Article Text

Abstract
Introduction Access to maternal and newborn healthcare has improved in Myanmar. However, regular contact with skilled care providers does not necessarily result in quality care. We assessed adequate contact made by women and newborns with skilled care providers, reception of high-quality care and quality-adjusted contacts during antenatal care (ANC), peripartum care (PPC) and postnatal care (PNC) in Myanmar.
Methods This cross-sectional study was conducted in a predominantly urban township of Yangon and a predominantly rural township of Ayeyawady in March 2016. We collected data from 1500 women. We measured quality-adjusted contact, which refers to adequate contact with high-quality care, as follows: ≥4 ANC contacts and receiving 11–14 of 14 intervention items; facility-based delivery assisted by skilled care providers, receiving 7 of 7 PPC intervention items; and receiving the first PNC contact ≤24 hours postpartum and ≥2 additional contacts, and receiving 16–17 of 17 intervention items. Using multilevel logistic regression analysis with a random intercept at cluster level, we identified factors associated with adequate contact and high-quality ANC, PPC and PNC.
Results The percentage of crude adequate contact was 60.9% for ANC, 61.3% for PPC and 11.5% for PNC. However, the percentage of quality-adjusted contact was 14.6% for ANC, 15.2% for PPC and 3.6% for PNC. Adequate contact was associated with receiving high-quality care at ANC, PPC and PNC. Being a teenager, low educational level, multiparity and low level in the household wealth index were negatively associated with adequate contact with healthcare providers for ANC and PPC. Receiving a maternal and child health handbook was positively associated with adequate contact for ANC and PPC, and with receiving high-quality ANC, PPC and PNC.
Conclusion Women and newborns do not receive quality care during contact with skilled care providers in Myanmar. Continuity and quality of maternal and newborn care programmes must be improved.
- child health
- maternal health
- quality of care
- effective coverage
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Although access to healthcare services has improved, women and their newborns need to make contact with healthcare providers and receive high-quality care throughout their pregnancy, delivery and in the postpartum phase.
What are the new findings?
Nearly 60% of women and their newborns had adequate contact with healthcare providers during pregnancy and delivery, yet only 15% received high-quality care during these encounters.
Regular contact with healthcare providers and quality care are considerably challenging in the postpartum period: less than 12% of women and their newborns made postnatal contact with healthcare providers three times, during which 3% received high-quality care.
What do the new findings imply?
Maternal and newborn health programmes should make further efforts to fill the gap between crude contact and quality-adjusted contact with healthcare providers, particularly for postnatal care.
A standard quality of care measurement that corresponds to the national guidelines is necessary for monitoring the progress of the maternal and newborn health programme.
Introduction
Maternal and newborn health has dramatically improved during the Millennium Development Goals era. However, the majority of countries have not reached the target of 75% reduction in maternal mortality.1 2 Continuity of care is an important approach to improving maternal, newborn and child health outcomes.3 4 However, continuity of care continues to be a critical challenge in resource-limited settings. In 2009 - 2014, nearly 90% of women received antenatal care (ANC) at least once, but only 55% received ANC at least four times. Additionally, a skilled care provider supervised 65% of the women during delivery, and 58% of women and 28% of newborns received postnatal care (PNC) in 75 priority countries.5 Moreover, in 2010 - 2013, 25% of women in three South Asian countries and 14% of women in six sub-Saharan African countries received a series of care including four ANC contacts, delivery assisted by skilled care providers and PNC within 24 hours postpartum.6
The regular access of women and newborns to healthcare and healthcare providers does not reflect the quality of care they are offered. Poor quality of care does not contribute to a healthy pregnancy and safe childbirth. Previous studies have measured the content of care or effective care coverage as representations of the quality of care,7–12 because there was no standard measurement of quality of care for maternal and newborn healthcare until the WHO developed its ‘Standards for improving quality of maternal and newborn care in health facilities’ in 2016.13 14 Previous studies have shown that high-quality antenatal and obstetric care is associated with a decrease in maternal and neonatal complications,15 stillbirths16 and neonatal mortality.17 18 However, prior quality studies and effective coverage analyses demonstrated gaps in care.19–21 Women and newborns are continuously at risk of developing complications in the postpartum period.22 23 According to our literature review, little evidence is available on the frequency of contact and quality of PNC, compared with ANC and delivery care.
The Republic of the Union of Myanmar (Myanmar) is located in South East Asia, and had an estimated population of 51.5 million in 2014.24 In 2015, the country was classified as a lower-middle-income country by the World Bank.25 The maternal mortality ratio declined to 200 deaths per 100 000 live births in 2013.26 Neonatal mortality had also declined to 25 deaths per 1000 live births by 2015.27 However, these statistics are still too high based on the Sustainable Development Goals targets. This may be due to lack of resources and capacity in healthcare facilities, and poor utilisation of routine maternal and newborn healthcare. The maternal and newborn health programme is funded by the government with the support of various development partners.28 Myanmar’s Demographic and Health Survey 2015–2016 found that 58.6% of women had at least four ANC contacts, 60.2% delivered with the assistance of skilled care providers, and 71.2% had a postnatal check-up within 2 days postpartum.27 While quality of care along with continuity is essential for improving maternal and newborn health, little evidence is available on the quality of care during regular contact with healthcare providers for ANC, peripartum care (PPC) and PNC in Myanmar.
We aimed to assess the contact of women and their newborns with healthcare providers, quality of care and quality-adjusted contacts during ANC, delivery and PNC, and to identify factors associated with having adequate contact and receiving high-quality care in Myanmar.
Methods
Study setting
We conducted a cross-sectional study in Myanmar in March 2016. We selected the Yangon and Ayeyawady regions as study sites to enhance the generalisability of the study. Yangon is the most urbanised region in Myanmar and has the highest population in the country. In 2014, Yangon had an estimated population of 7.4 million people and a density of 716 people per square kilometre, whereas the Ayeyawady region had an estimated population of 6.2 million and a density of 177 people per square kilometre.24 We selected only one township from each region to make the target population numbers for each region comparable. Out of the 46 townships in the Yangon region,29 we selected Shwe Pyi Tha township, which is a predominantly urban site. Out of the 33 townships in the Ayeyawady region,30 we selected Pan Ta Naw township, which is a predominantly rural site. Health systems within townships generally comprised public healthcare facilities including a township hospital, station hospitals, rural health centres, subrural health centres, and community-based activities by community health workers and volunteers. Shwe Pyi Tha township had a township hospital, no station hospital, two rural health centres and eight subrural health centres. Pan Ta Naw township had a township hospital, four station hospitals, nine rural health centres and fifty subrural health centres. Public healthcare facilities provided free services. A growing number of private facilities are being operated in urban areas like Yangon.
Sample selection
We recruited women who were between 6 weeks and 12 months postpartum at the time of the survey. We did not include women who had an abortion during that period. We identified a target population of 1456 in Pan Ta Naw township and 1958 in Shwe Pyi Tha township. The sample size of the study comprised 1500 women, which accounted for about half of the target population in the two sites. We recruited 750 women from each site because the two sites had an almost similar-sized target population. At the first stage, we adopted the administrative unit named ‘ward’ or ‘village tract’ as a cluster, and selected clusters to cover about half of the target population. The Yangon site was composed of 27 clusters, including 23 wards and 4 village tracts, and we randomly selected 14 clusters: 12 wards and 2 village tracts. The Ayeyawady site had 56 clusters, including 4 wards and 52 village tracts. We randomly selected 21 clusters comprising 2 wards and 19 village tracts. At the second stage, we determined the sample size for each cluster by calculating the proportion of the target population within a cluster to the total target population within the township using a birth registration list. Although we attempted to select eligible women randomly, we switched to convenience sampling on the first day of on-site recruitment due to logistical constraints (incorrect address of women’s household, women’s absence from home or migration). To mitigate potential selection bias, we announced the date and venue of the survey to women in advance with the support of healthcare providers, the local authority and community volunteers, and conducted interviews at local public places such as monasteries, community centres and at women’ homes.
Data collection
We developed a survey questionnaire based on the Myanmar government’s ‘Five-year strategic plan for reproductive health 2014–2018’,28 ‘Maternal and Child Health Handbook (MCH Handbook)’,31 and the WHO’s ‘Pregnancy, childbirth, postpartum and newborn care: a guide for essential practice’.32 The 30 research assistants administered face-to-face interviews among eligible women and collected data on their basic characteristics, the frequency of their contact with healthcare providers, and the content of the ANC, PPC and PNC they received. Assistants collected data that women recalled regarding the frequency of their contact with healthcare providers and the content of the care they received. They also used the MCH Handbook as a reference whenever it was available during the interviews. Data on these women’s basic characteristics included age, ethnicity, educational level, marital status, household wealth, regular household income, parity, timing of the first ANC attendance, alcohol consumption, tobacco smoking and betel chewing during pregnancy, type of health facility used, whether they received an MCH Handbook, child’s age, and experience of complication during pregnancy, delivery and postpartum period. The household wealth variable was generated by conducting a principal component analysis with 13 items of household assets and infrastructure (radio, television, computer, mobile phone, refrigerator, bicycle, motorbike, car, washing machine, gas/electric cooker, household piped water, private toilet and electricity), ranking the scores in descending order and categorising the household wealth index into 0–20, 21–80 and 81–100 centiles: high, middle and low levels. Data on complications were collected from a list of common complications during pregnancy, delivery and postpartum, and were converted to a binary variable representing any complications experienced at each phase.
Study outcomes
The study outcomes were the frequency of women and their newborns’ contact with healthcare providers and the quality of care during this contact. We defined quality-adjusted contact as having adequate contact and receiving high-quality care (online supplementary table 1).
Supplemental material
Adequate contact for ANC, PPC and PNC was defined as follows: at least four contacts for ANC; delivery at a healthcare facility with the assistance of skilled care providers; and at least three contacts for PNC, with the first contact being within 24 hours postpartum. Although the national guidelines recommend four PNC contacts, this was not introduced in the MCH Handbook at the time of the survey. Thus, we considered at least three contacts for PNC as adequate contact.
Quality of care was measured based on the content of care that women and their newborns received during their contact with healthcare providers. This measurement of quality focuses on the domain of competent care defined in the high-quality health system framework proposed by Kruk et al.33 We selected 14 intervention items for ANC, 7 intervention items for PPC and 17 intervention items for PNC (12 maternal intervention and 5 newborn intervention items). These items were routine interventions recommended in the MCH Handbook31 and the WHO’s guidelines.32 Since previous studies measured quality of care using an index of service provision and regarded the top 20–25 percentile of the scores as high-quality care,8 18 19 we ranked the study sample by the total number of interventions received by a woman and her newborn at each phase, and determined the top 20 percentile as having received high-quality care: ≥11 items in ANC, 7 items in PPC and ≥16 items in PNC.
Analysis
Descriptive analyses included distributions of sociodemographic characteristics of women. We used χ2 test without controlling for the clustered nature of the data to compare the coverage of routine interventions for ANC, PPC and PNC between women who had adequate and no/inadequate contact. We calculated the proportions of adequate contact, receipt of high-quality care and quality-adjusted contact at ANC, PPC PNC, and all three phases accordingly.
Finally, we performed a multilevel logistic regression with a random intercept at sampling cluster level to identify factors associated with the two study outcomes: having adequate contact and receiving high quality of care for ANC, PPC and PNC accordingly. We included adequacy of contact, age, educational level, parity, household wealth, whether women received an MCH Handbook, child’s age, experience of complication and study site as independent variables based on our field observations and previous research.34 The variable of health facility type was not included in the model because the analysis involving this variable automatically excludes women who had no contact for ANC and PNC. The characteristics of the healthcare facility could affect the quality of care. However, this information was not available in this study. Therefore, we assumed that the variance of study outcomes attributed to the sampling cluster (residential area) partially included unmeasured factors related to healthcare facilities within the cluster. We calculated intraclass correlation coefficient (ICC) to estimate the proportion of variance in the study outcome explained by the cluster factor (ie, random intercept). We tested two models for each outcome: the null model, which does not include any independent variables; and the full model, which includes a set of independent variables. Missing data were excluded from the analysis. We analysed data using Stata V.13.
Results
We analysed 1500 women (table 1). Women in Yangon were more likely to be Burmese (86.7% vs 56.3%), have high school or higher education (24.1% vs 12.8%), be wealthy (32.8% vs 5.6%) and have a regular household income (66.4% vs 60.3%) compared with women in Ayeyawady. Meanwhile, women in Ayeyawady were more likely to receive the first ANC within 16 weeks compared with women in Yangon (44.1% vs 18.9%). During pregnancy, 1.5% of women consumed alcohol, 2.1% smoked tobacco, 15.0% chewed betel and 34.7% of women had family members who smoked tobacco. Over 65% of women received ANC at a health centre in Ayeyawady and nearly 40% of women in Yangon received ANC at a hospital. Women in Yangon were more likely to give birth at a hospital (58.0%) compared with women in Ayeyawady (45.7%). Women in both Yangon (52.4%) and Ayeyawady (44.3%) received PNC at a hospital.
Basic characteristics of participating women
The coverage of routine interventions was significantly higher among women who had adequate contact apart from checking on history of domestic violence during ANC, immediate drying of a newborn’s body, delayed first bathing of newborns and skin-to-skin contact at PPC when all study samples were considered (table 2). On excluding women who had no contact with healthcare providers for ANC and PNC, most of intervention coverage was still higher among those who had adequate contact with healthcare providers for interventions other than for deworming medication and checking on history of domestic violence during ANC, and blood pressure and anaemia checks during PNC. Regarding newborns interventions during PNC, however, no difference was observed in the intervention coverage between those who had adequate and inadequate contact if newborns had at least one postnatal contact.
Content of antenatal, peripartum and postnatal care received by women and newborns
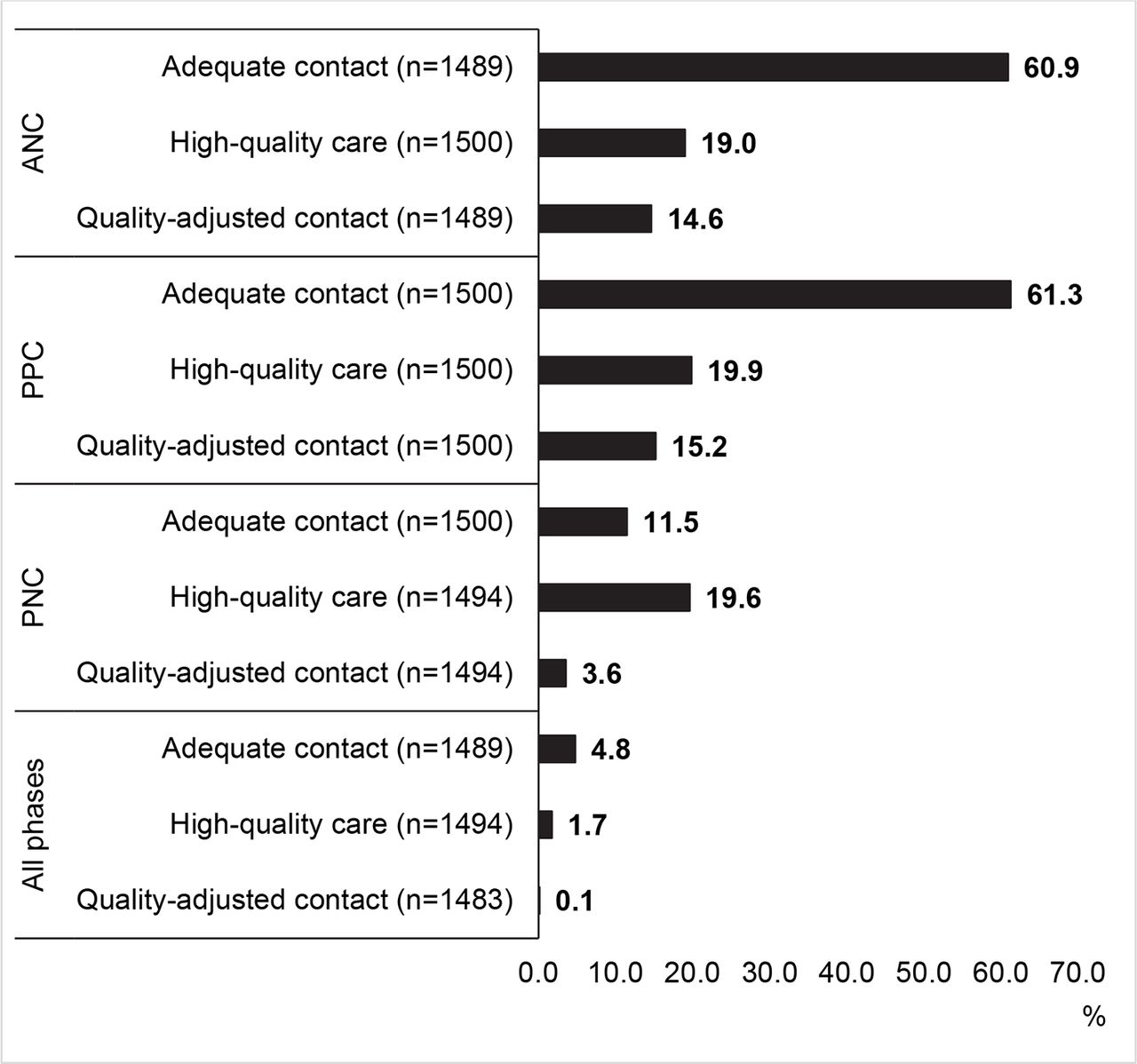
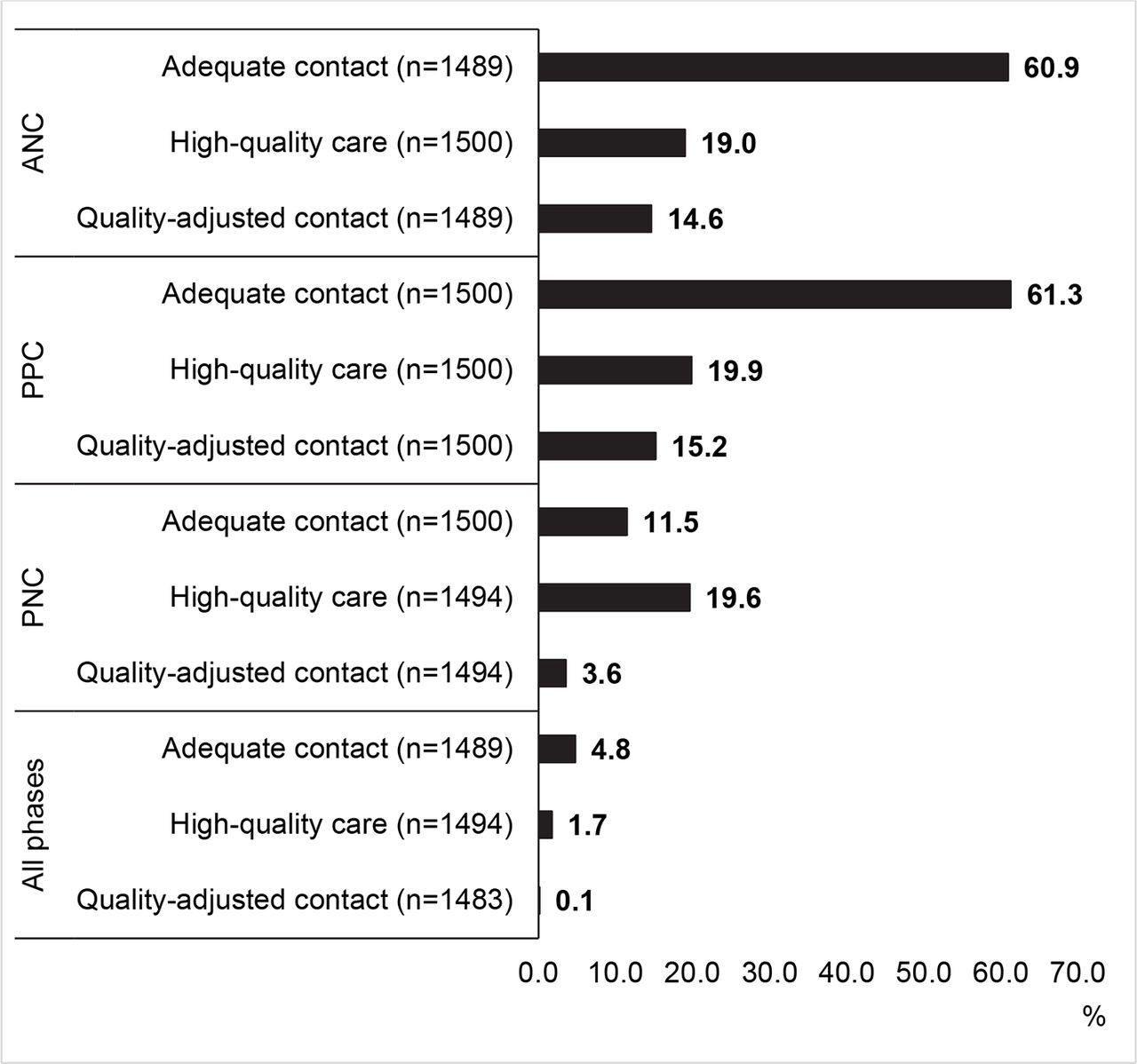
Figure 1 shows the distributions of adequate contact, high-quality care and quality-adjusted contact for ANC, PPC and PNC. During pregnancy, nearly 60% of women had adequate contact, but less than 15% had quality-adjusted contact. Similarly, in PPC, 61% of women delivered with the assistance of skilled care providers at a healthcare facility, and only 15% received high-quality care during contact with healthcare providers. In the postpartum period, 11% of pairs of women and newborns had adequate contact for PNC and only 3.6% had quality-adjusted contact. Consequently, 4.8% of pairs of women and newborns had adequate contact, 1.7% received high-quality care and only 0.1% had quality-adjusted contact across all three phases of maternal and newborn care.
{kind=link}
Proportion of adequate contacts, high-quality care and quality-adjusted contacts during antenatal care (ANC), peripartum care (PPC) and postnatal care (PNC), and across all three phases. Quality-adjusted contacts refer to adequate contact with the reception of high-quality care. All phases refer to a series of the three phases including ANC, PPC and PNC.
Tables 3–5 show the associations of women’s characteristics with the two study outcomes (adequate contact and receiving high-quality care) during ANC, PPC and PNC, using multilevel logistic regression. Unadjusted ORs are shown in online supplementary tables 2, 3 and 4 . Overall, women who had adequate contact were more likely to receive high-quality care at each phase compared with their counterparts.
Associations of having adequate contact and receiving high-quality care with basic characteristics during ANC
Associations of having adequate contact and receiving high-quality care with basic characteristics during PPC
Associations of having adequate contact and receiving high-quality care with basic characteristics during PNC
During pregnancy, two factors were positively associated with adequate contact for ANC. One was having middle or high school education and the other was receiving an MCH Handbook. In contrast, three factors were negatively associated with adequate contact: being a teenager, multiparity, and middle or low level in the household wealth index (table 3).
Factors that were not associated with adequate contact for ANC were the child’s age, experience of complications during pregnancy and the study site.
Reception of an MCH Handbook was associated with high-quality care in ANC, and experience of complications during pregnancy was associated with low-quality care. Women’s age, educational level, parity, household wealth, child’s age and study site were not associated with high-quality care in ANC.
During delivery, five factors were associated with skilled facility-based delivery: women’s age of ≥35 years, having middle or high school education, receiving an MCH Handbook, experience of complications during pregnancy and living in Yangon (table 4). Meanwhile, three factors associated with non-skilled facility-based delivery were being a teenager, multiparity, and middle or low statuses in the household wealth index. The child’s age and experience of complications during delivery were not associated with skilled facility-based delivery.
Reception of an MCH Handbook was associated with high-quality care in PPC. Women’s age, educational level, parity, household wealth, child’s age, experience of complications during pregnancy and delivery, and study site were not associated with high-quality care in PPC.
During the postpartum period, high school education was positively associated with adequate contact for PNC, whereas living in Yangon was negatively associated with adequate contact (table 5). Women’s age, parity, household wealth, reception of an MCH Handbook, child’s age and experience of complications during delivery and postpartum periods were not associated with adequate contact for PNC.
Receiving an MCH Handbook was associated with high-quality care in PNC, while living in Yangon was associated with low-quality care. Women’s age, educational level, parity, household wealth, child’s age and experience of complications during delivery and postpartum period were not associated with high-quality care in PNC.
Tables 3–5 also present the ICCs of a random intercept to examine variations in the study outcome variables explained by differences in residential areas. Conditional ICCs of adequate contact were higher compared with those of receiving high-quality care at each phase. The full model of ANC shows that 13.4% (conditional ICC=0.134) of the variance in adequate contact and 8.5% of the variance in high-quality care can be explained by residential areas, after controlling for individual characteristics measured in this study. In the same way, the full model of PPC shows that 7.6% of the variance in adequate contact and 5.3% of the variance in high-quality care can be explained by residential areas. The full model of PNC shows that 7.7% of the variance in adequate contact and 5.0% of the variance in high-quality care can be explained by residential areas. The median ORs in the full models were 1.98 for adequate ANC contact, 1.69 for high-quality ANC, 1.64 for adequate PPC contact, 1.51 for high-quality PPC, 1.65 for adequate PNC contact and 1.49 for high-quality PNC.
Discussion
The gap between crude contact and quality-adjusted contact was an important finding in this study. This indicates that, even though women and newborns had adequate contact with healthcare providers through improved access to care, the majority of them did not receive high-quality care. Age, educational level, household wealth, parity, reception of an MCH Handbook, experiencing complications and study site were associated with having adequate contact and receiving high-quality care. Variations observed in the frequency of contact and quality of care were influenced by the residential cluster effect.
Women’s characteristics including being a teenager, low levels of school education and household wealth index, and multiparity were associated with inadequate contact, but not necessarily with receiving high-quality care for ANC and PPC. This implies that women’s socioeconomic backgrounds affected the odds of access to routine contact with healthcare providers, and that non-individual factors, such as the health system or community, might affect the odds of receiving high-quality care. The associations of the MCH Handbook and study site with high-quality care observed in this study might reflect this proposition. A previous study found that women with higher socioeconomic statuses were more likely to access healthcare because of their financial capacity to assume direct and indirect costs of healthcare.34 As a result, socioeconomic disparity has been a critical challenge in the improvement of maternal and newborn health services in low-income and middle-income countries.35 Although the rapid economic growth in Myanmar may accelerate the development of the country’s health system, it may also create a disparity in access and utilisation of primary healthcare among people with different socioeconomic statuses.
Women who received an MCH Handbook were more likely to have ≥4 ANC contacts with healthcare providers, deliver at a healthcare facility with the assistance of skilled care providers, and receive high-quality ANC, PPC and PNC. Similarly, in other Asian settings, women who received a home-based record including the MCH Handbook had adequate ANC visits, delivery with the assistance of skilled healthcare providers, and practised newborn feeding and care properly.36–38 Although women must access a healthcare facility at least once to obtain the Handbook, the Handbook may effectively facilitate women to access healthcare continuously and increase their chances of receiving essential care. It could also help healthcare providers offer routine interventions and pay attention to women and newborns with special care needs. The maternal and newborn care programme in Myanmar should prioritise full coverage of the Handbook as a policy agenda.
Women who experienced complications during pregnancy were less likely to receive high-quality care at ANC, but they were more likely to deliver at a healthcare facility with skilled assistance. A similar finding was reported by a study conducted in Tanzania.39 Although the cross-sectional design used in this study does not explain the sequence between the two findings, women’s experience of complications and reception of interventions to treat these complications might subsequently change their care-seeking behaviour. To identify and treat complications early, healthcare providers should educate new mothers about danger signs during ANC, offer optimal interventions for complications and follow up to ensure safe delivery.
Women in Yangon were more likely to give birth at a healthcare facility with skilled assistance but not have postnatal contact and receive high-quality care, compared with women in Ayeyawady. This indicates that women in Yangon did not necessarily seek PNC after delivery at a healthcare facility. Poor utilisation of PNC by women after giving birth at healthcare facilities was also observed in Tanzania.40 Lack of knowledge and perceptions regarding the necessity of PNC visits were major reasons for not seeking PNC in China.41 Another potential reason was that, despite the relatively greater number of better equipped facilities and variety of health and social services available in urban areas, urban population growth commonly takes place in low-income communities, where inadequate healthcare is provided to people living in these communities.42 Shwe Pyi Tha township is an urban industrial area with several migrants from rural regions; the study finding may imply an urban poverty issue. Another potential reason is that women in Ayeyawady were relatively more likely to seek PNC because they were more likely to give birth at home and would need to receive the first PNC check-up and a birth certificate at a healthcare facility. Further indepth research is needed to assess site-specific reasons for low coverage and quality of PNC at individual and community levels.
Variations in achieving adequate contact and receiving high-quality care were partially explained by cluster effects according to the random intercepts of multilevel analysis. The cluster effect was greater for adequate contact, compared with high-quality care during ANC and PPC, potentially due to the higher prevalence of the adequate contact compared with high-quality care observed in this study.43 Other studies also reported that variations in the use of maternal newborn care40 44 and newborn survival45 can be explained by community-level effects. Further studies should explore the characteristics of healthcare facilities or communities that are associated with women’s contact with healthcare providers and reception of high-quality care.
This study assessed the coverage of various routine interventions, during which a low percentage of women had their emotional status and history of domestic violence checked. Moreover, about 35% of women had family members who smoked tobacco during their pregnancy. Mental disorder,46 domestic violence47 and secondhand smoke48 are priority issues affecting women’s health and that could also affect their newborns’ health. Access to care continues to be a challenge for many women living in low-income and middle-income countries. Therefore, addressing these health issues in maternal and newborn health programmes could greatly benefit those in need.49 50 Further, pregnancy and childbirth are major family events, and they may serve as an opportunity to improve health behaviours and address psychosocial health issues among family members.
Limitations
This study has several limitations. First, random sampling was compromised at the individual level: the study samples were potentially biased, which could affect the study results. To mitigate the potential effect of selection bias, we disseminated the survey information in advance with the help of midwives and health volunteers in order to reach all eligible women, and we collected the data at various public places. Further, we compared the distributions of educational level, ANC contact, facility delivery and PNC contact between the present study and the recent population-based surveys27 29 30 in online supplementary table 5. Second, the vague memory and limited health literacy of participating women might affect the quality of the data. However, previous research has found that women can recall the care items they receive,51 and Myanmar Demographic and Health Survey 2015–2016 used data from women’s recollection of the antenatal, delivery and postnatal care they received more than 2 years before the survey.27 Third, we assessed only one aspect of quality of care. Future studies should be conducted to measure multifaceted dimensions of quality of care such as safety, timeliness, client experience, client and healthcare provider interaction, and health impact.13 Fourth, lack of information about facility characteristics limited our ability to assess the associations of supply-related factors with the study outcomes. Although we performed a multilevel analysis to consider cluster effects of the study outcomes, further analysis will be beneficial if we include facility or community characteristics. Finally, the cross-sectional design and the limited geographical representation may limit the generalisation of the study findings. Myanmar is composed of 15 regions/states with various characteristics, and it has been experiencing rapid economic growth. Monitoring the effects of the socioeconomic transition on access and quality of care and outcomes in maternal and newborn health across the country would be beneficial.
Conclusions
Women and newborns who had adequate contact with healthcare providers did not necessarily receive quality care. Mitigating disparities in individual socioeconomic status and health system development will be instrumental in improving the continuity and quality of maternal and newborn care in Myanmar.
Acknowledgments
The authors are thankful to the study participants and research assistants for supporting the study. Particularly, we thank Ms. Thu Nandar Saw, Dr. Yu Mon Saw, Dr. Khine Thet Su, Dr. Su Sandy, and Ms. Kanan Nakamura for their technical support during data collection. We also thank Associate Professor Margaret E. Kruk, Professor Ana Langer, Lecturer Jesse B. Bump and Professor Michael Reich at the Harvard T. H. Chan School of Public Health for their technical support, as well as the Takemi Program in International Health at the Harvard T. H. Chan School of Public Health and the Japan Medical Association for their support.
References
Footnotes
Handling editor Sanni Yaya
Contributors SO, HHW, KN and MJ conceived and designed the study. AS and PPA provided critical advice on the design. SO and HHW collected the data. SO analysed the data. SO wrote the first draft of the manuscript. HHL and MJ contributed to data interpretation and critically edited the manuscript. MJ obtained funding. MJ and HHW supervised the study. All authors read and approved the final manuscript.
Funding This research was supported by the Japan Agency for Medical Research and Development (AMED).
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval We obtained ethical approval from the University of Medicine I, Yangon, Myanmar Ministry of Health and Sports, Department of Medical Research, and The University of Tokyo. We also obtained written consent from all participants before interviewing them.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are not publicly available because they contain information that could compromise the confidentiality or consent of the study participants.