Article Text

Abstract
Universal health coverage (UHC) has been identified as a priority for the global health agenda. In 2009, the Chinese government launched a new round of healthcare reform towards UHC, aiming to provide universal coverage of basic healthcare by the end of 2020. We conducted a secondary data analysis and combined it with a literature review, analysing the overview of UHC in China with regard to financial protection, coverage of health services and the reported coverage of the WHO and the World Bank UHC indicators. The results include the following: out-of-pocket expenditures as a percentage of current health expenditures in China have dropped dramatically from 60.13% in 2000 to 35.91% in 2016; the health insurance coverage of the total population jumped from 22.1% in 2003 to 95.1% in 2013; the average life expectancy increased from 72.0 to 76.4, maternal mortality dropped from 59 to 29 per 100 000 live births, the under-5 mortality rate dropped from 36.8 to 9.3 per 1000 live births, and neonatal mortality dropped from 21.4 to 4.7 per 1000 live births between 2000 and 2017; and so on. Our findings show that while China appears to be well on the path to UHC, there are identifiable gaps in service quality and a requirement for ongoing strengthening of financial protections. Some of the key challenges remain to be faced, such as the fragmented and inequitable health delivery system, and the increasing demand for high-quality and value-based service delivery. Given that China has committed to achieving UHC and ‘Healthy China 2030’, the evidence from this study can be suggestive of furthering on in the UHC journey and taking the policy steps necessary to secure change.
- health policy
- health systems evaluation
- public health
- health insurance
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Universal health coverage (UHC) has been identified as a priority for the global health agenda in many countries, including China.
Out-of-pocket expenditures as a percentage of current health expenditures in China have dropped dramatically.
The health insurance reform is achieved in the breadth of coverage in the population, the comprehensiveness of the benefits packages and increased reimbursement rates.
The coverage of healthcare services greatly progressed in terms of accessibility, equity and quality, but it remains to be improved in some aspects, such as quality in non-communicable diseases.
Taking the next steps is suggested when the Chinese government encounters some key challenges to achieve UHC.
Introduction
Universal health coverage (UHC) has been identified as a priority for the global health agenda. UHC means that all people can access the health services they need, without suffering financial hardship,1 and became a critical part of the Sustainable Development Goals (SDGs) in 2015.2 In September 2019, all United Nations Member States have committed strongly to achieve UHC by 2030, with the global effort to build a healthier world for all.3 Measuring progress towards UHC is complex due to the different political contexts among countries. In 2015, the WHO and the World Bank (WB) jointly launched a monitoring framework for UHC and reported the first global assessment of the progress towards UHC. Subsequently, a second report was published in 2017, more specifically monitoring SDG 3 target 3.8. The second framework built on two SDG UHC indicators: coverage of essential health services (target 3.8.1) and financial protection (target 3.8.2).1 Such an evaluation framework will provide guidance for assessing UHC in a country and tracking progress over time, and be meaningful in making cross-country comparisons.
Since the Chinese government launched a new round of health system reform in 2009, China has made tremendous efforts to achieve the long-term objective of UHC—providing affordable and equitable basic healthcare for all by 2020.4 A series of comprehensive healthcare reforms have been adopted step by step, including the expansion of healthcare insurance, making basic public health services available and equal for all, establishing a national essential medicines system, improving the primary care delivery system to provide basic healthcare, and the reform of public hospitals.5 This year marks the 10th anniversary of the healthcare reform. It is especially timely and significant to assess and track progress towards UHC in China. However, very few evaluations have been conducted on this issue.
This study aims to analyse China’s progress towards UHC in the past 10 years of healthcare reform, based on two dimensions: financial protection and coverage of health services. We also tracked UHC indicators by the latest WHO and WB framework in our analysis, and conclude with a discussion of the remaining challenges towards UHC. Due to the constraints of the available data, we conducted a secondary data analysis from multiple sources: public databases (eg, WHO and WB), related reports, the China Statistical Yearbook, the National Health Services Survey (NHSS) in China and so on. To present a comprehensive and detailed picture of UHC in China, we combined our analysis with a literature review and summarised findings from the peer-reviewed original research. The search method, search strategy and included papers are listed in online supplementary file 2. Findings from this analysis will provide evidence for policy-makers on the path to achieving UHC and recommendations for the next step moving forward in China.
Supplemental material
Financial protection
Financial protection is critical to reaching UHC, as all citizens should have access to health services without suffering financial hardship. Figure 1 shows the trends in the core indicators of health systems financing in China and the members of the Organisation for Economic Co-operation and Development (OECD) between 2000 and 2016. Compared with OECD members, China spent less of its gross domestic product on health, but the total health expenditures still grew. Although Chinese government spending on health increased to 9.05% of its total expenditure in 2016, it is far less than the share of OECD countries. The out-of-pocket spending is a key indicator with regard to financial protection. Out-of-pocket expenditures (OOPE) as a percentage of current health expenditures in China have dropped dramatically from 60.13% in 2000 to 35.91% in 2016, but remain significantly higher in China than in OECD member countries. The amount of OOPE per capita continued to increase.6Online supplementary figure S1 shows the total health expenditure composition in China from 2000 to 2018. As for the indicator of catastrophic health expenditure, recent national studies showed that China made progress in reducing the rate of catastrophic health expenditure, especially for low-income groups.7 8 However, the financial burden for medical services of patients remains high.9 10
Supplemental material

Trends in the core indicators of health systems financing in China and OECD members between 2000 and 2016. The core indicators are according to the ‘Health Systems Financing-Toolkit on monitoring health systems strengthening, WHO, 2008’. Source: The World Bank data (https://data.worldbank.org; last updated: 8 October 2019). CHE, current health expenditure; GDP, gross domestic product; GGE, general government expenditure; GGHE-D, domestic general government health expenditure; OECD, Organisation for Economic Co-operation and Development; OOPE, out-of-pocket expenditure.
The achievements of health insurance reform in China are impressive for both the scale of coverage expansion and the speed of expansion.11 The NHSS showed a rapid increase in coverage over the past decade for both the urban and rural populations (figure 2). The health insurance coverage of the total population jumped from 22.1% in 2003 to 95.1% in 2013. The gap of insurance coverage was greatly narrowed between the urban and rural areas, reducing inequality. According to the evaluation framework on health insurance programmes coverage by Lagomarsino and colleagues,12 we examined the coverage of basic social health insurance programmes in China across three dimensions: who is covered, what is covered and how much is covered (table 1). Significant achievements were realised on the breadth of coverage in the population, the comprehensiveness of the benefits packages and increased reimbursement rates. In 2018, 1.34 billion people participated in the basic health insurance nationwide, with a steady coverage of more than 95%.13 In each insurance scheme, the benefit of health service package was improved, and the number of pharmaceuticals on the drug list was expanded to 2643 in 2019. Currently, there is no variation in the number of drugs covered by the different insurance schemes. Along with an increase in the per capita premiums for the Urban Resident Basic Medical Insurance and the New Rural Cooperative Medical Scheme, government subsidies per capita have increased more than fivefold in 2018 compared with 2009. China’s health insurance system has been proven to be effective in boosting the utilisation of healthcare services and alleviated the financial burden of patients.14 15 The integration of fragmented health insurance schemes could promote access to and improve equity in healthcare utilisation for rural residents.16 17 However, some of the populations, such as children,18 lower income groups19 and rural-to-urban migrants,20 21 have a lower rate of insurance coverage.

Changes in the basic health insurance coverage of the survey population in different years. UEBMI, NRCMS and URBMI were established in 1998, 2003 and 2007, respectively. Adapted from ‘the fifth national health service survey analysis report in 2013’.39 NRCMS, New Rural Cooperative Medical Scheme; UEBMI, Urban Employee Basic Medical Insurance; URBMI, Urban Resident Basic Medical Insurance.
Three dimensions of coverage on basic social health insurance programmes in China
Coverage of health services
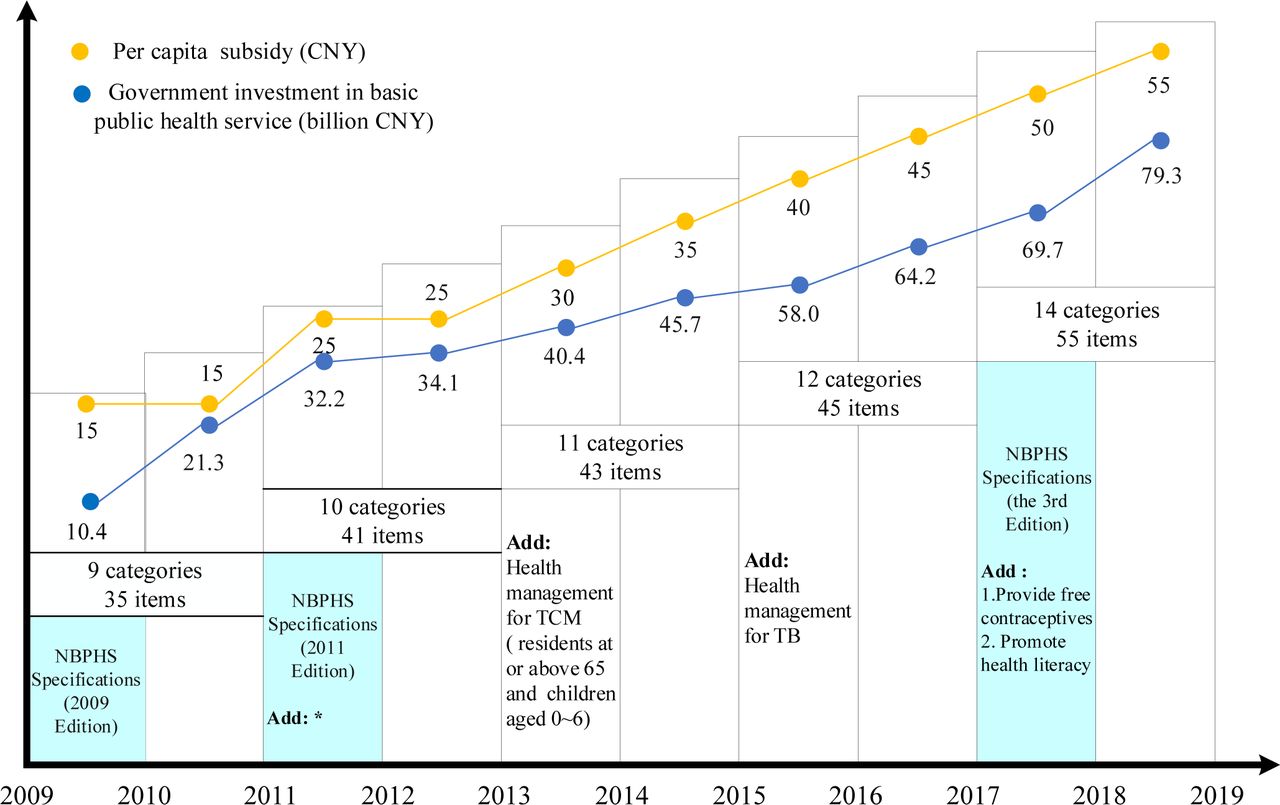
The national Basic Public Health Service (BPHS) programme was launched in 2009 to provide free basic public health services for all urban and rural residents equally. Figure 3 shows the Chinese government’s efforts in this area. To regulate the guideline for basic services, three editions of BPHS specifications were issued in 2009, 2011 and 2017, respectively. The initial service package consists of nine categories, including health archive management, health education, vaccination, communicable disease reporting, health management for children, maternal and elderly, and health management for chronic diseases and severe psychosis. Increased government public funding was invested to expand the services (14 categories in 2017) and availability of the basic public health package to almost everyone. An average of ¥15 was allotted per capita in 2009 and was increased to ¥55 in 2018. Following the previous literature, findings of the studies showed the following: the coverage of BPHS has increased greatly, but it has not reached the goal of universal coverage,22 23 especially coverage of migrants24 25; the utilisation of the BPHS is generally improved, but some of the services are underutilised26 27; ensuring equal access to the basic public health services is improved,28 29 and the gaps between urban–rural areas and different regions have been narrowed, but inequality still exists24 30 31; and with respect to the effects of the BPHS policy, there are some improvements in maternal health services and reductions in maternal mortality,32 and improved the treatment and control among patients with hypertension and type 2 diabetes.33 34 New evidence from the Global Burden of Disease Study showed that China has made substantial progress in reducing the burden of many diseases and disabilities.35

Changes in NBPHS programme, 2009–2018. Sources: Data on government investment in basic public health service are from the National General Public Budget Expenditure of National Government Final Accounts released by the Financial Ministry of the People’s Republic of China every year from 2009 to 2018. Data on per capita subsidy are from the news and Statistical Bulletin released by the National Health Commission of the People’s Republic of China. Data on basic public health services are from National Basic Public Service Specifications in 2009, 2011 and 2017, and Qin’s and Wang et al’s research.90 91 *Public health emergency reporting and assistance for health inspection, and the target services group for children’s health management extended from 0–3 years to 0–6 years. CNY, Chinese yuan; NBPHS, national Basic Public Health Service; TB, tuberculosis; TCM, traditional Chinese medicine.
According to the China Health Statistics Yearbook, the utilisation of medical services increased between 2009 and 2018: the outpatient visits increased from 518.7 million to 797.8 million, the hospital admissions increased from 132.6 million to 254.5 million, and the annual resident hospitalisation rate increased from 9.95% to 18.27%. Accordingly, both the number of visits to hospitals and primary care institutions (PCIs) increased. However, the percentage of visits delivered by hospitals among all healthcare institutions increased from 35.02% to 43.06%, while the proportion accounted for by PCIs dropped from 61.82% to 53.04% (figure 4). It indicates the current disordered situation—medical services are increasingly concentrated in hospitals rather than in primary care.

Comparison of the visits in hospitals and primary healthcare institutions, 2009–2018. Sources: China Statistical Yearbook, 2010–2018; China Health Statistics Yearbook, 2019. H, hospital; PCI, primary care institutions.
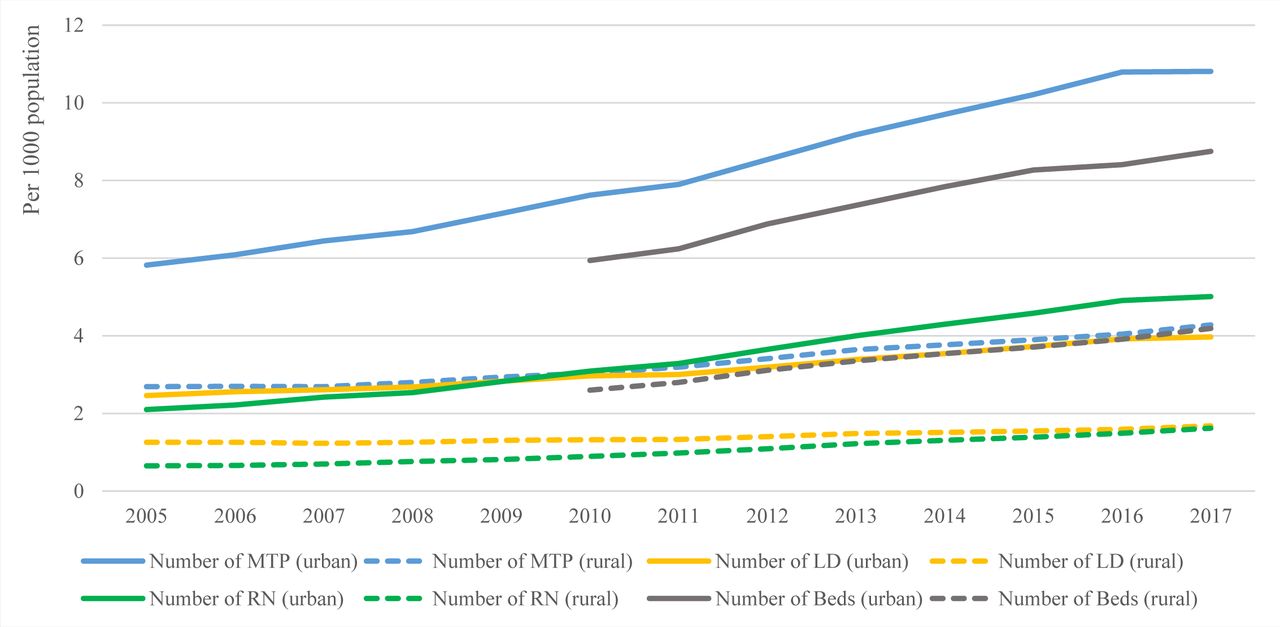
Delivering healthcare services in an accessible and equitable manner is essential to the goal of UHC. Access to health services has improved since the healthcare reform of 2009,36 37 but regional disparity is also apparent.37 38 Compared with 2008, the proportion of people who were not hospitalised due to financial difficulties decreased significantly, from 17.6% in 2008 to 7.4% in 2013.39 It indicated that the affordable access to healthcare services was improved, but some studies showed that the financial burden remains heavy,40 41 and the current reform has not resulted in access to affordable quality care.42 With the increase in government investments, the total amount of healthcare resources has increased in China and the equity of health resource allocation improved gradually.43–45 However, inequity in healthcare resources and services still existed. The inequitable determinants may relate to region,46 income47 and insurance type.46–49Figure 5 shows the gap between urban and rural areas in resource allocation. Between 2005 and 2017, the number of medical technical personnel, licensed (assistant) doctors, registered nurses and beds per 1000 population in urban areas grew more than in rural areas. According to the fifth NHSS in 2013, maternal and child health indicators (eg, the proportion of women receiving at least five antenatal check-ups, the proportion of children qualifying physical examination) in Central China were the poorest of the three regions (Western, Central and Eastern China). To achieve ‘effective UHC’, ensuring good quality of healthcare services should be emphasised as well.50 51 According to a recent global study, China has significantly increased personal healthcare access and quality, with an increase in the Healthcare Access and Quality Index (HAQ) score from 56.2 in 1990 to 78 in 2016.52 Although large HAQ score gaps remain between subnational regions, the expanded coverage of health services has led to health improvements, particularly for residents in rural areas. During the period between 2000 and 2017, the average life expectancy increased from 72.0 to 76.4, maternal mortality dropped from 59 in to 29 per 100 000 live births, the under-5 mortality rate dropped from 36.8 to 9.3 per 1000 live births, and neonatal mortality dropped from 21.4 to 4.7 per 1000 live births (online supplementary file 1, table S1). The differences in the neonatal, infant, under-5 and maternal mortality rates between urban and rural have greatly narrowed (figure 6).
Supplemental material
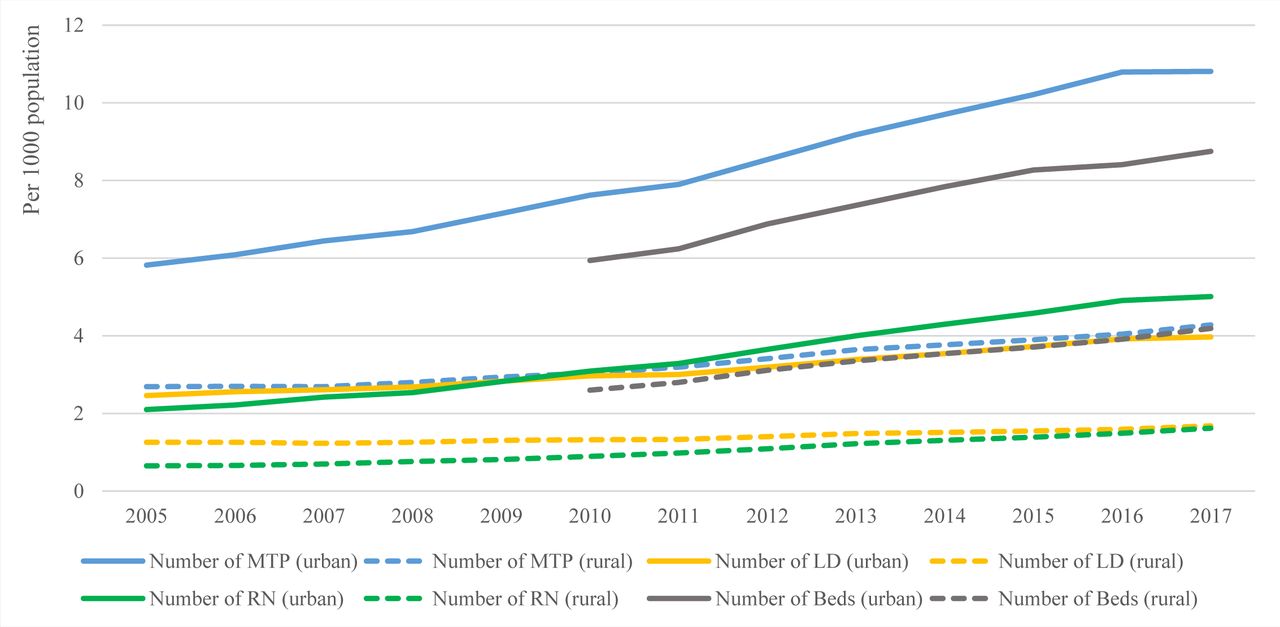
The gap between urban and rural medical resources, 2005–2017. Source: China Statistical Yearbook, 2006–2018. LD, licensed (assistant) doctors; MTP, medical technical personnel; RN, registered nurses.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Neonatal, infant, under-5 children and maternal mortality rate between urban and rural areas, 2000–2018. Source: China Health Statistics Yearbook, 2019. IMR, infant mortality rate; MMR, maternal mortality rate; NMR, neonatal mortality rate; U5MR, under-5 mortality rate.
Health services, broadly understood, also include the provision of drugs, devices and other goods, especially the essential medicines.53 Assuring access to essential medicines is also crucial for moving towards UHC.54 As part of the commitment to giving every citizen access to basic healthcare, China implemented the National Essential Medicines Policy (NEMP), which aims to increase the availability and affordability and to ensure the quality and promote the rational use of medicines. Since the revision of the National Essential Medicines List (NEML) issued in 2009, the list has been updated constantly from 307 medicines (2009) to 520 medicines (2012) and 685 medicines (2018), for fully meeting the needs of basic healthcare.55 Based on the literature review on the evaluation of the effects of the NEMP, there is no consensus conclusion. Differences in research conclusions may be due to the use of data from different regions, research period or study design. But overall, these findings have demonstrated that the NEMP interventions are effective: the availability of essential medicines had improved,56 57 but remains at a low level58 59 and had a problem of regional inequity60; drug prices were reduced significantly,57 61–63 and the affordability of essential medicines has improved57 59 60; and the rational use of medicine has effectively improved, but remained poor.56 64–67 In the subjective questionnaire surveys, patients were satisfied with the price and quality of essential medicines.68 However, village doctors were unsatisfied with the NEML; most of them believed that the NEML could not meet the needs of the villagers.69
Monitoring and evaluation of UHC indicators
To evaluate China’s UHC and compare it with other countries, we used the indicator framework defined in the Joint WHO/WB report entitled ‘Tracking Universal Health Coverage: 2017 Global Monitoring Report’.1 China has comparatively high coverage of essential health services but a low score for financial protection against catastrophic health expenditures. We analysed secondary data from international and national data sets to evaluate trends in indicators (refer to online supplementary figure S2 for the trends from 2000 to 2017, and online supplementary file 1, table S2 for detailed indicators and data sources).
Supplemental material
In terms of health service coverage, all indicators demonstrate improvement, with the exception of family planning. However, the level of demand satisfied by modern methods in 2017 (80.5%) is considered high, which is more than 75%.70 The largest relative increases are for tuberculosis (TB) and HIV treatment, which are consistent with global trends. This reflects China’s concerted efforts in the prevention and treatment of infectious diseases, for example, national ‘Action Plans’ to stop TB and HIV.71 72 However, progress in non-communicable diseases has been slower; in particular, blood glucose control (diabetes management) is deteriorating. Although the number of patients covered by type 2 diabetes management (including screening, regular follow-up and health education) increased from 18.5 million in 2011 to 31.2 million in 2017, blood glucose control rate has remained persistently low, indicating that the expanded service coverage may lack quality.73 More efforts are needed to develop effective strategies to control chronic diseases.
The upward trends in hospital beds, physicians and health security indicate greatly improved service capacity and access. In terms of financial protection, the risk of financial hardship due to out-of-pocket healthcare costs increased during 2000 and 2007, as measured by a growing incidence of OOPE exceeding 10% or 25% of household total consumption or income and an increased incidence of impoverishment at the $3.10 per day poverty line. However, the poverty gap due to OOPE (ie, the average per capita amount by which OOPE pushes or further pushes households below the poverty line)1 decreased for both poverty lines.
Challenges and policy recommendations
China has made unprecedented achievements on the path to realising UHC, but still faces a series of challenges when the healthcare system is subjected to multiple and persistent pressures, such as the changes in the distribution of diseases, urbanisation and a rapidly ageing population.
China’s healthcare system is facing a considerable challenge of fragmented healthcare delivery: hospital-centred and treatment-dominated. The current healthcare services in China still rely on hospital care, and PCIs do not play an important role in providing the basic healthcare with the first level of contact. Patients prefer to seek care in higher level of hospitals instead of primary healthcare (PHC) providers due to various factors, such as equipment and drug availability, medical staff, and perceived quality of primary care.74 75 The overdependence on hospital care not only leads to heavy financial burden and barriers to accessing basic healthcare, but also makes it difficult to form effective and continuous management of chronic diseases. There is a need for urgency in transition from fragmented care to integrated care in China’s healthcare systems. The key solution is the establishment of a tiered healthcare delivery system based on a people-centred integrated care model that can coordinate the PHC and hospital care.76 77 Thus, the service integration between PCIs and higher-level hospitals can be achieved through two-way referral, cooperation and information sharing among providers and between providers and patients, and active patient involvement in their continuous care.78
The second challenge is the persistent inequity in healthcare delivery between urban and rural areas, and among different income regions. Despite substantial improvements in access to health services and the dramatic reductions in poverty, inequalities still exist. Urban–rural disparities in financing and health services access are major issues in China when promoting UHC.79 Given China’s urban–rural dualistic economic structure, uncoordinated development in the healthcare system has led to more and better healthcare resources in urban areas,80 especially with regard to health personnel, and the differences in regional economic development tend to be the cause of the regional inequity. China needs to make more progress with respect to equity in healthcare in the future healthcare reforms. Except that policy is tilted in favour of resource-poor regions, the development of the Healthcare Alliance (HCA) is a priority issue. HCA refers to a collaborative alliance or medical group consisting of different types and levels of healthcare organisations in the same region or across regions. It is able to promote optimal healthcare resources allocation and flow, and improve the capability of primary care. Based on the HCA, strengthening the health information technology, such as mobile health and telemedicine, can help solve regional disparities and shortage of health personnel (especially for the low-income and remote areas) and promote homogenisation of healthcare services. At the same time, we need to coordinate the reform of medicine and health insurances to improve health equity.
The third challenge is to develop health services that can meet the emerging health needs of socioeconomic and demographic transitions. Given the rapidly rising incidence of non-communicable diseases and a rapidly ageing population, the health strategy should shift from treatment to prevention, calling for more comprehensive approaches to serving population health rather than solely the patient’s health.81 82 Meanwhile, with increased economy and improved lifestyle, people are demanding more and better healthcare. More attention should pay to building high-quality and value-based service delivery.78 The coverage of basic health services has been basically achieved; therefore, improving the quality of services is the next step.
Conclusion
This analysis gives an overview of UHC in China with regard to health financing, healthcare services and the reported coverage of WHO/WB indicators. It is the first attempt to integrate WHO/WB framework into a summary measure of UHC in China. Our findings show that while China appears to be well on the path to UHC, there are identifiable gaps in service quality and a requirement for ongoing strengthening of financial protections. Some of the key challenges remain to be faced, such as the fragmented and inequitable health delivery system, and the increasing demand for high-quality and value-based service delivery. Given that China has committed to achieving UHC and ‘Healthy China 2030’, the evidence from this study can be suggestive of furthering on in the UHC journey and taking the policy steps necessary to secure change.
References
Footnotes
Handling editor Seye Abimbola
WT and ZZ contributed equally.
Contributors WT and ZZ wrote the first draft of the manuscript, did the literature search and review, collected and analysed the data, produced the tables and figures, and interpreted the results. HD contributed to analysis formulation. PL assisted with data collection. LC was involved in editing each draft. DY, JW and RZ provided comments and suggestions in revisions of the analysis. WL designed the study and set the research direction. GK critically revised the analysis and provided overall guidance. All authors approved the final submitted version.
Funding This work was supported by the National Natural Science Foundation of China (grant no 71874115) and China Scholarship Council (CSC no 201806240304).
Disclaimer The funders had no role in the study design, data collection, data analysis, data interpretation and in writing the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.