Article Text

Abstract
The geographic and economic characteristics unique to island nations create a different set of conditions for, and responses to, the spread of a pandemic compared with those of mainland countries. Here, we aimed to describe the initial period of the COVID-19 pandemic, along with the potential conditions and responses affecting variation in the burden of infections and severe disease burden, across the six island nations of the WHO’s Africa region: Cabo Verde, Comoros, Madagascar, Mauritius, São Tomé e Príncipe and Seychelles. We analysed the publicly available COVID-19 data on confirmed cases and deaths from the beginning of the pandemic through 29 November 2020. To understand variation in the course of the pandemic in these nations, we explored differences in their economic statuses, healthcare expenditures and facilities, age and sex distributions, leading health risk factors, densities of the overall and urban populations and the main industries in these countries. We also reviewed the non-pharmaceutical response measures implemented nationally. We found that the burden of SARS-CoV-2 infection was reduced by strict early limitations on movement and biased towards nations where detection capacity was higher, while the burden of severe COVID-19 was skewed towards countries that invested less in healthcare and those that had older populations and greater prevalence of key underlying health risk factors. These findings highlight the need for Africa’s island nations to invest more in healthcare and in local testing capacity to reduce the need for reliance on border closures that have dire consequences for their economies.
- COVID-19
- epidemiology
- health systems
- public health
- prevention strategies
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Six WHO African region Member States are considered island nations. While the geographic context and small, dispersed local populations mean pandemic control could be easier in the islands than in countries with porous land borders and densely populated urban centres, they face substantial challenges in dealing with global health emergencies due to their limited healthcare facilities and strong dependence on tourism.
SARS-CoV-2 infection burden was highest in countries that had larger economies or greater capacity for case detection. However, the burden of severe COVID-19 outcomes was highest in countries with older populations, lower healthcare capacity, and where the prevalence of pre-existing health risk factors including cancer, diabetes, air pollution and obesity was high.
Early interventions and movement restrictions at the beginning of the COVID-19 pandemic were important for delaying and limiting community spread, but over-reliance on these measures in African island countries dependent on international travel can have dire consequences for their economies.
Action and investments are needed to improve testing capacity, reduce the prevalence of health risk factors, strengthen the healthcare system as well as to decrease the dependencies of the economies of the African island nations on international travel.
Introduction
In 2020, the global health situation changed due to the spread of a new virus, SARS-CoV-2, which was first detected at the end of 2019 in Wuhan, China.1 The WHO, on 11 March 2020, declared the outbreak of COVID-19, caused by the SARS-CoV-2 virus, a global pandemic.2 This situation led to a patchwork of strategies to contain COVID-19 at the local and global level. Most national governments across the world implemented a combination of measures that included travel and movement restrictions, lockdowns, curfews, limited social interactions and physical distancing. These interventions were aimed at containing the outbreak, to avoid overburdening the healthcare system, and otherwise mitigate the pandemic’s negative impacts at the local and national levels.3–5 While they shared the goals of limiting viral transmission, protecting the most vulnerable individuals from exposure, and detecting, isolating and treating infected individuals, the methodologies and stringency employed were highly variable across countries. In most instances, the strategies adopted were based on the local context, available resources, critical challenges and the epidemiological characteristics of COVID-19 at the time of the decision-making.6 The lack of coordinated response strategies within and between countries during this crisis has been a motivator for the global health community to put in place more plans and protocols for preparedness, but it has also provided an opportunity for leaders to evaluate what strategies have been most effective.
According to the WHO, the vast majority of the locations that have kept their territories free from COVID-19 as of September 2021 have been small island nations. More specifically, Cook Islands, Nauru, Niue, Tokelau, Saint Helena, the Federated States of Micronesia, Tonga, Tuvalu, the Pitcairn Islands and Kiribati have all avoided documenting any cases. Other island nations have reported single-digit case counts, such as Samoa, Vanuatu, the Marshall islands and Palau.7 Most of these countries strictly restricted the influx of travellers early on in the pandemic.8 Stringent controls to limit movement, and specifically the early timing of those controls, were shown to have had an important impact on containing the spread of COVID-19 in small island developing states (SIDSs) across much of the Caribbean.9 This finding is similar to the influenza pandemic of 1918, when the Pacific islands that imposed strict border controls delayed the introduction of the pathogen by 3–30 months and reduced mortality in comparison with the other islands that did not adopt similar measures.10 Similarly, larger coastal-island countries like New Zealand, Greece, Iceland and Singapore, which also implemented early strict measures, showed better containment of COVID-19 and fewer cases in comparison to inland countries.11–13 Very early controls to limit movement into countries may be particularly effective for SIDSs, particularly those in which population density and international connectivity are heavily impacted by the influx of tourists.
However, imposing indefinite border closure to avoid the introduction of the virus is not a sustainable measure due to harmful economic and social consequences, particularly for island nations.14 Most SIDSs are characterised by small and fragmented populations, remoteness, dependence on international trade and imported food, reliance on income generated from tourism and fishing industries, limited resources due to their small economies, vulnerability to external global financial shocks and high rates of food-related non-communicable diseases (NCDs).9 15–19 Moreover, they also face limitations regarding access to healthcare services.9 This, along with the resource constraints they face, restricts their capability to respond to global health emergencies.20 Furthermore, the global health security index, which measures the capacities of the countries to detect, prevent and handle health emergencies, is below 35 across the studied countries, when the global average is 40.2, and average score of high income countries is 51.9.21 As a result, reduced connectivity can result in the delay of imported goods and jeopardise medical evacuations.22 The performance of different island countries in response to COVID-19 likely depended on the complex interplay between these factors.
In this article, we examine the spread of, and response to, COVID-19 in the African island nations of Cabo Verde, Comoros, Madagascar, Mauritius, São Tomé e Príncipe and Seychelles from the start of the pandemic through 29 November 2020, all of which with the exception of Madagascar were on the United Nations list of SIDSs at the start of the pandemic. COVID-19 was first reported in Madagascar, Mauritius and Cabo Verde at the end of March 2020, and by the end of April 2020, all six countries had reported at least one confirmed case.7 By 29 November 2020, all six countries had experienced some levels of sustained local transmission. We focus on the first 9 months of the pandemic, prior to the deployment of vaccines, global dissemination of significant new variants and end-of-year festive seasons to understand what these nations experienced in terms of initial introduction and propagation of local spread. We then analyse differences in their geography, socioeconomic conditions and preparedness levels that may have influenced variation in their exposure to the virus and in their capacity to respond. We also examined the speed and comprehensiveness of control measures implemented in these countries, which likely had significant impacts on both introductions and further local spread of the virus.5 Box 1 includes a summary of our methodological approach and the data we analysed. To our knowledge, this is the first published study focusing exclusively on the COVID-19 outbreaks in these African island nations.
Summary of methodology and data sources.
The approach
For this study, we took a descriptive approach to present the trajectory of the pandemic during the first wave in the African island nations, between the first detected case in each country and 29 November 2021 (inclusive). Qualitative comparisons were made between these countries to understand how their prepandemic characteristics and peri-pandemic responses influenced the trajectory of their local COVID-19 epidemics. The complete list of data sources is given in online supplemental table S1. Data were processed and analysed using the R software, V.4.0.2 (https://www.r-project.org/).
The data
Local epidemic trajectories of the COVID-19 pandemic in African island nations were described using the reported infection burden (number and per-capita number of cases) and severe disease burden (number and per-capita number of deaths) in each country, expressed both cumulatively and daily over time. Population size estimates were obtained from the World Bank (online supplemental table S1).46 We included cases confirmed with PCR tests or rapid diagnosis tests (RDTs, which are less sensitive than PCR tests). At the time, confirmation required a positive PCR test result for SARS-CoV-2. However, cases marked as ‘probable’ due to sole availability of RDTs—representing only 70 cases from Comoros—were also included in the present analyses. Clinical outcome of each case (alive, dead, recovered) was used to calculate crude case fatality ratios (not adjusted for death or reporting lag). We excluded cases with missing clinical outcome status. The total reported number of tests performed (PCR and RDT), cumulatively and over time, were also compiled. All SARS-CoV-2 cases, deaths and tests reported were taken from official situation reports published by each country’s health ministry.
Data on the socioeconomics, healthcare and population structures of the countries investigated were obtained from the latest available scientific reports published by various international institutions and non-governmental organisations. This included sex and age distribution, population density and urbanisation, number of doctors/nurses/midwives per 1 k inhabitants, available healthcare facilities, density of health posts/health centres per 1 k inhabitants, number of hospitals, number of hospital beds per 1 k inhabitants, health expenditure, prevalence of obesity among adults, estimate of insufficient physical activity among adults, ambient air pollution attributable to disability-adjusted life years, probability of dying between the age of 30–70 due to diabetes, cardiovascular disease, cancer or chronic respiratory disease.47 ,34 39
Information about the measures adopted by each country in response to the COVID-19 pandemic were based on the COVID-19 Government Measures Data set published by ACAPS44 and the Oxford Coronavirus Government Response Tracker.45 From the latter resource, we adopted the stringency index, a composite measure of the strictness of government policies based on the nine response indicators, namely school closures, workplace closures, cancellation of public events, restrictions on public gatherings, closures of public transport, stay at home requirements, public information campaigns, restrictions on internal movements, international travel controls, which can take values between 0 (no measures) and 100 (most strict).
Supplemental material
COVID-19 pandemic in the African islands
An overview of the course of the pandemic in the African island nations (online supplemental figure S1) shows that each country experienced different epidemic magnitudes and trajectories, but that there was generally an initial wave of cases and deaths, followed by a lull lasting until the festive season following our study period.7 In March and April 2020, the first cases were detected throughout these islands in travellers arriving from both outside of the region (most notably from Europe) as well as from other countries within the Africa region. While many of the imported cases identified were among tourists, local transmission was first detected among contacts of locals who had recently returned home from abroad in Cabo Verde, Comoros, Mauritius and Madagascar. In Seychelles, cases originating from both foreign nationals and local residents returning from abroad were identified, but strict travel restrictions, quarantine, isolation and contact tracing measures kept the island free of true community spread until measures were eased in June, July and August. Similarly, the easing of containment measures in Madagascar in mid June 2020 was followed by a large wave of local transmission in July and August. In São Tomé e Príncipe, there were several clusters of cases following importation early in the pandemic, potentially due to limited local testing capacity and subsequent delays in case identification, but incidence had stabilised by August. The cumulative number of cases (figure 1) grew little after August 2020 onwards, with the exception of Cabo Verde, where the daily incidence of confirmed cases grew continuously from the start of its epidemic through the end of the study period (29 November 2020) and beyond (online supplemental figure S2). Similarly, the daily death counts in Cabo Verde kept increasing until the end of the study period, unlike in other countries (online supplemental figure S3).

The numbers of total cases and deaths, the case fatality ratio (CFR), and the cumulative attack rates (cases per million) for each island country as of 29 November 2020 are shown. We have shown CFRs in percentages. STP, São Tomé e Príncipe.

{kind=link}
{kind=link}
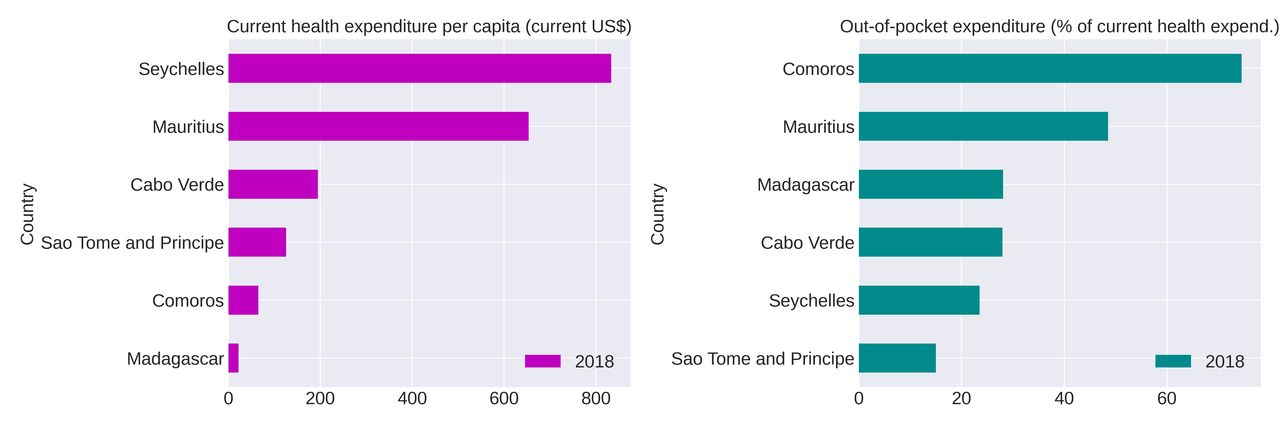
Health expenditure per capita (current US$) and out-of-pocket expenditure (% of current health expenditure) for each island nation corresponding to the year 2018.
In figure 1, online supplemental figure S2, S3 and table S2, we show the burden of infection with SARS-CoV-2 using the cumulative numbers of confirmed cases and cumulative attack rates (cases per million), the burden of severe COVID-19 using deaths and cumulative death rates (deaths per million), and the case fatality ratio (deaths/cases) in the African island nations of Cabo Verde, Comoros, Madagascar, Mauritius, São Tomé e Príncipe and Seychelles through 29 November 2020. Island territories of non-African countries in the African geographic region were not included. Although Guinea-Bissau is also a UN-designated SIDS in the WHO African region, since part of its territory shares land borders on the continent, it was also excluded from our analysis. The total number of cases ranged from 172 in Seychelles to 17 341 in Madagascar. Similarly, the number of deaths ranged from 0 in Seychelles to 251 in Madagascar, with four of the six islands managing to keep the number of reported deaths below 20. However, after accounting for population size, Mauritius had the lowest attack rate (396 cases per million inhabitants) and lowest death rate (7.9 deaths per million inhabitants) after Seychelles, which reported zero deaths during the study period. The two islands present in the Atlantic Ocean, Cabo Verde and São Tomé e Príncipe, reported the highest cumulative attack rates (19 141 and 4599 cases per million, respectively). In fact, Cabo Verde had the highest attack rate and second-highest death rate among all the sub-Saharan African countries during the study period (online supplemental table S2). Crude case fatality ratios (CFRs; unadjusted reported deaths divided by reported cases in the same time period) ranged from 0% in Seychelles to 2% in Mauritius and were lower or equal to the global average of 2%–3%13 during this time period. Although the total number of confirmed cases and deaths appeared low, the cumulative attack and death rates were high in most African islands compared with their non-island counterparts, owing to the low absolute population sizes of the islands, which makes individual cases easier to identify than in countries with larger populations and more dense urban centres (online supplemental table S2).
Examining potential factors contributing to variation in burden of COVID-19 infection and severe disease
Here, we lay out some of the key factors that likely contributed to variation in the burden of COVID-19 infection and severe disease at the start of this pandemic in African island nations. In order for cases to be identified and reported, there must first be exposure to imported cases, particularly for the initial spread of a pandemic disease. There must then also be clinical or epidemiological indication for conducting a test. Once a test is confirmed, there must be access to healthcare facilities, and these facilities must be prepared to provide the necessary diagnostics, care and data management capacity to transmit that information to national authorities. We, therefore, singled-out factors that affect disease exposure, presentation, and healthcare capacity.
Economy
According to the World Bank classification, Mauritius and Seychelles are high-income countries, Comoros, São Tomé e Príncipe and Cabo Verde are lower middle-income countries, and Madagascar is a low-income country.23 Tourism is a primary industry for most islands, whereas Comoros and São Tomé e Príncipe rely mainly on agriculture and fishing.24 Fishing is also a leading industry in Madagascar and Seychelles.25 Large tourism and fishing industries leading to a higher influx of international travellers and migrant workers, as is the case in these countries, has been documented as an important factor responsible for the spread of the virus at the beginning of the epidemic.26–28
Population structure
Factors such as population density and urbanisation have influenced the arrival of the first case and the within-country speed of the epidemic, respectively, in the context of the whole African continent.28 While the dependence of the arrival of the first case may not be on population density in the context of islands, the early spread of COVID-19 could still be influenced by urbanisation and might also explain the high attack rates in Cabo Verde, São Tomé e Príncipe and Seychelles (see table 1 and figure 1).
Indicators of population structure, healthcare capacity and health risk factors associated with an increase in the risk of severe disease and death from COVID-19
Age and sex distribution
There exist differences in the age distribution among islands (table 1), which may have impacted the number of deaths. It is known that the risk of severe disease and death due to COVID-19 is higher among older people.29 Given that Mauritius and Seychelles have a much higher percentage of people over 55 years of age (23.4% and 19.7%, respectively) in comparison to the other four island countries, we would expect higher mortality. Another interesting point about the age distribution is that Comoros, Madagascar and São Tomé e Príncipe have approximately 40% of the population under 14 years of age. With this age distribution, it would be expected that these countries had lower mortality since children are less affected by severe COVID-19.30 31 In addition to age risk, it appears that men are more susceptible to severe disease and death from COVID-19 than women globally.32 However, since all islands have a sex ratio approximately equal to 1, there is little variation in this factor to explore. That said, further exploration of the heavy skew towards male-dominated employment in the fishing industry (excluding postharvest)33 should be undertaken to understand whether the relatively heavy surveillance measures placed on this industry (particularly at points of entry) were able to help control spread and limit deaths in men compared with mainland countries.
Health risk factors
In addition to the age and sex distributions discussed above, we looked at a range of pre-existing health risk factors, such as diabetes and obesity, in the African island countries (table 1).34 According to WHO, pre-existing chronic health conditions, such as diabetes, obesity, cancer, air pollution, may increase the risk for severe COVID-19 disease.35 Obesity and nutritional insufficiency are prevalent in SIDSs, mainly due to low quality of available food choices and the dependence on food imports, characterised by food high in calories, fat and sweeteners.36–38 These factors contribute to high incidence of NCDs, which in some regions like SIDSs in the Pacific account for around 70% of total deaths. Obesity prevalence was lowest in Madagascar and highest in Seychelles. The prevalence of insufficient levels of physical activity was highest in Mauritius, with other countries reporting roughly 50%–60% less insufficiency. In five out of the six African island nations studied, the risk of premature mortality due to diabetes, cardiovascular disease, cancer or chronic respiratory disease for 30–70-year olds exceeded 20%, with Madagascar reporting 25%, and Cabo Verde reporting 17.4% probability of death due to these four categories of NCDs in this age group; the 2019 global average was 17.9% and average for all WHO Africa region countries was 20.8% (summary statistics obtained from the source dashboard listed in online supplemental table S1). The disability-adjusted life years due to air pollution34 was highest in Comoros and in Seychelles—at two ends of the wealth spectrum. The impact of air pollution on life expectancy was lowest in Cabo Verde, which also had indicators of greater access to healthcare (see below), suggesting investment in infrastructure that limits negative impacts on population health.
Healthcare capacity
The level of government expenditure as well as the encumbrance of out-of-pocket expenditures on households differ substantially between the countries (based on 2018 estimates; table 1). At first glance, all countries invest similar percentages of their annual gross domestic product (GDP) in healthcare services, with São Tomé e Príncipe spending the highest (6.3% of the total GDP), and Comoros spending the lowest (4.6%). However, due to large differences in their total GDP, the expenditure per capita differs substantially, with Seychelles spending around US$833 per capita per year, while Madagascar spends the lowest, US$22 per capita per year (see figure 2). As a result, the out of pocket expenditure that households need to cover can be as low as 15% for São Tomé e Príncipe and as high as 74.5% for Comoros.39 Finally, greater numbers of doctors, nurses and beds per 1000 inhabitants in Mauritius and Seychelles are indicative of their higher healthcare capacity compared with countries such as Madagascar and Comoros where resources are much more limited (table 1).
Testing
The availability of laboratory resources and equipment is a vital requirement for the early confirmation of positive cases and the epidemiological monitoring of the evolution of the outbreak at a national level. To this end, São Tomé e Príncipe and Cabo Verde faced challenges at the beginning of the pandemic, since they had to send samples for analysis to other countries, until their laboratories were ready to process suspected COVID-19 samples. This might have caused considerable delays in confirming positive cases40 41 and resulted in early epidemic spread before the implementation of restriction measures, thus leading to the very high cumulative attack rates (and corresponding death rates) in these islands (online supplemental table S2). In fact, it appears that the increase in cases in Cabo Verde occurred when the government initiated a free testing policy, meaning that undetected community spread was already occurring.40 It is also possible that before that testing policy, the small number of available tests caused under-reporting of cases, which led to a premature lifting of some restrictive measures while the number of cases was still increasing in the country. Table 2 shows information about the cumulative number of tests performed in each country and the cumulative test positivity rate over the study period. Mauritius, due to their mass testing policy that included systematic quarantine and symptom screening of all passengers and crew of leisure vessels, cargo ships and fishing boats42 and precautionary testing of all front-line healthcare workers,26 reported the highest number of total tests performed overall. Seychelles reported the lowest number of tests, despite mandatory testing requirements for incoming travellers at points of entry and for those moving between islands put in place very early in the pandemic. Cabo Verde performed the highest number of tests per 10 000 inhabitants and Madagascar the lowest. The cumulative test positivity rate was highest in Madagascar with 18.5% and lowest in Mauritius with 0.4%, as of 24 November 2020. Thus, countries did not have equal access to PCR tests, and it should be noted that the criteria to test also varied by country and over time within each country. Since the inclusion criterion in the WHO confirmed cases database was a positive PCR test for most countries, a bias towards underdetection of cases likely prevailed in the more resource-limited settings such as Madagascar and Comoros.
COVID-19 testing capacity indicators (number of SARS-CoV-2 PCR tests performed and the positivity rate recorded in each country), cumulative through 29 November 2020
Non-pharmaceutical measures in response to COVID-19 pandemic
In response to the COVID-19 pandemic, African island nations followed similar response strategies to contain the spread of the virus and protect public health. All island nations decided to close their international borders soon after the detection of the first confirmed case (online supplemental figure S1). A state of emergency, accompanied by the implementation of lockdowns, was activated in all countries. More specifically, in Mauritius and Madagascar, this happened 2 days after official declaration of the pandemic, in Comoros after 4 days, in Cabo Verde after 8 days, in São Tomé e Príncipe after 17 days, and in Seychelles after 23 days (online supplemental figure S1). Some of these islands implemented protective measures even before the first case was detected in their territory. In these cases, the measures implemented were health screenings at points of entry, entry restrictions and testing, isolation and quarantine policies. More specifically, Mauritius and Comoros organised quarantine centres for the isolation of patients with COVID-19.43 No information about such facilities was available for the other countries. All countries enforced movement restrictions to contain the virus’ spread soon after confirmation of the first case in their territory.44 Tracking of these measures imposed by governments has been undertaken by Oxford University for many countries around the world since part-way through the first wave of the pandemic and are summarised in the ‘stringency index’ indicator qualifying the strictness of policies enacted to influence people’s behaviour.45 In online supplemental figure S4, we present the temporal evolution of the stringency index for four of the six African island nations (the index was not available for Comoros or São Tomé e Príncipe). All four islands implemented strict movement restrictions soon after the first COVID-19 case was confirmed. The level of strictness of the implemented measures did not differ considerably at the beginning of the outbreak. Seychelles and Mauritius removed most of the restrictions in June 2020 and Madagascar in September 2020, while Cabo Verde maintained most restrictions through the end of the study period (29 November 2020). Temporal analysis of the stringency index also reflects this tendency for governments to relax the measures as incidence subsided.
Conclusions
In a pandemic caused by a virus with respiratory transmission, where several containment measures were introduced simultaneously, it is difficult to evaluate the effectiveness of each measure in isolation. However, it appears that early implementation of control measures in the initial phase of global spread were crucial in containing the number of cases in most African island nations for the first few months of the pandemic. Similar results were reported in a study conducted on SIDSs in the Caribbean, where stringent control measures were also associated with lower levels of community spread.9 In the context of limited national resources, the closure of borders and the control of imported cases might have been both easier than in larger mainland populations and also more crucial for delaying community transmission while capacity for testing and patient care could be put in place.
The initial control of the spread of the infectious agent becomes even more important if we consider the factors that contribute to severe disease. As has been previously reported that NCDs increase the likelihood of serious symptoms and death from COVID-19. Most of our countries reported high premature mortality due to NCDs. Without the controls put in place, it is likely that rapid spread of the virus would have caused high hospitalisation and mortality rates and strained the under-resourced healthcare systems of these countries.
However, some of the African islands had more than just rapid and stringent control measures to aid in their pandemic response. Between countries, variation in capacity and policies present before the pandemic may have also had big impacts. For instance, Cabo Verde had the highest attack rate, but is a lower middle-income country that puts a high percentage of its GDP towards health services. With the highest density of health posts (33.4 per 100k inhabitants) of any other African island nation, and free testing made available from 29 May 2020, their capacity for case detection was likely higher than in islands where access to healthcare professionals or testing facilities was more limited. This could also be the reason for the country’s relatively low CFR, since higher testing capacity means there would have been less bias towards detection of severe cases.
High-income countries such as Mauritius and Seychelles had high capacity for response, including detection, but the relatively high burden of severe disease in Mauritius may have been due to the relatively higher frequency of both older age classes and other pre-existing risk factors for severe disease such as obesity.
In low-income countries where response capacity is severely limited, reliance on border closures is a double blow, since the economic impact is greater, which further weakens this capacity. The long-term impact of strict government responses on the health and well-being of these nations, particularly those with low proportions of underlying risk factors for severe COVID-19 disease such as the Comoros, should be carefully considered for motivating preparedness investment strategies for the future. Investments in surveillance (including testing) capacities and access to healthcare would likely be more economically and socially advantageous over the long term. No matter the wealth of the country, improvements to air quality and lifestyle (such as diet and exercise), which affect a large range of diseases, would also have played a role in limiting the impact of the severity of COVID-19 pandemic on Africa’s island nations.
The COVID-19 pandemic exposed the weaknesses in public health crisis preparedness and response capacities of the African island nations. Future work should investigate the long-term implications of the pandemic on the economies and societies of these countries. In addition, a global review of the challenges and impacts of COVID-19 response on island nations would help guide pandemic prevention, preparedness and response plans optimising the allocation of resources (whether abundant or limited, alike) available in these countries, which share specific geographic, social, and economic vulnerabilities.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
TK, DV, JD and AJ are joint first authors.
OK, JLA and CBH are joint senior authors.
Handling editor Seye Abimbola
Twitter @TheVetFuturist, @AnanthuJames, @jessieabbate
Contributors TK conceived the study with the support of JD, DV, AJ, JLA and CBH. TK, JD, DV, AJ designed and conducted research with the support of JLA and CBH. JD, TK, DV, AJ actively took part in weekly discussions and exchanged ideas that were crucial for the progress of this article. GSW, AB, TM, and FM verified the COVID-19 data and made it available for the public WHO COVID-19 dashboard. JD compiled, cleaned and analysed the data with the support of DCPC, AJ and JLA. JD, AJ, DCPC, JLA, TK and DV interpreted the data. TK and DV conducted the literature review with the support from AJ, JD and JLA. JD, TK, DV and AJ drafted the initial manuscript. AJ, JD, TK and JLA finalised the manuscript after improving it substantially. CBH, JLA, CC, OK, GSW, AB, TM, FM and BI made substantial contributions in reviewing the design of the study and contributed by revising the manuscript critically for important intellectual content. We also acknowledge and thank Laëtitia Viau for initially compiling a portion of the data used. All authors contributed to final approval of the submitted version.
Funding OK was funded by the Swiss National Science Foundation (grants number 163878 and 202660).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.