Article Text

Abstract
Background Access to health facilities in many low-income and middle-income countries remains low, with a strong association between individuals’ distance to facilities and health outcomes. Yet plausibly causal estimates of the effects of facility construction programmes are rare. Starting in 2004, more than 2800 government health facilities were built in Ethiopia. This study estimates the impact of this programme on maternal health service utilisation and birth outcomes.
Methods We analyse the impact of Ethiopia’s health centre construction programme on health service utilisation and outcomes, using a difference-in-difference design. We match facility opening years to child birth years in four rounds of Demographic and Health Surveys (DHS) using georeferenced data. We also use event study models to test for pre-trends in the outcomes of interest.
Results Opening of new health facilities within 5 km increases facility delivery by 7.2 percentage points (95% CI 5.2 to 9.1) and antenatal care by 0.38 visits (95% CI 0.24 to 0.52). It is not significantly associated with changes in caesarean section births or neonatal mortality. Opening of district hospitals increases facility delivery by 18.2 percentage points (95% CI 12.7 to 23.7), and caesarean section births by 6.8 percentage points (95% CI 2.5 to 11.2), but is not associated with reduction of neonatal mortality.
Conclusions Ethiopia’s facility construction program improved access to antenatal and delivery care. However, there was no detectable association between facility construction and neonatal mortality. Increased access to care must be combined with health system quality improvements and broader social development initiatives to sustainably improve health outcomes.
- health economics
- health systems evaluation
- maternal health
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
There are strong and robust associations between distance to health facilities and health service utilisation and child mortality.
However, it is difficult to interpret these associations causally because facilities may be built in more populated and economically dynamic areas, which introduces selection bias into estimates.
What are the new findings?
This study finds that Ethiopia’s health facility construction programme led to large and significant increases in key elements of maternity care such as facility delivery, antenatal care, and caesarean section delivery. There was no significant impact on neonatal mortality.
This research also shows that utilisation is affected differentially by the mix of services provided by facilities, with larger increases for more complex services like caesarean sections in communities close to new primary hospitals, compared to those close to lower level facilities.
What do the new findings imply?
This evidence suggests that reduced distance to health facilities increases utilisation of antenatal and delivery care in substantively meaningful ways.
These findings also highlight that geographic access to higher quality health facilities is needed to increase utilisation of more complex obstetric services such as caesarean sections.
Introduction
The WHO estimates that half of the people in the world do not receive the health services they need, and this problem is particularly acute for mothers and young children.1 Lack of access to care for pregnant mothers and young children is a major risk factor for maternal and child mortality, and the WHO has recommended skilled antenatal and delivery care as a key strategy to reduce maternal and neonatal mortality.2 3 While many countries have removed financial barriers to antenatal and delivery care, geographical barriers remain important, particularly for essential maternal and child health (MCH) services.4 A global push for the scale-up of primary healthcare has yielded investments in front-line health workers and lower-level facilities to provide essential health services, including antenatal and basic obstetric care.5 This push has emphasised infrastructure expansion, in line with the recognition that barriers to care can be geographic as well as financial or social. However, expansion of access to care via building large numbers of new facilities has also been contested on the grounds that existing facilities are often underused, many are poorly equipped and supervised, running costs may be unsustainable, and quality of care may not be sufficient to deliver improved health outcomes. For example, the 2018 Lancet Global Health Commission on High Quality Health Systems in the SDG Era has emphasised that increases in access alone mean little if the services provided are not of high quality.6
Starting in 2003, Ethiopia undertook a massive expansion of access to primary care via investment in physical infrastructure and in the health workforce. The country began expanding primary healthcare units by constructing and equipping primary hospitals and health centres which oversee a network of health extension workers (HEW) based at lower-level health posts. Over the time period studied in this paper, over 2800 health centres were built, 35 000 HEWs were trained and deployed, and over 15 000 health posts were constructed. In the Health Extension Program, young women with secondary education were trained for 1 year and deployed to communities to deliver health education and preventive and basic curative care to communities.
In this paper, we focus on construction of health centres and primary hospitals in areas which previously lacked access to such facilities. Most newly constructed facilities were health centres; these were designed as second-level health facilities, above the health post, but below the level of primary (district) hospitals.7 They were intended to serve catchment areas of approximately 15 000–25 000 people each, to be referral points to primary hospitals, and to be training sites for HEWs. The health centre construction programme was part of a broader expansion of primary care services: in accordance with Ethiopia’s Health Sector Development Plans, a contemporaneous influx of external funding supported a large set of programmes targeting MCH which were initiated over the 2003–2007 period.8 Government sources have credited this programme with increases in key utilisation indicators such as births occurring in health facilities.7 Despite this expansion of care, distance remains an issue in Ethiopia: for example, the 2011 Ethiopia Welfare Monitoring Survey reported that fewer than half (40%) of households live within 5 km of a health centre.9
We study the impact of the facility construction component of Ethiopia’s primary healthcare expansion programme on health services utilisation and health outcomes. Previous research has focused on the effects of HEWs, often showing correlations between HEW density and utilisation.10 11 However there has been little research focused on the expansion of the health facility network, despite the size and scope of these investments. Beyond Ethiopia, several studies show correlations between distance to health facilities and infant mortality or maternal mortality.12 13 A related literature shows negative effects of distance to facilities on use of antenatal and delivery care.4 For example, Hanson et al examine the relationship between changes in distance to health facilities and uptake of maternity services such as hospital delivery, primary facility delivery, antenatal care (ANC) and caesarean section births in Tanzania.14 In Ghana, Gabrysch et al find that living closer to facilities is associated with higher levels of facility delivery, but not with reduced mortality.15 Most of this literature relies on covariate adjustment to eliminate selection bias, or else seeks causal inference via instrumental variable strategies which rely on strong assumptions.16 By contrast our work exploits cohort variation in plausibly exogenous shifts in facility proximity, to identify the effects of proximity on access to services and health outcomes.
This paper estimates the impact of this facility building programme on MCH healthcare utilisation and health outcomes, focusing on facility births, ANC visits, caesarean sections and neonatal mortality. We focus on antenatal and maternity care since these are high volume interactions which may require contact with skilled health workers and well-equipped facilities (compared to other elements of primary healthcare, such as vaccinations, which are often delivered by lower level workers or via campaigns), and for which distance has previously been shown to be an important barrier. Moreover, most newly constructed facilities were designed to provide ANC as well as labour and delivery care. We focus on neonatal mortality as an outcome because it is plausibly affected by increased access to antenatal and skilled delivery care. Although maternal mortality could also be affected by these changes, the measurement of maternal mortality in the DHS questionnaire is not location-specific, and therefore cannot be linked to facility construction.
Methods
We use two primary data sources. To identify the location and year of opening of health facilities, we use a full census of public facilities conducted in 2014, which includes the date of facility establishment, from the master file created for the 2014 Ethiopia Service Provision Assessment Survey. While the full Service Provision Assessment survey was only carried out on a subsample of facilities within Ethiopia, the Federal Ministry of Health used the survey as an opportunity to capture a more limited set of information from all public facilities in the country.17 We use this list of all public facilities, their locations and the facility opening date. The earliest facility in the data was constructed in 1910; the most recent ones are from 2014, which is the year when the assessment was conducted. There are 3491 operational facilities in this data set. Facility opening years are missing for 54 of these facilities, which are dropped from the analysis.
Second, we use the four rounds of Demographic and Health Surveys (DHS) which have been conducted in Ethiopia.18–21 The DHS are nationally representative household surveys which have been fielded in Ethiopia in 2000, 2005, 2011 and 2016. The surveys contain detailed information on all children ever born to interviewed women in the sample, including survival (for all children) and medical care received by the mother before and at birth (for children born within 5 years of the survey). We include all records (one observation for every child born to surveyed women) for each of these four survey rounds. All births are georeferenced by a single Global Positioning System (GPS) point for the survey primary sampling unit. We define each survey cluster as having a nearby facility if it is within 5 km of a health facility contained in the facility census database. Births are defined as treated or not based on whether their survey cluster had a health facility within 5 km, and whether the birth took place before or after the facility opening year. The 5 km cut-off used to define access is roughly equivalent to a walking distance of 1 hour, which is a standard cut-off in rural areas.
The DHS cluster and health facility GPS coordinates were mapped onto zone and woreda shapefiles of Ethiopia using ArcGIS. These data were then exported to Stata to calculate distance for every facility-cluster combination. The distance between these DHS survey clusters and facilities was calculated using the ‘geodist’ command in Stata. There are 2314 survey clusters (primary sampling units) and 175 557 births in the data set that we created by aggregating cluster GPS coordinates and birth recode files from the 2000, 2005, 2011 and 2016 Ethiopia DHS (EDHS), with birth years spanning from 1963 to 2016. Restricting to those for which information about place of delivery is recorded (ie, births in 5 years prior to the survey) there are 42 966 births, spanning the period 1995–2016. Information about ANC is recorded for the most recent birth, among all women who have given birth in the 5 years prior to the survey, resulting in 28 631 observations. Place of delivery is missing for 50 out of 43 016 observations, number of ANC visits is missing for 148 out of 28 779 observations and whether or not a delivery was via caesarean section is missing for 2 out of 42 936 observations. There are 4570 (2.6%) missing values out of 175 567 observations for child survival. Observations are omitted from regressions where the dependent variable is missing.
We examine all outcomes using both the full sample (all observations) and subsamples of rural locations only (for the all-facilities analysis) and urban-only subsample (for the hospital-only analysis). There are valid theoretical reasons to expect that effects would be largest for rural households, as they are likely to have had the largest barriers to health access before new facilities are constructed. However, for confidentiality purposes, the geocoordinates of survey clusters in rural areas are randomly displaced by up to 5 km (and 1 out of every 100 clusters are displaced up to 10 km), mechanically introducing downward bias on average in estimates of effects. In urban areas, treatment effects of new facilities may be expected to be smaller, since pre-existing access to care was greater, but there is less measurement error, because cluster locations are only scrambled by up to 2 km. Accordingly, treatment effects will have less downward bias on average.
For subsample analysis focusing on hospital construction, we analyse the full sample, and the urban subsample separately, since very few primary hospitals were built near rural survey clusters. We also focus analysis on primary hospitals, since these hospitals were designed to provide the kinds of routine maternal health and delivery care services that we examine here, in contrast to general and referral hospitals, which provide more specialised care for complex conditions.
Statistical analysis
A standard problem in estimating effects of facility placement on health outcomes is that health facilities are placed deliberately rather than randomly. We use a difference-in-difference design, which exploits temporal and geographical variation in facility construction to lessen this potential bias. Without proper adjustment for deliberate facility placement, simple comparisons would retain bias in the estimation of treatment effects. The difference-in-difference design allows us to compare the difference between households located in locations which ever get a new facility to those which do not, and then the differential impact on births which take place after versus before a new health facility is constructed, while also controlling for time-invariant location characteristics and for temporal trends.
This design relies on the assumption that there were no differing trends prior to treatment between treated and untreated groups. We address this assumption via an event study analysis, which allows us to non-parametrically test for pre-trends in the variables of interest. When the pre-treatment coefficients of interest are indistinguishable from zero, but post-treatment coefficients are significant, we have greater confidence that the identifying assumptions of the difference-in-difference model hold.
We estimate treatment effects via linear probability models presented in equations 1 and 2. Equation 1 follows the standard difference-in-difference two-way fixed effects estimator, where i indexes individuals, and the specification includes fixed effects for child birth year cohorts (c) and zones (z), a term denoting whether a location cluster (l) ever had a facility within 5 km of it (‘any nearby facility’), and an interaction term which equals one for birth years which are in these clusters and where the child’s birth year is in or after the opening year of the health facility (‘birth after nearby facility opening’); we also include fixed effects for the year of the survey round (t). In cases where there is more than one health facility with 5 km of the survey cluster, the first facility built within 5 km defines treatment.
In addition to this two-way fixed effects model, we estimate event study models, which extend the difference-in-differences model by estimating separate indicator variables for a set of years prior to and after the treatment exposure occurs. This approach has several advantages. The first is that the pre-exposure coefficients can be interpreted as a ‘Granger-type causality’ test, on the assumption that future health facility construction should not have significant effects on outcomes for pre-construction birth cohorts.22 In addition, several recent papers have shown that two-way fixed effects models generate estimates which are weighted averages with differential weightings of different treatment years, which is problematic if treatment effects are not constant over time.23 In the event study models (equation 2), we calculate, for the ‘any nearby facility’ group, a variable which represents birth year relative to facility opening year. Indicator variables for each value (j) of this pre- and post-event variable can be included in estimation. Thus controlling for zone, birth year and survey round fixed effects as well as demographic and socioeconomic controls, we can estimate the impact of four pre- and post-event indicator variables on outcome (y) of interest. All births four or more years after or four or more years prior to facility opening are binned into indicators which equal one if the event was more or less than 4 years away from a given birth. These binned coefficients are not plotted. We omit the ‘t-1’ time period from the event study regression specification, following standard practice. Robust standard errors are clustered at the woreda (district) level. In both two-way fixed effect and event study models, we include a vector of socioeconomic and demographic controls (χ) for household wealth quintile, child’s gender, birth order, an indicator for multiple births and mother’s age and education.
 (1)
(1)
 (2)
(2)
In addition to these main effects, we also examine heterogeneity by the type of facility built (hospital vs health centre), by the education level of mothers, and by region.
We first examine heterogeneity across type of facility. 98% of the facilities built between 2003 and 2014 were health centres. However, 32 primary hospitals, 30 general hospitals and 5 referral hospitals were also built during this period. Services offered varied between hospitals and health centres. For example, while both health centres and hospitals typically offer antenatal and normal delivery care, only 1% of health centres offer caesarean sections, compared to 77% of primary hospitals.17 We examine heterogeneity in this dimension in order to see whether variation in complexity of services offered is reflected in utilisation patterns.
We examine the sensitivity of the main findings to the inclusion of different levels of regional fixed effects, such as region or district (woreda). Next, we examine whether results are robust to changing the distance that defines treatment ±3 km (ie, defining clusters 2 km or 8 km from health facilities as treated). Since analysis relies on the assumption that mothers live in the same community at the time of survey as they did when giving birth, we restrict the sample to mothers who report having lived in same location for a minimum of 5 and 10 years. The online supplementary appendix also contains event study graphs with standardised coefficients so that effect sizes can be compared across outcomes. For heterogeneity analysis by region and education level, we also substitute a binary outcome indicating whether or not a respondent attended four or more ANC visits in place of the continuous ‘number of ANC visits’ variable, so that plotted outcomes are easily visually comparable between the facility delivery and ANC outcomes.
Supplemental material
Role of the funding source
The funders had no role in study design, analysis, interpretation or writing. The corresponding author had full access to the data and had final responsibility for the decision to submit the study for publication.
Patient involvement statement
Patients were not involved in the design and implementation of this research.
Results
Figure 1 (panels A and B) shows the map of public health facilities in 2004 and 2014, demonstrating the scale and pace of the health centre construction initiative. More than 200 facilities were opened in every year between 2008 and 2013, peaking in 2010 when 626 facilities were opened.
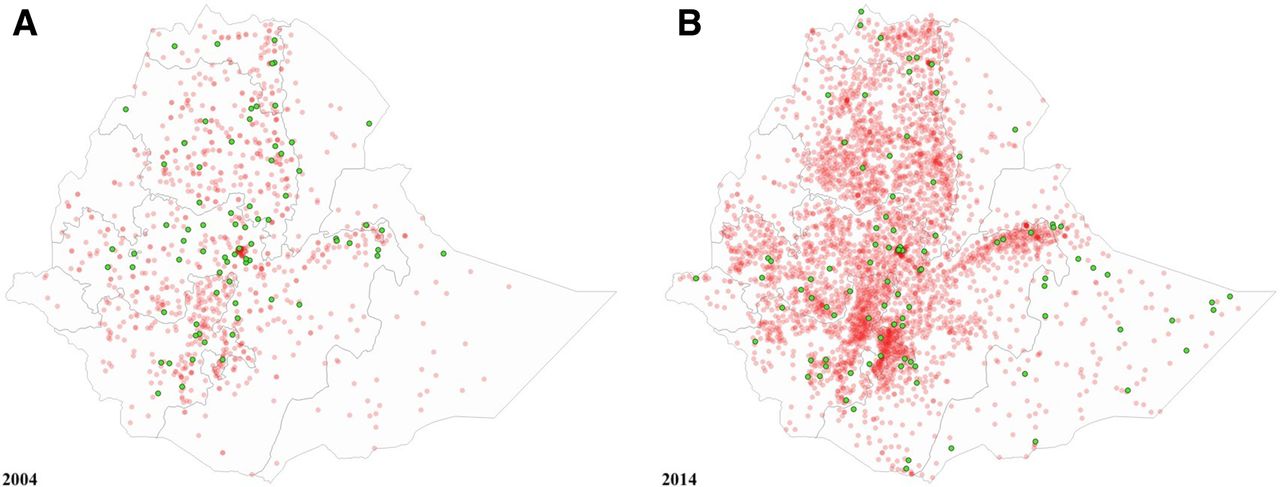
Public facilities in existence (red dots) and just opened (green dots) in 2004 and 2013. Facility locations and opening dates obtained from the 2014 facility census.
Table 1 presents characteristics of child births observed in the surveys. The sample of births is 48% female, 82% rural and mothers have an average of 1.9 years of education. Sixteen percent of births took place in health facilities, and the average number of ANC visits was 1.8. 2% of children were born via C-section, and 5% of children born did not survive the neonatal period.
Summary statistics
In the two-way fixed effects model (equation 1), having a health facility within 5 km increases facility delivery by 7.2 percentage points (95% CI 5.2 to 9.1), and increases the number of ANC visits by 0.38 (95% CI 0.24 to 0.52). There is no significant impact on caesarean sections (−0.10 percentage points, 95% CI −0.54 to 0.34) or neonatal mortality (−0.16 percentage points, 95% CI −0.56 to 0.24) in the full sample (table 2, panel A).
Effect of any health facility construction, two-way fixed effects model
In the rural subsample, the presence of health facilities increases facility delivery by 3.7 percentage points (95% CI 2.10 to 5.3), and increases the number of ANC visits by 0.23 (95% CI 0.09 to 0.36), but does not significantly increase caesarean sections (0.06 percentage points, 95% CI −0.28 to 0.40) and is not associated with significant reductions in neonatal mortality (−0.28 percentage points, 95% CI −0.78 to 0.22). (table 2, panel B)
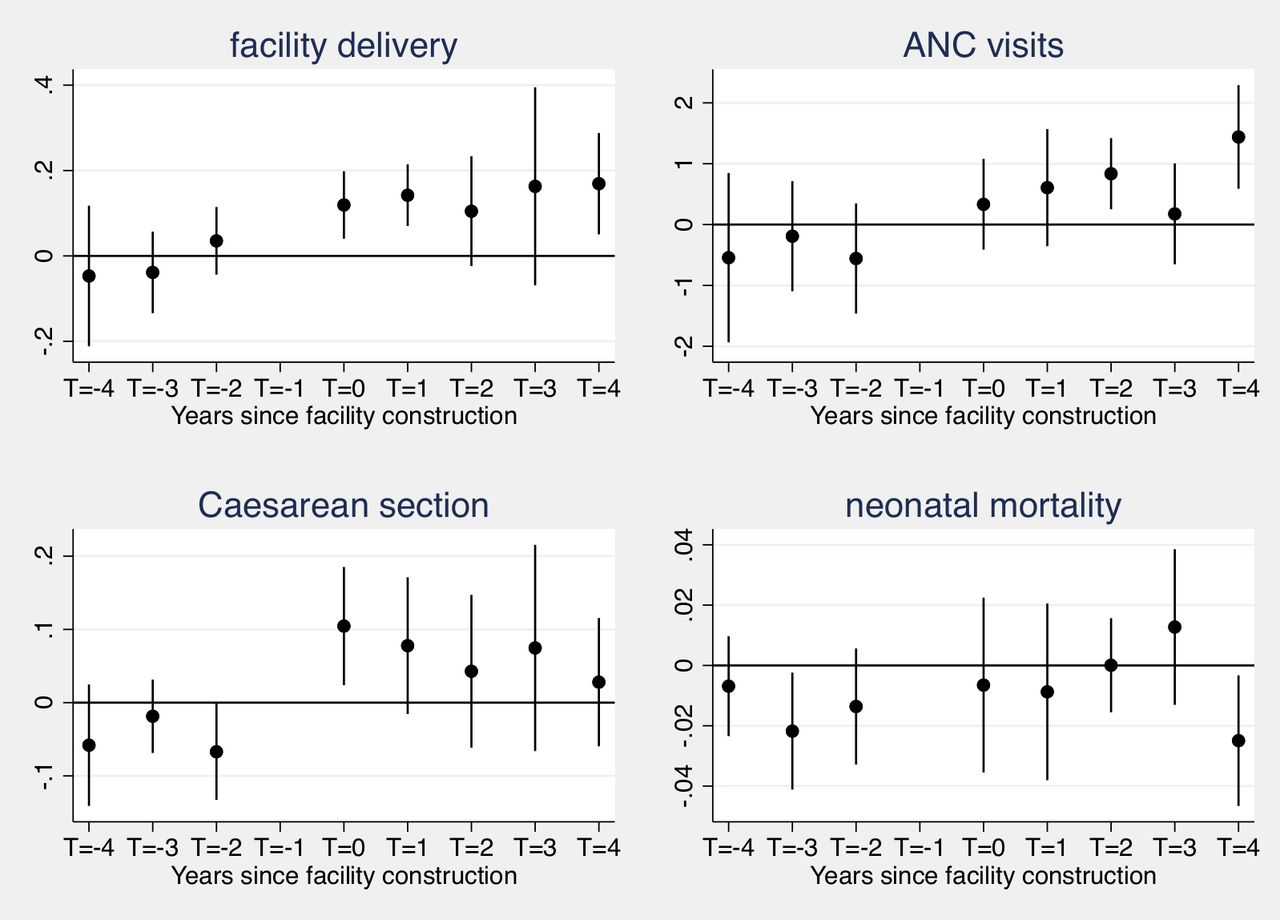
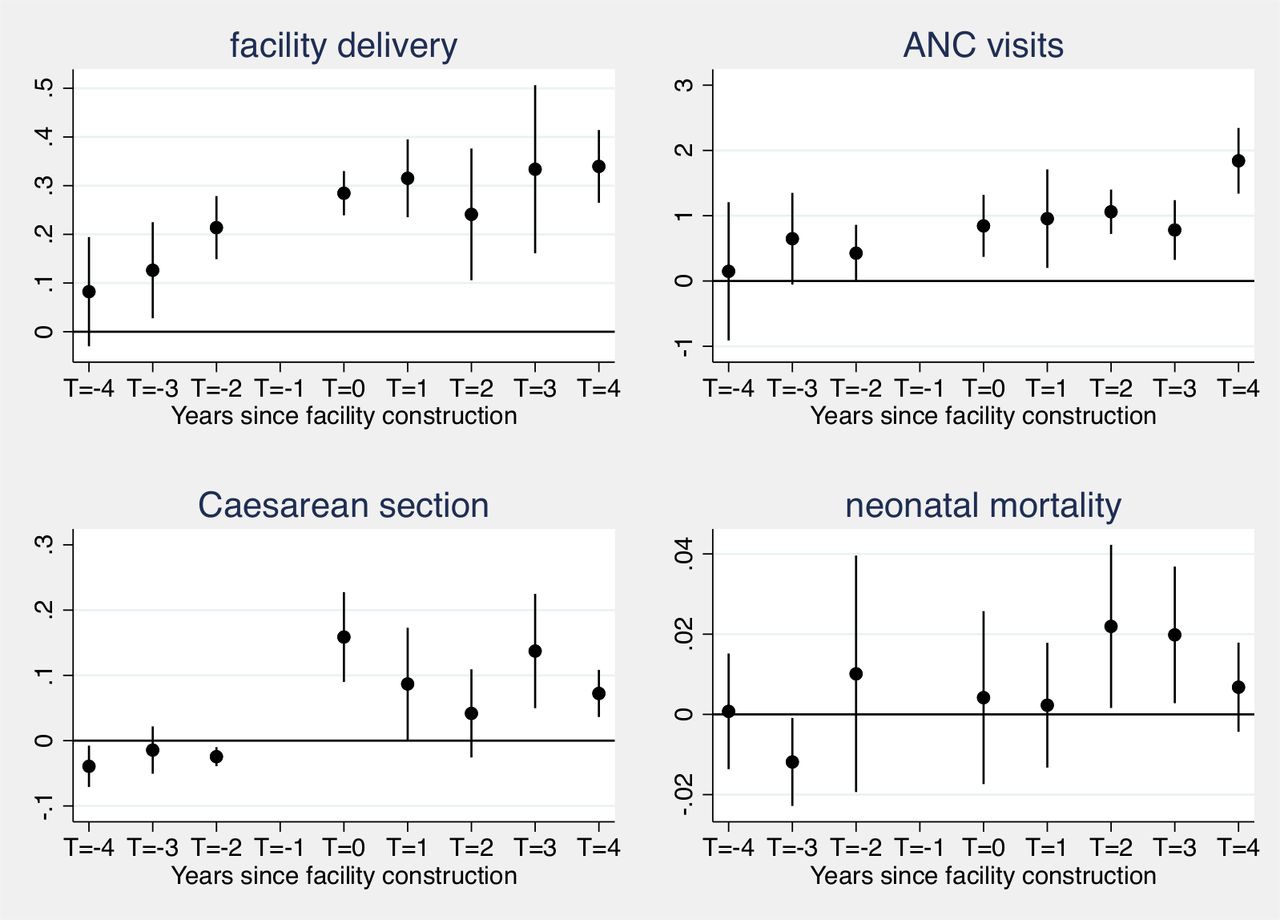
Using the event study model (equation 2), we test non-parametrically for pre-treatment trends in the outcomes of interest, and estimate the time path of treatment effects for each outcome. For facility delivery, ANC and caesarean sections, the pre-treatment coefficients for births 4, 3 and 2 years before facility construction are not statistically different than zero. Increases in facility deliveries and number of ANC visits are substantively large and significant by the time of births which take place 2–3 years after facility opening. For neonatal mortality, several pre-treatment coefficients are significantly negative (t-4, t-3). This indicates facility construction in settings with lower pre-treatment mortality, and suggests that mortality estimates should be interpreted as associations (figure 2). Similar patterns for pretreatment and post-treatment coefficients are present in the rural-only subsample (figure 3).

Health utilization and outcomes before and after local health facility opening, all locations

Health utilization and outcomes before and after local health facility opening, rural locations
Subgroup analysis
Shifting focus to births in clusters after primary hospital construction (rather than after construction of any health facility), there are significant increases in facility deliveries (18.2 percentage points, 95% CI 12.7 to 23.7) and caesarean sections (6.8 percentage points, 95% CI 2.5 to 11.2). The point estimate for ANC visits is 0.25 (95% CI −0.02 to 0.52), and for neonatal mortality the point estimate is 0.7 percentage points (95% CI −0.1 to 1.5). When analysis includes all hospitals (primary, general and referral hospitals), results are broadly similar (table 3, panel C): The increase in facility deliveries for all hospitals is 15.1 percentage points (95% CI 8.5 to 21.8) and the increase for caesarean sections is 2.2 percentage points (95% CI 0.5 to 3.8).
Effect of hospital construction, two-way fixed effects model
In the event study framework, there is evidence of positive pre-trends for facility delivery and to a lesser extent for ANC visits, though not for caesarean sections (figure 4). As such, for facility delivery and antenatal care, coefficients for births taking place 2–4 years after facility opening (t+2, t+3, t+4) likely reflect both increases relative to (positive) pre-facility opening trends as well as unobserved selection effects. However, when the sample is restricted to urban areas, there are no significant pre-trend across any outcomes, yet treatment effects remain large and significant for facility delivery, ANC and caesarean sections (figure 5). In both the full sample and urban subsample, large increases in facility delivery and caesarean sections occur immediately (ie, starting with births in the year of hospital opening).

Health utilization and outcomes before and after local primary hospital opening, all locations
Health utilization and outcomes before and after local primary hospital opening, urban locations
Effects are larger for mothers with some education versus mothers with no education for facility delivery, but not for other outcomes. We also examine effects across Ethiopia’s regions. Effects are similar across regions for facility delivery, with the exception of the limited treatment effect in the Southern Nations, Nationalities, and Peoples' (SNNPR) region. For caesarean section, effects are larger in the Amhara, Oromo and Tigray regions than in the more remote Somali and Afar regions. The are no regional differences in the effects on neonatal mortality (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Health utilization and outcomes by mother’s education level and by region of residence. Plotted coefficients are from two-way fixed effects model.
We test whether the results are sensitive to changes ±3 km in the distance threshold that defines treatment, to inclusion of higher or lower level geographical fixed effects, and to exclusion of individuals who have moved with the last 5 or 10 years. Results are robust to each of these tests (online supplementary appendix tables A1‒A3).
Discussion
This paper uses secondary data to estimate the impact of a high profile, globally recognised, at-scale primary healthcare programme that comprised major investment in physical facility construction, together with complementary investments in staffing, equipment and community outreach. In doing so, we show that the facility construction component of Ethiopia’s flagship health programme improved access to antenatal and delivery care. However, we do not find evidence of reduced neonatal mortality. The empirical design lends credibility to the conclusions by ensuring valid counterfactuals, and is able to show dynamic treatment effects over time.
For facility deliveries and number of ANC visits, significant effects emerge most clearly 2–3 years after facility construction in the full sample. This is consistent with programme design in which additional community level interventions (health posts, HEWs) were often rolled out after health clinics were constructed, and in which health worker deployment may have lagged facility opening. By contrast, for primary hospital construction, increases are visible for cohorts born immediately after facility opening; most notably there is a large and discontinuous increase in caesarean sections for mothers who live near newly constructed primary hospitals, which are more likely than health centres to have surgical capability. While health centres typically do not have surgical capacity, they could in theory increase caesarean sections by generating more rapid referrals to surgically equipped facilities for high risk pregnancies. However, we do not see evidence of this mechanism. In addition, we lack data to ascertain whether these caesarean sections were in response to medical need. Since only 2% of births are by caesarean section in the full sample, this suggests that caesarean sections remain significantly underprovided and increases are likely warranted.
An important contextual factor is that access to health facilities was highly limited prior to the programme. In addition, Ethiopia has a relatively small private health sector, suggesting that these newly constructed public facilities were unlikely to be crowding out previous private facility usage. The increases in utilisation observed in this study may also reflect that the facility construction campaign was part of a national commitment to expanded health access and improved care, with high-level political commitment. Accordingly, these estimates of the effect of health centres may also reflect complementary investments that were made in hiring additional clinical officers and midwives at health centres. In addition, it may reflect the activities of Ethiopia’s HEWs, who starting in 2003 were deployed to newly constructed health posts. While not directly providing most MCH services themselves, HEWs may have increased uptake of maternal and child services through their outreach activities for pregnant women. In the final years of our sample (post 2012), the activities of extension workers were intensified by the ‘Health Development Army’ programme which mobilised women into ‘1 to 5’ groupings through the country, and also referred pregnant women for facility delivery.
The estimated 6.8 percentage point increase in facility delivery can be compared with other programmatic efforts to increase maternal healthcare utilisation in low income settings, such as cash transfer programmes to pregnant mothers. In Kenya, Grepin et al find that an unconditional cash transfer plus a voucher increase facility delivery by 12 percentage points.24 Powell-Jackson et al estimate an increase in facility delivery of 7.5 percentage points from India’s Janani Suraksha Yojana (JSY) programme.25 De Brauw and Peterman estimate at least a 15.3 percentage point increase in hospital births from El Salvador’s Conditional Cash Transfer programme.26 More work on the relative cost effectiveness of different strategies to increase uptake of MCH services, as well as their benefits on non-MCH health, is warranted.
Another way to contextualise the effect sizes estimated here are relative to the gaps between socioeconomic groups in Ethiopia. For example, the effect size of 6.8 percentage points is 22% of the gap in facility delivery rates between mothers with no education and those with at least some formal education, and 17% of the gap in number of ANC visits between these two groups.
A limitation of our study relates to the scrambling of DHS locations, which introduces error into estimates of proximity.27 However, this creates classical measurement error in the independent variable of interest which is likely to on average bias treatment effects towards zero. This may also help to explain the smaller treatment effect estimates obtained in rural areas. Ex ante, we would expect larger treatment effects in rural areas which have less access to care before facility construction. However, rural clusters are displaced by 5 km, compared to 2 km in urban areas. Accordingly, treatment effect estimates in urban areas may exhibit less attenuation bias.
A second limitation is that this study incorporates relatively limited information about the quality of care. The recent Lancet Commission on High Quality Health Systems in the SDG Era has argued that minimisation of distance should not be the main criteria for health planning, as having women give birth in poorly equipped low-level facilities may not improve outcomes.6 Key factors in ensuring that improved access to facilities results in reduced mortality will be to ensure that the new facilities deliver quality services, and that the facilities are maintained at appropriate levels of staffing and supply over time. Donor financing was critical for the start up phase of Ethiopia’s primary healthcare programme, but continued economic growth and increased domestic revenue mobilisation and allocation to health will be critical to maintenance of these primary healthcare investments over time.28
We find no associations between facility construction and reduced neonatal mortality in the full sample with all controls, despite significant increases in facility delivery and ANC utilisation. This may reflect limited statistical power to detect mortality reductions; for example, the SE of the main sample coefficient of interest is 0.002 (0.2 percentage points), implying that the minimum detectable effect is approximately a 0.4 percentage point reduction; this represents an 8% reduction of the sample mean of 5.0%. The observed increases in antenatal and delivery care may not have been sufficient to bring about this magnitude of reduction in mortality. Increases in access to care were largest when hospitals, rather than health centres, were constructed. However since there were fewer hospitals constructed, and they were largely built in urban settings, statistical power remained limited to detect mortality impact, and residual confounding remains possible.
Ethiopia’s investment in primary health care infrastructure has been widely praised, but there has been limited comprehensive, national evidence to date on the health impact of this program. These findings can inform other low and middle income countries considering large scale investments in primary health infrastructure as part of efforts to achieve the Sustainable Development Goals.
Acknowledgments
The authors would like to acknowledge research assistance from Shruti Korada.
Footnotes
Handling editor Sanni Yaya
Contributors All authors contributed equally to the paper.
Funding World Bank Development Economics Group Research Support Budget and Harvard T.H. Chan School of Public Health Dean’s Fund for Scientific Advancement.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All DHS data are freely available from measuredhs.com. Facility location data was obtained from Ethiopia Public Health Institute (EPHI). The authors are not at liberty to share this data, but it can be requested from EPHI.