Article Text

Abstract
Background Delivery attended by skilled professionals is essential to reducing maternal mortality. Although the facility delivery rate in Ethiopia's rural areas is extremely low, little is known about which health system characteristics most influence women's preferences for delivery services. In this study, women's preferences for attributes of health facilities for delivery in rural Ethiopia were investigated.
Methods A population-based discrete choice experiment (DCE) was fielded in Gilgel Gibe, in southwest Ethiopia, among women with a delivery in the past 5 years. Women were asked to select a hypothetical health facility for future delivery from two facilities on a picture card. A hierarchical Bayesian procedure was used to estimate utilities associated with facility attributes: distance, type of provider, provider attitude, drugs and medical equipment, transport and cost.
Results 1006 women completed 8045 DCE choice tasks. Among them, 93.8% had delivered their last child at home. The attributes with the greatest influence on the overall utility of a health facility for delivery were availability of drugs and equipment (mean β=3.9, p<0.01), seeing a doctor versus a health extension worker (mean β=2.1, p<0.01) and a receptive provider attitude (mean β=1.4, p<0.01).
Conclusion Women in rural southwest Ethiopia who have limited personal experience with facility delivery nonetheless value health facility attributes that indicate high technical quality: availability of drugs and equipment and physician providers. Well-designed policy experiments that measure the contribution of quality improvements to facility delivery rates in Ethiopia and other countries with low health service utilisation and high maternal mortality may inform national efforts to reduce maternal mortality.
- Maternal mortality
- facility utilisation
- facility delivery
- stated preference
- discrete choice experiment
- decision-making PR
- developing country CG
- health services research
- maternal DI
Statistics from Altmetric.com
- Maternal mortality
- facility utilisation
- facility delivery
- stated preference
- discrete choice experiment
- decision-making PR
- developing country CG
- health services research
- maternal DI
Introduction
The maternal mortality ratio, an indicator of progress on Millennium Development Goal 5 to improve maternal health, is a measure of obstetric risk associated with each live birth. While maternal death is exceedingly rare in developed countries, high rates of death have persisted in poor countries with the result that the global maternal mortality ratio has remained relatively constant over the past several decades.1 Developing countries that have managed to reduce maternal mortality, such as Malaysia and Sri Lanka, have done so through high-level, sustained political commitment to the survival of mothers, by professionalising delivery care and by improving health system infrastructure to respond to obstetric complications.2–4
Ethiopia, a country with a widely dispersed and largely rural population of approximately 77 million people, has 1806 physicians, 18 146 nurses, 143 hospitals and 690 health centres.5 By comparison, France, with a population of 61 million, has 207 000 physicians and 486 000 nurses.6 Most physicians and nurses in Ethiopia practice in Addis Ababa and other urban areas. To address this human resource crisis, the Ethiopian government has trained 30 000 health extension workers to provide health education and preventive services at rural health posts, and is increasing the training of physicians and other health personnel. It has also expanded its network of first-level health posts from 1311 in 2001 to 11 446 in 2007.7 While some health posts are equipped to provide delivery services, the government has designated health centres and hospitals for the provision of obstetric services. Of those, only hospitals can provide comprehensive emergency obstetric care, including caesarean section and blood transfusion. Health centres can handle some non-surgical obstetric complications and refer others to hospitals. Health centres and hospitals experience frequent shortages of staff, medicines and equipment.
Ethiopia's maternal mortality ratio of 673 per 100 000 live births, however, remains among the highest in the world and has fallen little if at all since 2001.8 Maternal mortality in Ethiopia is likely linked to extremely low utilisation of skilled birth attendants and facility delivery and to even lower use of emergency obstetric care. The 2005 Demographic and Health Survey found that only 25% of all Ethiopian mothers living in rural areas received any antenatal care from a health professional in their last pregnancy, 3% delivered in a health facility and 0.3% delivered by caesarean section.8 Women in rural areas have limited access to facilities and low social status.8 For example, one-third of women in Ethiopia report that their husbands make decisions about their healthcare without consulting them, while only 15% of women make their own decision.8
While there is a growing body of literature about community-level, cultural and socioeconomic factors that may promote or impede facility delivery in sub-Saharan Africa,9–12 there is less research on health service characteristics that promote utilisation, with the exception of research on user fees, which have been shown to reduce utilisation.13–16 However, facility delivery rates, cultural factors and health system characteristics vary widely among countries in Africa, and there are no recent studies on determinants of maternal health service utilisation in Ethiopia—a country that will not meet the maternal health Millennium Development Goal at current rates of progress.
In this article, we explore health system factors that are important to women in selecting a facility for delivery in rural southwest Ethiopia using a discrete choice experiment (DCE). Promoting delivery in health facilities is a core strategy to reduce maternal mortality in Ethiopia.17 DCEs are an increasingly used technique to elicit preferences for health and healthcare. The main assumptions behind DCEs are that any good or service can be described in terms of a set of characteristics and that its valuation depends on the levels of these characteristics.18 If a price for the service is included as an attribute, then willingness to pay (WTP) can be estimated by calculating how much money people are willing to trade off to gain an improvement in another attribute.19 DCEs have been shown to be efficient and have good convergent validity with other utility assessment tools in health economics, such as standard gambit and open-ended preference elicitation.20 They have the advantage of presenting a bundled set of health service attributes to the user, which is a better representation of actual choices than ranking or rating individual attributes.21 22 With the addition of graphic representations of attribute levels, DCEs have also been shown to be viable for use in populations with low literacy.18 23
Methods
Study area and sample
This study took place in the Gilgel Gibe area in Jimma zone, Oromia region, in southwest Ethiopia. This is a predominantly rural area where the primary occupation is subsistence agriculture. The Gilgel Gibe Growth and Development Study (GGGDS) is a longitudinal cohort study of families in the Gilgel Gibe region that is concerned with adult mental health and child development. It has been described elsewhere.24 The baseline sample for the GGGDS consisted of households that had a child between the ages of 3 and 24 months from the population of all births in Gilgel Gibe in the 2 years before the estimated start date of the survey, December 2006. This analysis is about 1006 women, all living in rural areas, who were included in wave 2 of the study; the baseline response rate was 85%, and the follow-up rate was 86%. Data were collected between May and August 2007.
Instrument design and fielding
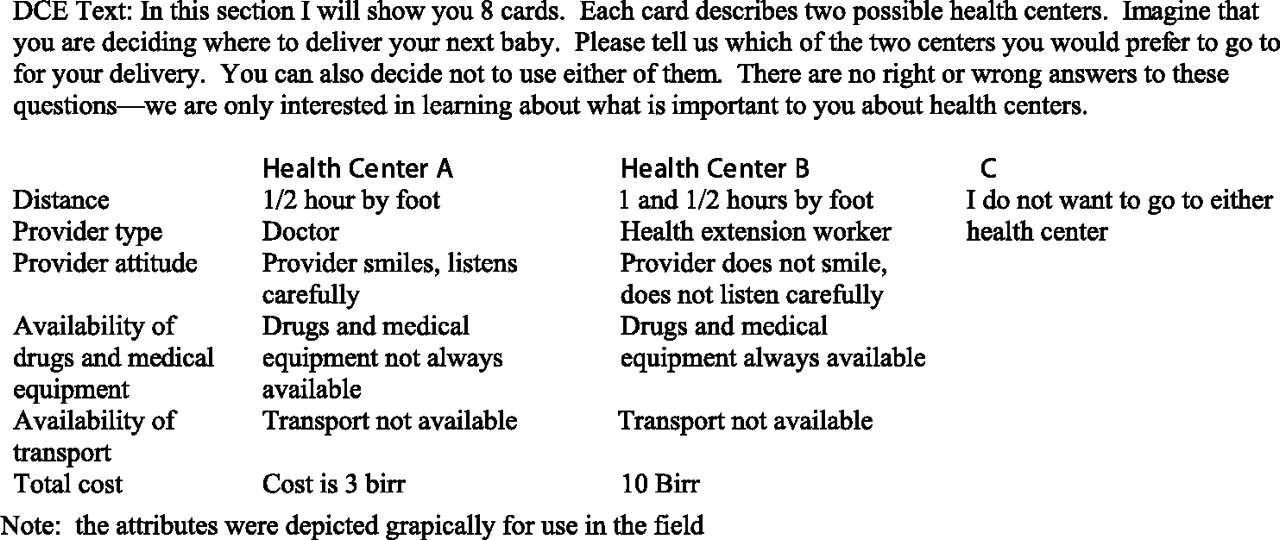
The questionnaire included sections on demographics, child and maternal health and utilisation of healthcare for the most recent delivery, as well as the DCE. The DCE was designed to estimate the relative value or worth of different features (attributes) of health facilities to women in considering where to deliver their next child. The attributes tested were cost, distance, availability of transport, type of provider, provider attitude and availability of drugs and medical equipment. Each woman was shown eight cards, each with two health centres with various combinations of the above characteristics and asked to select either health centre A, health centre B, or neither centre (C). The full range of attributes and levels in the DCE is shown in supplementary appendix A. Each card was also described using a standard script by interviewers in the relevant local language to ensure consistent interpretation (figure 1). For more detail on design and fielding of the DCE, see supplementary appendix B.
{kind=link}
Sample card used in discrete choice experiment, Jimma Zone, Oromia, Ethiopia.
Questionnaires and consent documents were developed in English then translated and back translated into the two dominant languages in the study area, Amharic and Affan Oromifa, by native speakers. Written informed consent was obtained from all participants. The interview was administered face-to-face by trained and experienced interviewers, from Jimma University, who are fluent in Amharic and Affan Oromifa. Each team was headed by a supervisor who observed at least two interviews per day. The responses were recorded by pencil and paper and transferred into a text file, cleaned, and imported into SAS and Sawtooth software. The institutional review boards of University of Michigan and Jimma University reviewed and approved the study protocol.
Statistical analysis
Descriptive univariate statistics were calculated for demographic and place of delivery variables for the study sample using SAS. We also calculated univariate statistics for rural Ethiopian women (DHS 2005) to gauge to the extent to which the GGGDS sample characteristics matched those of rural Ethiopians more generally; this helps us to assess the external validity of our results. The coefficients for the individual utilities of each attribute level were estimated using a hierarchical Bayesian procedure using Sawtooth Software's Choice Based Conjoint/Hierarchical Bayes (CBC/HB) statistical program.25 The model used is hierarchical because it has two levels, the aggregate or group and the individual (statistical detail in supplementary appendix B).
The model output consists of individual-level utility coefficients for attribute levels for each respondent and the average utility estimates for the sample. The ratio of any two coefficients is the marginal rate of substitution between these attributes; this indicates the relative value of one attribute compared to another. To test the predictive validity of the utility estimates for facility choices, we calculated the proportions of women who would be likely to select a specific facility using market simulator software in Sawtooth's CBC/HB module.25 These modelled preferences were then compared with DCE facilities selected by women who were given version 5 (see supplementary appendix B).
To obtain WTP, we calculated the ratio of the coefficients of the non-cost attributes and the coefficient of cost. This reflects the utility gain in moving from the reference level (least desirable level) of an attribute to a more preferred level of an attribute (eg, from not having drugs to having drugs always available).20
Results
Of 1016 interviewed women, 1006 had data for the DCE (99.0%). The characteristics of these respondents are shown in table 1, along with a comparison with national Ethiopian Demographic and Health Survey (DHS) data. The majority of women in our sample who had a pregnancy in the last 5 years did not give birth in a facility (93.8%). This and other characteristics are consistent with the DHS.
Characteristics of a sample of women from Jimma Zone, Oromia, Ethiopia,* and comparison with DHS rural subsample
In the DCE, women selected facility A or B (rather than “neither”) in 7524 of the 8045 completed choice cards (93.5%), suggesting the attributes and levels that comprised the facility choices were acceptable to the women. The predictive validity of the utility estimates, comparing predicted facility preferences with facility preferences expressed by women who were actually shown version 5 of the DCE, was reassuring with correlation coefficients of 0.94 for health centre A and 0.98 for health centre B.
The coefficients of utilities for the attributes are shown in table 2. For four of the attributes—provider type, provider attitude, availability of drugs and equipment and availability of transportation—the coefficients represent the gain (positive coefficients, or loss, negative coefficients) in utility compared to an omitted (dummy) category. In other words, a positive coefficient indicates that a woman would be more likely to prefer a health facility with that specific attribute. While cost is negatively associated with overall utilities, as expected, the association between utility and travel time was positive. Having an attentive provider, drugs and transport is positively associated with overall utilities, as expected.
Results from hierarchical Bayes model for utility of attributes of health facilities for delivery, reported for 1006 women from Jimma Zone, Oromia, Ethiopia
The coefficient size is an indication of the strength of the preference. The drug availability and doctor variables had the highest coefficients at 3.877 (SE 0.074) and 2.104 (SE 0.058), respectively, indicating that the two variables had a greater influence on women's preferences compared to other attributes in the study. All of the attribute-level coefficients were significantly associated with facility choice at α<0.01.
WTP results are shown in table 3. Women were willing to pay 133.2 Birr (95% CI 128.2 to 138.2) for a clinic that always had drugs and medical equipment compared to a clinic that did not. Having a nurse as a provider as opposed to a health extension worker was worth 56.8 Birr (95% CI 53.4 to 60.21).
Willingness to pay for attributes of health facilities, reported for 1006 women from Jimma Zone, Oromia, Ethiopia
Discussion
We found that women in rural Ethiopia strongly preferred health facility attributes indicative of good technical quality—highly trained providers and reliable supply of medicines and functioning equipment—in selecting a delivery facility. Provider attitude that indicated respect for the patient was also important; by way of illustration, the gain in utility derived from respectful treatment was similar to that in seeing a nurse instead of an extension worker. Convenient access (ie, availability of transport) and proximity to facilities were much less important. Indeed, the converse was true: all other factors being equal, women favoured more distant facilities. This seemingly paradoxical finding makes some sense in the local context because in the study area, the highest quality services are approximately one hour away by car; a trip few could afford to make. Higher-quality services truly are farther away. This result suggests that women are drawing upon their own (obstetric and non-obstetric) experiences with local health services, and perhaps those of neighbours and family, when undertaking the DCE exercise. Other studies in sub-Saharan African have found evidence of active social learning about local health facilities.27
These findings suggest that supply-side factors, particularly factors associated with high quality of care, play a central role in determining preferences for facilities that may in turn influence utilisation of delivery services in low-income countries. A study by Collier and colleagues in Ethiopia confirms the importance of quality using a different econometric approach. The authors used data from rural household surveys conducted between 1994 and 1997 as well as data on quality of nearby facilities to estimate influence of quality versus other characteristics, including distance, on healthcare utilisation. Quality measures included some of the attributes in this study, such as the presence of trained nurses and availability of drugs. The study found that across different model specifications, higher quality was associated with greater likelihood of facility use for people with episodic illness, even after controlling for distance, women's education and household wealth.28 Gertler and Hammer similarly note that studies from Kenya, Nigeria, Ghana and the Philippines found that structural quality improvements in health facilities—particularly in availability of medicines—are associated with substantial increases in utilisation.29
Other studies have documented natural experiments that suggest that facility delivery rates can be increased rapidly if service quality is improved. For example, a health reform effort in Peru that increased quality of obstetric services and promoted a human-rights-based approach to patient care raised the proportion of pregnancy complications treated in facilities from 30% to 84% within 4 years.30 Researchers in Egypt who combined facility data with population data found that objectively measured quality of family planning services were significant predictors of intrauterine device use, independent of distance to facility, maternal wealth, education or parity.31
These findings do not suggest that supply-side factors, such as quality or cost of facility care, are the only determinants of maternal health services utilisation. As noted earlier, intra-household decision-making that favours husbands and religious strictures against delivery by male providers, among other factors, almost certainly influence utilisation. Analysis of the 2000 Ethiopia DHS showed that education, and parity, and birth interval were significantly associated with skilled delivery, concluding that sociocultural factors were key determinants.32 It is noteworthy, however, that in analyses adjusting for these and other demand-side factors, women living in Addis Ababa still had 40 times the attended delivery rate of women in rural areas, with 71% reporting professionally assisted delivery compared to 2.2% in rural areas.32 This suggests that the availability of acceptable clinical services (ie, improving supply-side factors) can overcome at least some cultural, demand-side impediments to higher maternal health facility utilisation.
We found that women were willing to pay US$13 for a facility with medicines compared to a facility without and US$7 for a facility with a doctor compared to one with a health extension worker. Several other studies have also found that women are willing to pay a substantial amount for high quality of care in developing countries.33 34 However, these figures need to be interpreted with caution. The figures here appear high in the context of rural Ethiopia given that Ethiopia's Gross National Income per capita in 2007 was US$220 and that health spending was only US$7 per capita.6 35 These estimates also seem high compared to charges at local hospitals in Jimma, where a labouring woman pays a deposit of approximately US$5 and a regular patient US$10 for admission. Although admitted patients face other costs (eg, transportation, medicines, etc), the hospital charges suggest that a WTP of US$13 for a clinic with reliable medicines may be a high estimate. Other research has pointed out that WTP estimates in DCEs may overstate WTP derived using other valuation methods, and it seems likely that the WTP results here are biased upwards.20 36 As such, WTP results should be interpreted as relative—that is, indicative of the strength of women's relative preferences among the options presented—rather than absolute measures.
The findings need to be interpreted in light of several other limitations. As with some classical approaches to discrete choice modelling, Bayesian methods do not permit inclusion of respondent-specific attributes (as compared to alternative-specific attributes) and thus we cannot compare the strength of demand-side and supply-side determinants. For example, women may have had a neonatal death or other poor outcome that may have influenced their perception of health facilities. While our aim here was to understand health system factors that were important to women rather than to explain utilisation of health facilities for delivery, future research should attempt to quantify the relative contributions of respondent-specific and alternative-specific factors by analysing subsamples or by using more flexible modelling strategies such as mixed effects logit. Future work might also adopt an anthropological approach to populating the DCE variables. Although local health workers were consulted regarding important facility characteristics, it would be interesting to carry out focus groups with women (and men) in these communities to ensure that the attributes selected for the DCE are salient to potential users. Such an exercise might reveal more nuanced and locally specific variables.
By focusing on features of health services that are preferred by potential users, this study aims to contribute to the growing field of health systems implementation research. The results of this study strongly suggest that greater professionalisation of delivery attendants and well-equipped facilities, along with community education to inform women of these reforms, are essential to encouraging women to deliver in health centres. In its third Health Sector Development Plan, the Ethiopian government has laid out three potential scenarios for expanding access to health services ranging from cheapest to more expensive.17 The difference between scenario 1 (costed at US$5.54 per capita) and scenario 2 (costed at US$8.03 per capita) is the construction of more than 1000 additional health centres capable of basic emergency obstetric care and substantial expansion of hospital services along with the requisite addition of skilled personnel. Scenario 3 (US$10.96 per capita) is even more ambitious with extensive clinical service and hospital upgrading.17 The results of our study suggest that scenarios 2 and 3, with their focus on investing in health centres and hospitals, are more likely to lead to higher facility utilisation and, in turn, greater reduction in maternal mortality than scenario 1.
Collier and colleagues arrive at a similar conclusion based on analysis of facility utilisation and measures of density and quality of health centres and posts in rural Ethiopia.28 They estimate that expenditures on improving quality are likely to result in greater facility utilisation than the same expenditures focused on building more facilities and conclude that investments in quality are more cost-effective than investments in density of facilities.28 Given the low current use of facilities, health system improvements would need to be complemented by community-level efforts to encourage women to seek professional care for delivery. Well-designed policy experiments that measure the contribution of quality improvements to facility delivery rates in Ethiopia would provide important insights into maternal mortality reduction efforts there and elsewhere in sub-Saharan Africa.
What is already known on this subject
Ethiopia has a high maternal mortality ratio combined with low utilisation of skilled birth attendants and facility delivery.
While there is some research about demand-side determinants of utilisation, little is known about health system determinants of the decision to deliver in a facility.
What does this study adds
In selecting a hypothetical delivery facility, women in a rural region of Ethiopia placed a high value on well-trained providers and reliable supply of medicines.
This highlights the importance of good technical quality of obstetric services to women in this low healthcare utilisation setting.
Prioritising quality improvements in healthcare reform may increase facility delivery rates.
References
Supplementary materials
Web Only Data jech.2009.087973
Files in this Data Supplement:
Footnotes
Funding This study was supported in part by a grant from the National Institutes of Health (HD047861) and grants from the Robert Wood Johnson Foundation Health and Society Scholars Program.
Competing interests None.
Ethics approval This study was conducted with the approval of the Jimma University IRB and the University of Michigan IRB.
Provenance and peer review Not commissioned; externally peer reviewed.