible in limited time, perhaps with assistance from children, but still endure most of the burden.7 21 It will be interesting to see if this finding is replicated elsewhere, and if so, what the reason(s) are for this relationship.
Taken together, our findings are relevant to policy and programming in that they help identify various additional barriers to accessing safely managed drinking water (ie, SDG 6) beyond water quality and quantity. For example, is it simply the distance to a household’s primary water source that is a barrier, or is it the physical context or terrain, the fear of violence when water fetching, and/or the physical and financial cost of hauling water to the home?32 Our findings suggest several such opportunities for implementers to help mitigate the effects of water-fetching injuries through existing programming. For example, providing and maintaining numerous shared water points throughout rural and peri-urban communities and supporting affordable local water delivery systems can reduce overall water-fetching trip distance and time spent in queues. Providing access to affordable equipment, such as wheelbarrows, can further help mitigate pain and fatigue.14 33 Maintaining clear pathways along water collection routes can enable easy use of wheelbarrows or other equipment, and reduce the risk of injury due to slips, falls and traffic hazards.9 15 Encouraging men to help with water carriage, e.g. through public health campaigns, can reduce women’s injury risk and other adverse maternal and child health outcomes associated with water fetching.2 Lastly, locating water points in visible, open, public places can reduce the risk of gender-based violence or abuse.4
In this manner, we demonstrate that documenting and understanding the nature of water-fetching injuries and associated barriers would provide valuable data on physical safety and accessibility not covered by available international WaSH indicators. Not only can such indicators guide the design of interventions to reduce injury risk, but also the development of equitable solutions for water access. As such, our findings support Bartram and Hunter’s recommendation to revise Bradley’s classification of water-related hazards to incorporate the class of ‘water access-related disease’ with subclasses inclusive of ‘injury and violence associated with water collection.’11 Being able to attribute global injury data to water fetching would allow this new class of water access-related disease to be included in the DALY measurements for WaSH burden of disease estimates.
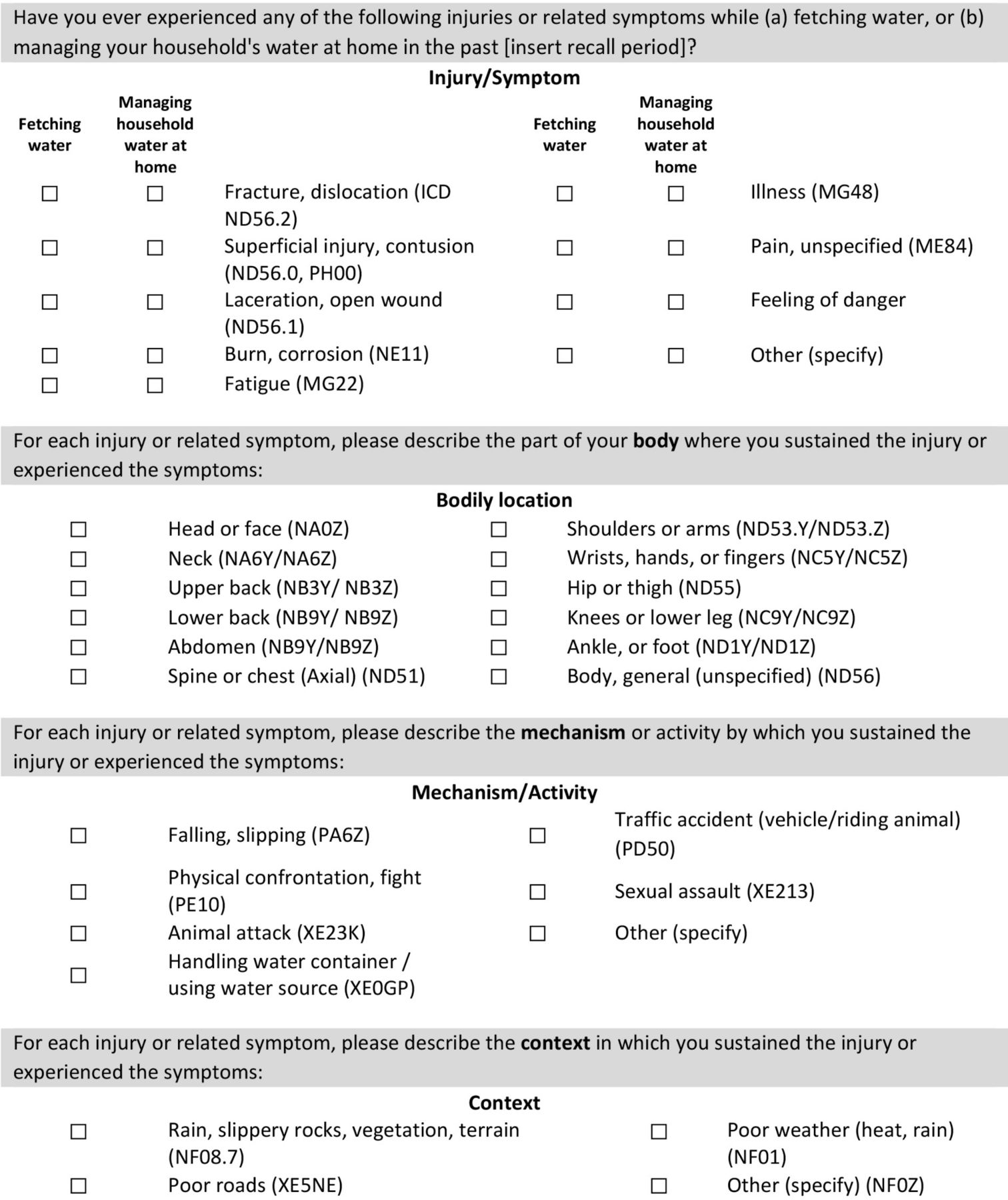
To this end, we propose the collection of data that more comprehensively capture the diversity of potential water-fetching injuries (figure 3). This suggested module would benefit from validation by experts, for example, using a Delphi method, as well as field testing. Once validity is established, these data can determine cause-and-effect relationships, long-term consequences of injury and risk management strategies. Future research and WaSH monitoring and evaluation should therefore measure the (1) prevalence of water-fetching injuries within a given timeframe (eg, in the past year), (2) injury type, mechanism, bodily location and physical context, and (3) severity and impact of the injury and related symptoms or disability. For example, the inclusion of a symptom severity scale, such as the New Injury Severity Score,34 would help reveal the intensity of the pain and fatigue documented across several sites. If resources exist, optimal data collection procedures should include a simple physical examination, adequate questioning to capture a subjective history, general health, detail of injury mechanisms and noting clusters of symptoms in different parts of the body.14
{kind=link}
{kind=link}
{kind=link}
Suggested survey module for assessing water-fetching injuries and related symptoms. Note: Illustrative ICD-11 codes are listed next to each option when possible. Each injury can have multiple ICD-11 codes for mechanism, body location and context. See online supplemental table 4 for an editable version of this suggested survey module. ICD, International Statistical Classification of Diseases.
Future research should also explore the links between water-fetching injuries and other health consequences, particularly psychosocial stress. While the association between stress and water insecurity has been increasingly well documented,35 we suggest that other contributors to this stress may include persistent pain, fear of re-injury or fear of further conflict or violence.4 36 Stress and fear of injury can also contribute to fatigue, a common symptom attributed to water fetching in these data and elsewhere.15 Both stress and fatigue are associated with pain intensity,37 a key symptom of physical injury.
Despite the notable strengths, our analyses were limited by the cross-sectional study design. It is possible that socioeconomic standing was not a significant predictor in multivariable models because we based it on subjective self-report.26 Similarly, enumerators determined rural/urban/periurban classifications subjectively rather than based on objective criteria, such that the classification may have been idiosyncratic. Because these injury data were self-reported, it was impossible to assess mortality; this could be assessed in future studies through a review of medical records or other reports that may reveal data such as deaths from drowning while fetching water. Further, because a majority of responses to the open-ended question about the nature of injury were unspecified, and we did not ask survey respondents about frequency of injuries, our understanding of the characteristics of injuries is limited. It is also possible that a better-prescribed recall period could lead to greater specificity in the description of the injury. With such high numbers of unspecified answers, we also could not build multivariable models for each characteristic (ie, type, mechanism, bodily location, physical context) of injury. This shortcoming can be remedied by using a survey module per the above (figure 3). As such, our results are likely an underestimate of water-fetching injuries, which highlights the importance of systematically documenting injury prevalence in future global water insecurity and WaSH research.
In sum, these data point to the burden of injury attributable to water acquisition. There is a clear need for safe water interventions that prioritise personal safety alongside the traditional goals of improved water quality and proximity to the home. Future research and programming should collect data on water-fetching injuries to more accurately represent the true burden of inadequate WaSH on health and well-being.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Sanni Yaya
Twitter @vvram15, @GeereJo, @profserayoung
Collaborators Household Water Insecurity Experiences Research Coordination Network (HWISE RCN): Ellis Adams (University of Notre Dame, Notre Dame, IN, USA); Jam Farooq Ahmed (University of Washington, Seattle, WA, USA); Mallika Alexander (Johns Hopkins University-Byramjee Jeejeebhoy Medical College Clinical Trials Unit, Pune, India); Mobolanle Balogun (College of Medicine of the University of Lagos, Lagos, Nigeria); Michael J. Boivin (Michigan State University, East Lansing, MI, USA); Alexandra Brewis (Arizona State University, Tempe, AZ, USA); Genny Carrillo (Texas A&M University, College Station, TX, USA); Kelly Chapman (University of Florida, Gainesville, FL, USA); Stroma Cole (University of the West of England, Bristol, UK); Shalean M. Collins (Tulane University School of Public Health and Tropical Medicine, New Orleans, LA, USA); Jorge Escobar-Vargas (Pontificia Universidad Javeriana, Bogotá, Colombia); Hassan Eini-Zinab (Shahid Beheshti University of Medical Sciences, Tehran, Iran); Matthew C. Freeman (Emory University, Atlanta, GA, USA); Hala Ghattas (American University of Beirut, Beirut, Lebanon); Monet Ghorbani (Arizona State University, Tempe, AZ, USA); Ashley Hagaman (Yale University, New Haven, CT, USA); Zeina Jamaluddine (American University of Beirut, Beirut, Lebanon); Wendy E. Jepson (Texas A&M University, College Station, TX, USA); Divya Krishnakumar (Anode Governance Lab, Bengaluru, India); Kenneth Maes (Oregon State University, Corvallis, OR, USA); Jyoti Mathad (Weill Cornell Medicine, Center for Global Health, New York, NY, USA); Jonathan Maupin (Arizona State University, Tempe, AZ, USA); Hugo Melgar-Quiñonez (McGill University, Ste-Anne-de-Bellevue, Quebec, Canada); Joshua D. Miller (Northwestern University, Evanston, IL, USA); Milton Marin Morales (Universidad Autónoma del Beni José Ballivián, Bolivia); Javier Moran (Autonomous University of Coahuila, Coahuila, Mexico); Nasrin Omidvar (Shahid Beheshti University of Medical Sciences, Tehran, Iran); Patrick M. Owuor (Northwestern University, Evanston, IL, USA); Sabrina Rasheed (International Centre for Diarrhoeal Disease Research Bangladesh, Mohakhali, Dhaka 1212, Bangladesh); Asher Y. Rosinger (Pennsylvania State University, State College, PA, USA); Luisa Samayoa-Figueroa (McGill University, Ste-Anne-de-Bellevue, Quebec, Canada); Marianne V. Santoso (Northwestern University, Evanston, IL, USA); Roseanne C. Schuster (Arizona State University, Tempe, AZ, USA); Mahdieh Sheikhi (Shahid Beheshti University of Medical Sciences, Tehran, Iran); Sonali Srivastava (Anode Governance Lab, Bengaluru, India); Chad Staddon (University of the West of England, Bristol, UK); Andrea Sullivan (University of Miami, Coral Gables, FL, USA); Yihenew Tesfaye (Bahir Dar University, Bahir Dar, Ethiopia); Nathaly Triviño (Pontificia Universidad Javeriana, Bogotá, Colombia); Alex Trowell (University of Amsterdam, Amsterdam, The Netherlands); Desire Tshala-Katumbay (Oregon Health & Science University, Portland, OR, USA); Raymond Tutu (Delaware State University, Dover, DE, USA); Amber Wutich (Arizona State University, Tempe, AZ, USA).
Contributors JS, SLY and HWISE RCN collaborators collected data across the 24 sites. SLY, JS, and VV initiated the analysis. VV and BT conducted the qualitative analysis, with guidance from J-ALG. PRH, J-ALG and VV conducted the statistical analyses, with input from JS and SLY. VV wrote the first draft of the paper, with input from J-ALG, BT, JS and SLY. All authors contributed to discussions and interpretation of the data, to revisions of the manuscript, and approved the final draft of the manuscript.
Funding This project was funded by the Competitive Research Grants to Develop Innovative Methods and Metrics for Agriculture and Nutrition Actions (IMMANA). IMMANA is funded with UK Aid from the UK Government. The Household Water Insecurity Experiences Research Coordination Network (HWISE RCN) is supported by the National Science Foundation (NSF) BCS-1759972. The project was also supported by the Buffett Institute for Global Studies, the Center for Water Research, and the Resnick Family Social Impact Fund, Institute for Sustainability and Energy at Northwestern University; and the Office of the Vice Provost for Research of the University of Miami.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Study activities were reviewed and approved by all relevant ethical review boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on request.