Article Text

Abstract
Problem Diabetes is a major, growing health problem often managed in primary care but with suboptimal control of risk factors.
Design A large-scale quality improvement collaborative implemented in seven waves.
Setting General practices and Aboriginal medical services across Australia.
Key measures for improvement Percentage of patients in each health service with haemoglobin A1C (HbA1C), total cholesterol and blood pressure at target.
Strategy for change Health services attended three 2-day workshops, separated by 3-month activity periods and followed by 12 months of further improvement work. Local collaborative program managers supported teams to report measures and plan/do/study/act (PDSA) cycles monthly. Health services received feedback about changes in their measures in comparison with their wave.
Effects of change 743 health services participated in seven waves between 2004 and 2009 serving approximately 150 000 people with diabetes. Mean numbers of patients at target HbA1c levels improved by 50% from 25% at baseline to 38% at month 18. Lipid and blood pressure measures showed similar improvement.
Lessons learnt Engagement in the Program and results demonstrated that the collaborative methodology is transferable to Australian primary care. The results may reflect improved data recording and disease coding, and changes in clinical care. Internal evaluation should be built into improvement projects from the start to facilitate improvements and reporting. Enthusing, training and resourcing practice teams appeared to be the key to rapid change. Local support of practice teams was instrumental in improvement. Early investment to facilitate automatic measure collection ensured good data reporting.
- General practice
- quality improvement
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Since 2004 the Australian Primary Care Collaboratives (APCC) Program has implemented quality improvement collaboratives based on the Institute for Health Improvement methodology1 to improve aspects of primary care including diabetes mellitus.
Diabetes mellitus is rising in prevalence around the world2 ,3 and in Australia.4 It is often undiagnosed5 and risk factors are not well controlled.6 It is a major contributor to the health gap of Australian Aboriginal and Torres Strait Islander people who have an average life expectancy 17 years less than non-Indigenous Australians7 and experience an incidence of diabetes four times that of non-Indigenous Australians.8 Good control of glucose, blood pressure, lipids and other risk factors can reduce morbidity and mortality in diabetes.9
There is an extensive literature describing quality improvement strategies in primary care and in diabetes care in particular. Systematic reviews show benefit from educational interventions10 and feedback to clinicians.11 Multifaceted professional interventions and organisational interventions that facilitate structured and regular review of patients improve the process of care. Patient education and enhancing the role of nurses in diabetes care further improve patient outcomes and the process of care.12 Case management, team changes, patient education, care algorithms, and information technology strategies have been shown to have some effect in improving quality of care.13 ,14
Quality improvement collaboratives are multifaceted interventions which bring together many of the strategies identified. They are effective in improving care in targeted topics such as diabetes.15 ,16 They have been used extensively in the USA17 and were adapted and applied in UK primary care. Policymakers in Australia became aware of the impact on chronic disease care of the National Primary Care Collaborative in England. The APCC was created in 2004 as a deliberate strategy to transfer and adapt their work to improve primary care in Australia.
The overall aim for diabetes in the APCC is that 50% of patients with diabetes in participating practices have a haemoglobin A1C (HbA1C) level ≤7%. The APCC also aims to intervene in the Australian primary care sector at multiple levels to achieve cultural change and build capacity in quality improvement and chronic disease care.
Context
Approximately 20 000 general practitioners (GPs) provide care in about 7200 practices in Australia.18 These practices receive support from regional, mainly government-funded, independent organisations called divisions of general practice. A network of Aboriginal medical services focus on the Aboriginal community. The APCC has engaged health services (general practices and Aboriginal medical services) from every state and territory of the Australian continent.
Eighty-three per cent of Australians visit a GP in a year and do so an average of 6.4 times a year.19 GP occasions of diabetes management increased from 2.7 to 4.1 per 100 encounters in the decade to 2008.20
The APCC is administered by Improvement Foundation (Australia) and funded by the Australian government Department of Health and Ageing. It is supported by a central office in Adelaide, South Australia which engages with divisions of general practice across the country. The divisions support local general practices through local collaborative program managers (CPMs).
Key measures for improvement
The key APCC measures for diabetes improvement are:
-
Number of patients on the register.
-
Percentage of patients with diabetes with a last recorded HbA1C ≤7 within the last 12 months.
-
Percentage of patients with diabetes with a last measured total cholesterol of <4 within the last 12 months, or from 2006, low-density lipoprotein cholesterol (LDL-C) <2 mmol/litre.
-
Percentage of patient with diabetes with a last recorded BP reading of <130/80 within the last 12 months until 2006 and then ≤130/80.
Assessment of the problem
Setting the standard
An expert reference panel (ERP) was convened of specialist diabetes experts, primary care clinicians and quality improvement staff. This group determined the aims of the project, the change ideas that would be implemented (table 1) and the improvement measures that would be used.
Australian Primary Care Collaboratives diabetes change principles
Measures
Measures were selected reflecting best evidence while being practical to report in the busy clinical context. The diabetes measures were amenable to extraction electronically from clinical software. Data were de-identified and aggregated at practice level. In early waves they were entered manually in the online reporting system. As software became more sophisticated, measures were automatically uploaded after extraction.
Capacity gaps
Australian general practices, though well computerised in some areas like prescribing and clinical records, were not equipped to collect outcome measures from the clinical record. Concepts like disease registers, disease coding, team care and population management were unfamiliar to many practices. A significant part of the project was capacity building in these areas.
A division of general practice with existing expertise was commissioned to create software that could search clinical record systems to collect outcome measures electronically. Educational experts were involved to design interventions to teach quality improvement.
Acceptability
Medical groups and health services themselves were at times sceptical of improvement projects and work was required by the APCC and the Improvement Foundation to engage them.
Strategies for improvement
Recruitment
Divisions of general practice were invited to recruit a number of health services to the Program. Funding was allocated to the divisions to employ CPMs and to the health services as partial recompense for staff time for workshops and in doing APCC work.
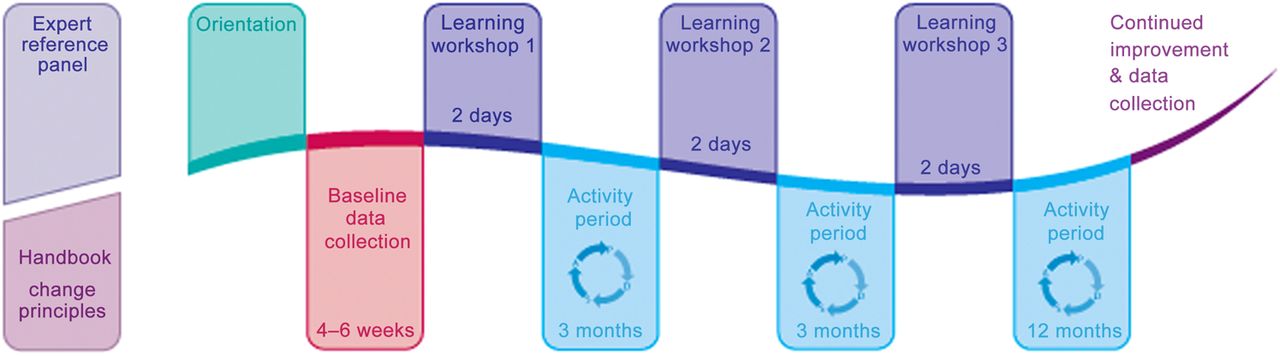
A small team from each health service, usually a doctor and one other, attended a series of workshops. The local teams were supported by a local CPM trained by the APCC. Teams attended an orientation describing the Program. Health services which committed to the collaborative received support to collect baseline improvement measures. In the seven waves they were required to do work in diabetes, coronary heart disease and access.
Learning workshops
Teams attended three learning workshops separated by activity periods of 3 months (figure 1). The 2-day interactive workshops addressed the change principles, the evidence behind them and quality improvement. Spending time together helped participants develop a group identity and generated enthusiasm. Health services that produced good results were used as exemplars in learning workshops two and three. Ideas, successes and failures were shared between health services.

Structure of a collaborative wave.
The model for improvement
Teams were taught improvement methodology using Langley and Nolan's approach.21 They were given experiences in using the three improvement questions and protected time to devise small plan/do/study/act (PDSA) cycles. They were challenged to report at least one PDSA cycle within a week of the first learning workshop.
Activity periods
During activity periods teams used the model for improvement to implement the change principles. They were required to submit improvement measures and PDSA cycle reports monthly. The local CPM reinforced the messages of the learning workshops, advised teams on how to meet challenges, helped with software installation to extract measures and helped with data submission.
Feedback
Health services received monthly feedback on their progress in the improvement measures compared with their wave. CPMs helped health services reflect on their feedback.
Role of the APCC organisation
The central APCC organisation negotiated with the local divisions to recruit and support CPMs and health services. It managed the three large learning workshop events for each wave.
The APCC commissioned software for data extraction. It collected, collated, analysed and returned feedback on changes in wave and health service measures through an online reporting system and negotiated at state and national levels with governments and stakeholders to maximise the chance of success of the Program.
Effects of change
Participation
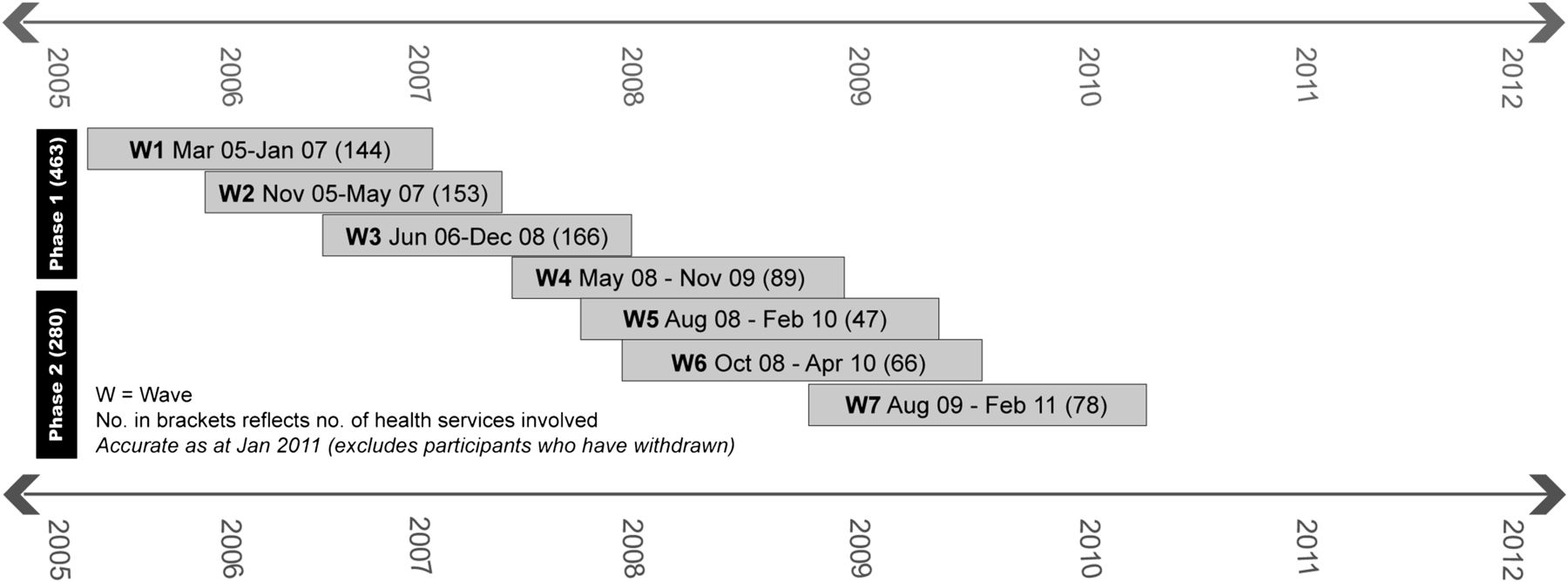
Eight hundred and eleven health services commenced the APCC Program. Sixty-eight withdrew leaving 743 health services completing the required 18 months. The Program was implemented in seven ‘waves’ of new practices between 2004 and 2009 (see figure 2).
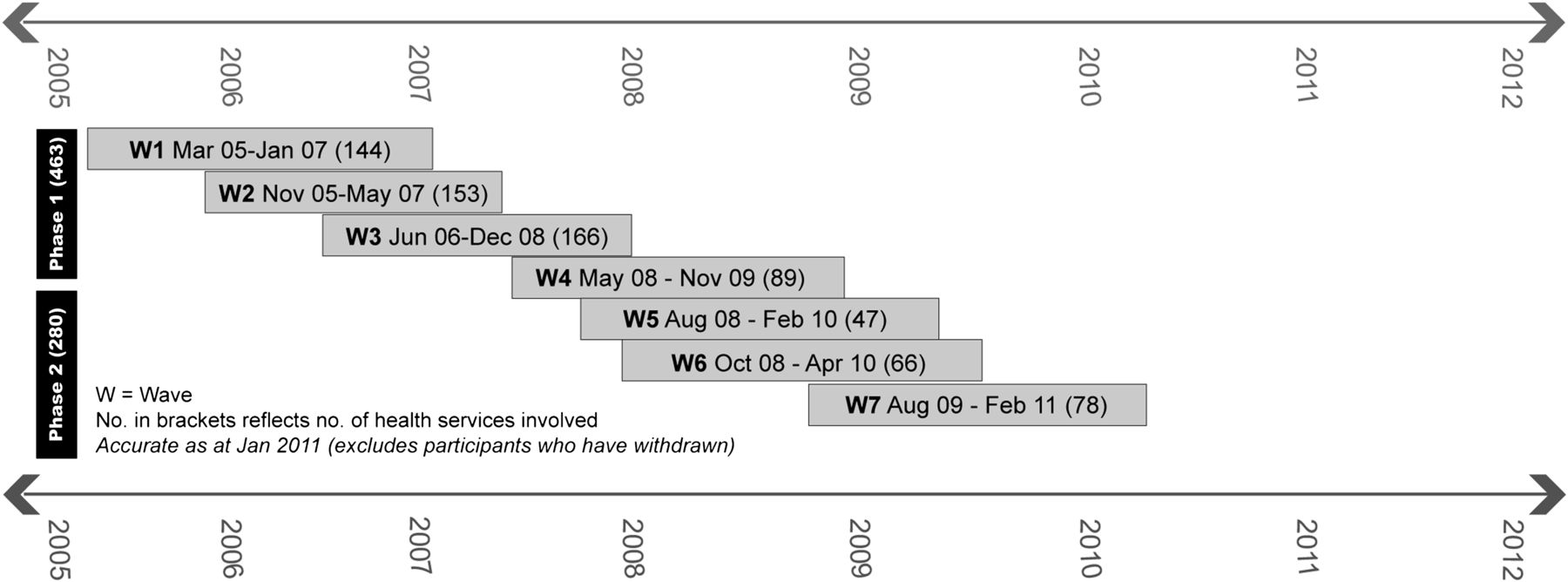
Timeline of diabetes waves in the Australian Primary Care Collaboratives Program.
Change in measures
Figure 3 charts the percentage of health services which were at the collaborative diabetes aim of having 50% of their patients with an HbA1C ≤7%. At baseline 49/743 (7%) health services were at the collaborative target. At month 17, 112/743 (15%) were at target.
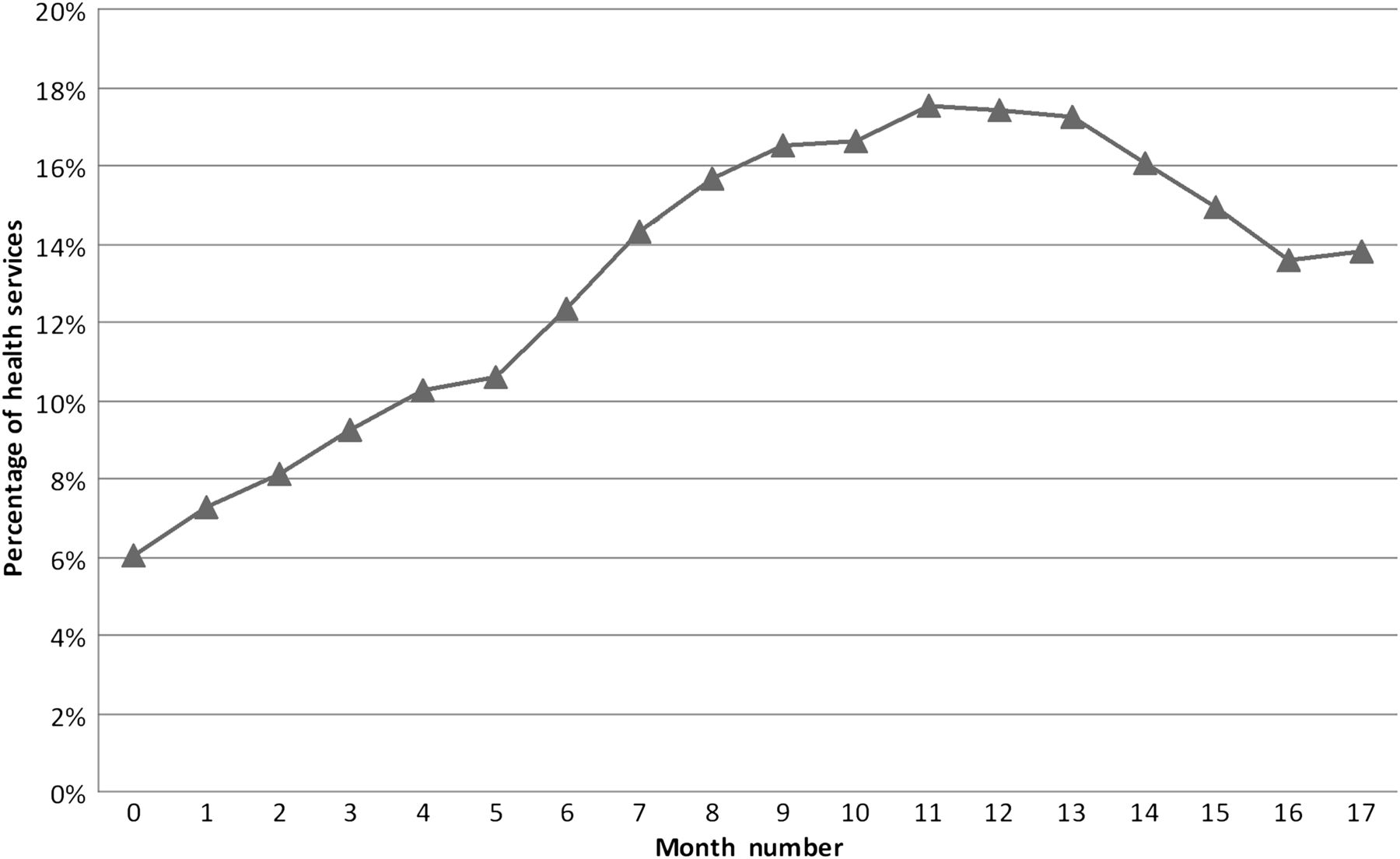
Percentage of health services achieving the collaborative aim of 50% of patients on the diabetes register having haemoglobin A1C ≤7 (n=743). This figure aggregates results from the seven waves occurring progressively over the project period.
The key clinical measure collected unchanged throughout the seven diabetes waves was the mean percentage of patients on each diabetes register in the health services with an HbA1C ≤7%. This measure improved from 25% at baseline to 38% by month 18. The graphs of individual waves and the graph summarising this across all 743 participating health services can be seen in figure 4.
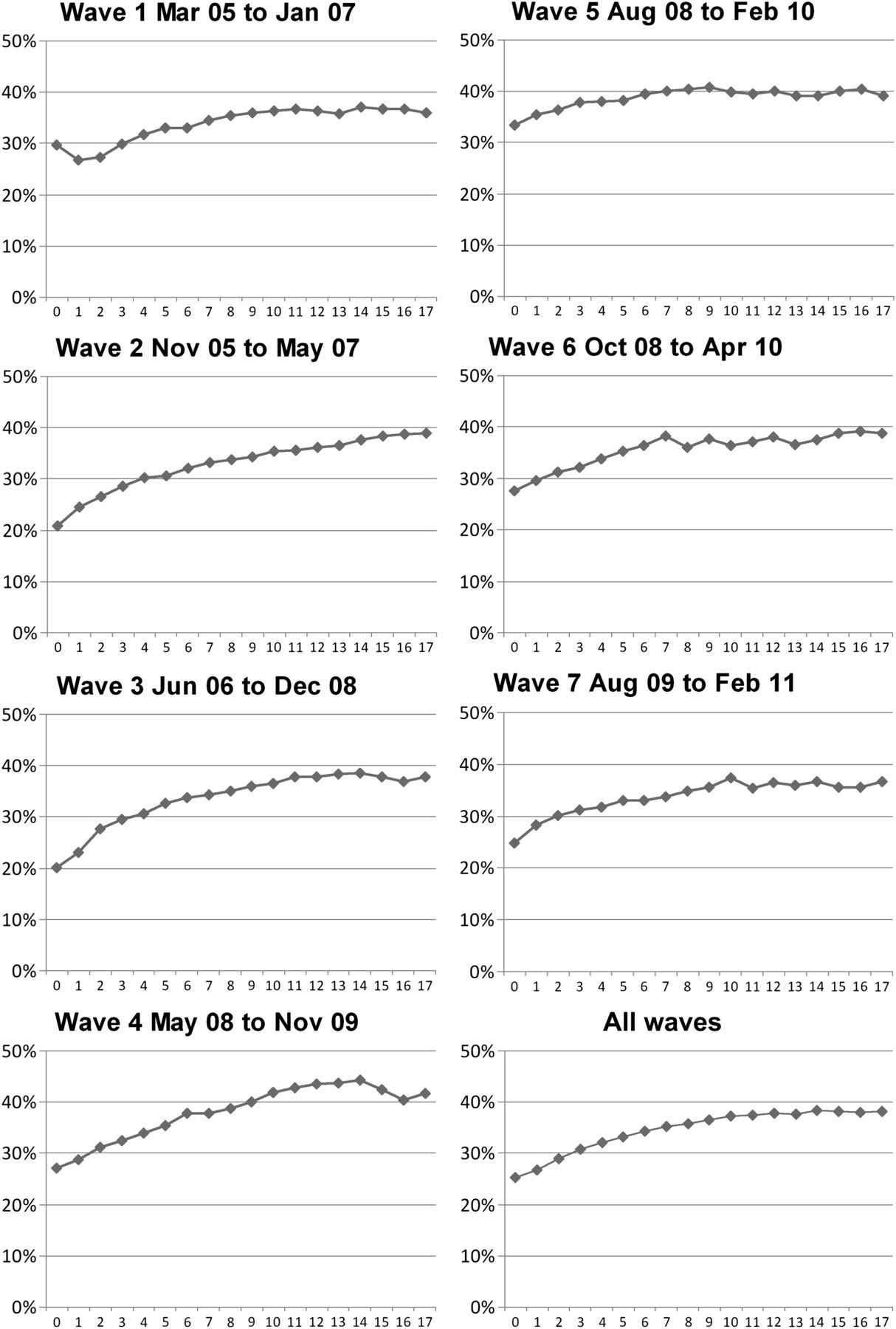
Mean percentage of patients on registers achieving haemoglobin A1C ≤7%. Results are from each wave with a final aggregated graph from all waves.
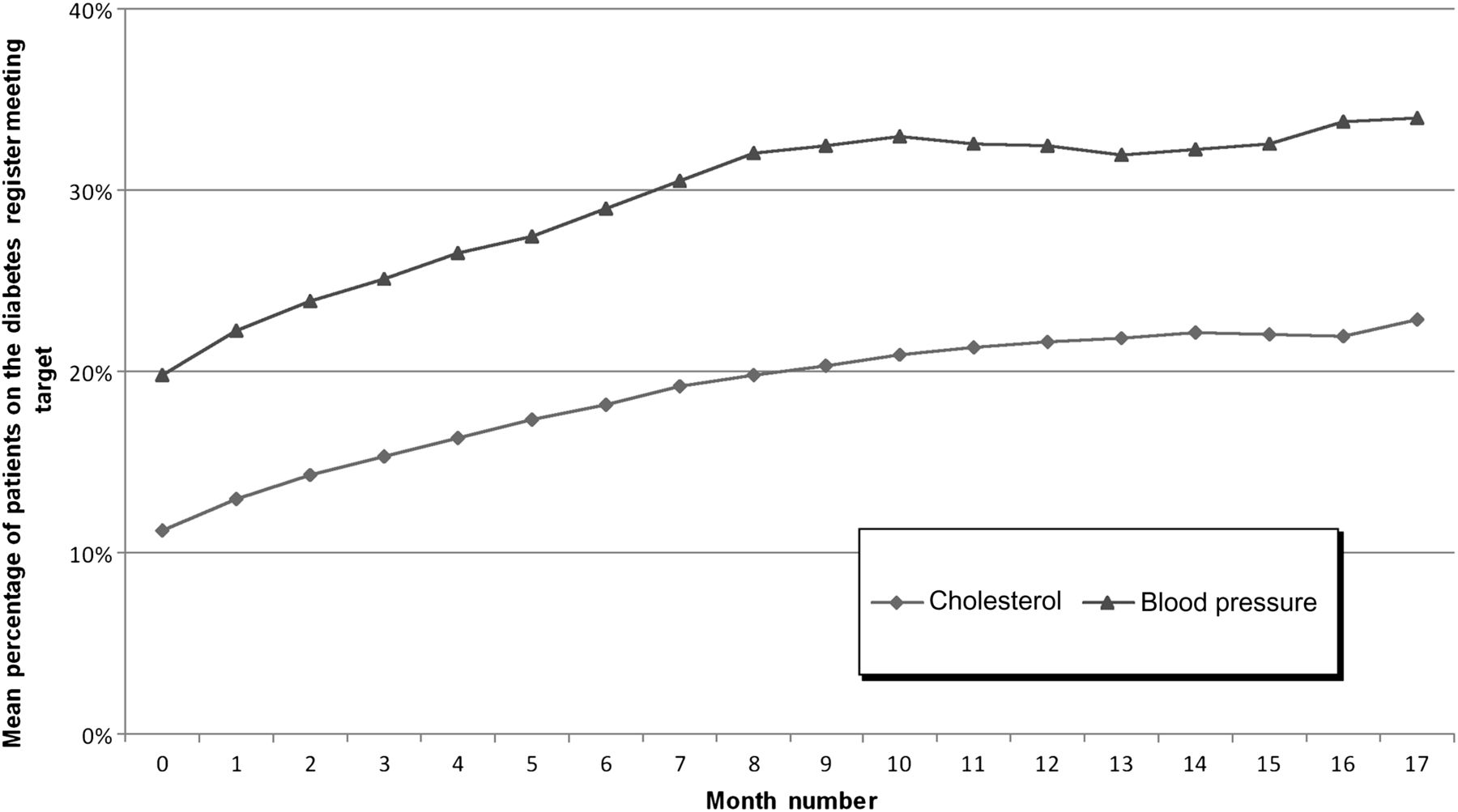
The mean percentage of patients at target increased from 11% to 22% for cholesterol and from 20% to 33% for blood pressure, as shown in figure 5.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean percentage of patients on registers at target for cholesterol and blood pressure measures (n=743). This figure aggregates results from the seven waves occurring progressively over the project.
Data completeness
The HbA1C measure submission rates ranged between 81% and 87% in the APCC. The mean percentage of patients on registers with an HbA1C recorded improved from 41% to 71%. The denominator used is the total of participating health services (n=743). See online figures 6 and 7 for graphs depicting these data.
Number of patients involved
Health services reported the size of their diabetes registers throughout the Program. Approximately 150 000 patients with diabetes were cared for over the seven waves of diabetes work in the APCC.
PDSA cycles submitted
Health services submitted 10 467 PDSA cycle reports in diabetes during their APCC involvement. An average of 13 diabetes PDSA cycles was reported per service (n=811).
Changes to the intervention
Teams returning to learning workshops two and three asked for help in engaging their colleagues in improvement. The APCC developed a ‘team change principle’ to help improve team functioning. This became the first change principle in all collaborative topics.
Data extraction software had some teething problems but became increasingly effective. As health services grew more sophisticated in their use of data they began to ask their software providers for improvements. Another provider developed a third party tool to do similar extraction work. A number of the improvement measures used by the APCC appeared in a suite of national performance indicators used in the health system and the software developed for the APCC was spread to many health services to facilitate collection of these measures.
Changes to the measures
The blood pressure measure was changed in 2006 by the ERP from ‘percentage of patients with a last recorded BP <130/80 in the last 12 months’ to ‘percentage of patients with a last recorded BP of ≤130/80 in the last 12 months’. This recognised the clinician approach that the target was achieved when blood pressure was recorded at the whole figure rather than below the whole figure. In addition, clinicians tended to round up or down to a whole number when recording blood pressure.
The cholesterol measure was changed at the same time to include a LDL-C measure of <2 mmol/litre as an alternative target to the original 4 mmol/litre for total cholesterol. This was in response to emerging evidence that LDL is a better measure for this risk factor while accommodating some lag in change in the clinical context.
The ERP recognized that important improvements in clinical care might not be captured by only measuring the percentage of patients with an HbA1C ≤7. In addition, evidence began to emerge during the life of the collaborative that the goal for HbA1C should be individualised to be optimal for different patient groups. In the second phase of the Program additional monthly feedback was provided to health services about patients in three bands: HbA1C >7 and ≤8, HbA1C>8 and <10 and HbA1C≥10.
Lessons and next steps
The APCC was a large undertaking with considerable risks in implementation. High levels of data reporting and the high average number of PDSA reports submitted indicate a significant amount of improvement work was undertaken by health services. The APCC has shown that it is possible to engage good numbers of divisions and health services in diabetes improvement and to sustain that engagement over years. This success indicates the ‘breakthrough’ collaborative approach was transferable to Australian primary care.
The measured improvements are large and consistent, showing a 50% improvement in mean percentage of patients at target for glycaemic control and similar improvements in blood pressure and cholesterol targets. It is likely that more improvement was achieved in the patient population as a whole than is indicated by these measures as many patients achieved improvements in their risk factors which were clinically important but fell short of meeting the target measure.
The outcome measures being clinical, numerical and collected directly from clinical software are likely to be robust. It should be noted that these improvements occurred in real world mainstream primary care health services across Australia and so demonstrate that the approach is feasible in busy service-focused workplaces.
The number of health services achieving the collaborative target peaked in month 11 and then fell back a little (figure 3). The mean percentage HbA1C ≤7 continued to rise (figure 4). It is possible that the fall in figure 3 reflects the difficulty in maintaining the very high performance of a smaller number of practices compared with the continued improvement in the large mass of reporting practices. It may also reflect a reduced number of reporting practices overall as the collaborative progressed and perhaps fatigue or loss of enthusiasm as the effect of the early workshops faded.
In an uncontrolled project such as this it may be argued that improvements have occurred due to other factors operating in the primary care environment. For instance, in the USA there has been a trend to lower HbA1C levels detected in people with diagnosed diabetes in the 11 years to 2005.22 The proportion of patients on registers at target may also improve if HbA1C is recorded for more patients. A rise in recording of HbA1C did occur in participating practices (see online figure 7). Both these factors could explain some of the changes reported. In the APCC each wave commencing over an interval of 5 years detected a low baseline measure of HbA1C at target and no rising trend is seen over the years. In addition, each wave showed a comparable degree of improvement over the course of the intervention (figure 3). These results provide evidence that the improvement occurred as a result of the intervention.
The APCC project was not just about redesign of clinical care. Participating health services were learning basic skills in developing and cleaning a disease register, coding patients accurately and learning to read and use data. Many had to address team dynamics. Teams tended to focus on these fundamental areas early in the collaborative before moving to redesigning clinical care as time passed. It is not possible to attribute the change in measures to any particular part of the intervention. Similarly it is not possible to determine to what extent diabetic care in participating health services has improved in isolation from the organisational and data improvements.
Nevertheless all of these changes are improvements. Improvements in administration, team functioning, data collection and accuracy underpin all other clinical care improvements and are an important outcome of the efforts of the APCC.
Lessons
More improvement is required
The collaborative method implemented in the APCC Program appears to deliver consistent and impressive improvements in measures. Services achieved an average of 38% of patients at HbA1C ≤7 and the number of practices achieved the collaborative aim of 50% of patients at target doubled to 15% at month 17. More improvement is needed if all patients are to receive the right care. This may require more concentrated collaborative efforts but will also require other policy levers such as incentives for improvement.
Chronic disease care versus focused topics
Many of the strategies used for diabetes care were the same as for coronary artery disease care and could be applied to any chronic disease. This supports suggestions by Wagner and others23 that primary care can provide integrated, generic chronic condition care across comorbidities.
However, health service teams seemed to elect to focus on particular diagnosis groups and even segments within that grouping to provide ‘digestible’ chunks of improvement work in which results could be achieved. This supports evaluations that participants engage better with the collaboratives focused on specific, measurable and achievable topics.
Groups implementing the collaborative methodology should use achievable topics to motivate teams while encouraging and facilitating generalisation of the principles to other conditions.
Build in evaluation from the start
The APCC would have benefited from stronger internal evaluation planned and budgeted for from inception. This would have been useful for planning improvements to the Program, to assure funders of value and for reporting the Program so that others may learn from it. Evaluation is required to identify with confidence the factors which determined why some practices made more improvement than others.
Focus on training, enthusing and resourcing the practice team
The practice team has been identified as key to improvements in primary care. When teams became motivated and skilled, improved care could happen quickly. Many teams seemed to be ready for the stimulus of contact with like-minded colleagues, education about effective strategies and challenge. The large collaborative workshops were good contexts for encouragement, healthy competition and sharing of ideas. Improvement science needs to be built into all levels of training of primary care team members.
Plan beyond the collaborative
The collaborative methodology is an effective short-term intervention for rapid change. After the collaborative the rapid change achieved must be consolidated and the investment leveraged by effective transition of participating practices to sustaining, long-term programs. This strategy is supported by evaluations of the methodology.24 Long-term support through data collection and feedback, support in improvement efforts and moving on to new areas for improvement should be provided by local organisations such as the divisions of general practice which are widespread throughout Australia. The aim should be to make quality improvement part of ‘business as usual’ for primary care service providers.
Make measure collection as easy as possible
The automated software in the APCC did not work well at the beginning of the first wave but persistence resulted in a better product that ensured collection of data was relatively easy for busy practices. Arduous measurement and reporting deplete resources needed for improvement.
Good local support increases improvement
Anecdotally good local support achieved better results as identified in collaborative evaluation literature.25 The CPMs of the APCC provided relationship and training close to the frontline. They need a good understanding of improvement, knowledge of the Program and good communication skills. The importance and role of CPMs should be evaluated in future projects.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure 1
- Data supplement 2 - Online figure 2
Footnotes
-
Funding The Australian Primary Care Collaboratives Program is funded by the Australian government Department of Health and Ageing and delivered by the Improvement Foundation (Australia) Ltd. The Improvement Foundation is a not-for-profit organisation whose core business is to provide expertise in the development and delivery of quality improvement programs to bring about systems change.
-
Competing interests None.
-
Ethics approval As a government-sponsored quality improvement project which used de-identified aggregated data for quality improvement purposes only, the Improvement Foundation was advised that ethics approval was not necessary for this Program.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement This article publishes a small indicative subset of the data collected by the APCC Program in the course of its improvement work. The complete dataset is held by the Improvement Foundation and is subject to agreements with participating health services which restrict its use. Researchers wishing to access the data may make direct contact with the Improvement Foundation (Australia).