Article Text

Abstract
Objective The objective of this review is to obtain a better understanding of the user-related barriers against, and facilitators for, the implementation of surgical safety checklists.
Methods We searched MEDLINE for articles describing stakeholders’ perspectives regarding, and experiences with, the implementation of surgical safety checklists. The quality of the papers was assessed by means of the Qualitative Assessment and Review Instrument. Thematic synthesis was used to integrate the emergent descriptive themes into overall analytical themes.
Results The synthesis of 18 qualitative studies indicated that implementation requires change in the workflow of healthcare professionals as well as in their perception of the checklist and the perception of patient safety in general. The factors impeding or advancing the required change concentrated around the checklist, the implementation process and the local context. We found that the required safety checks disrupt operating theatre staffs’ routines. Furthermore, conflicting priorities and different perspectives and motives of stakeholders complicate checklist implementation. When approaching the checklist as a simple technical intervention, the expectation of cooperation between surgeons, anaesthetists and nurses is often not addressed, reducing the checklist to a tick-off exercise.
Conclusions The complex reality in which the checklist needs to be implemented requires an approach that includes more than eliminating barriers and supporting facilitating factors. Implementation leaders must facilitate team learning to foster the mutual understanding of perspectives and motivations, and the realignment of routines. This paper provides a pragmatic overview of the user-related barriers and facilitators upon which theories, hypothesising potential change strategies and interactions, can be developed and tested empirically.
- Implementation science
- Patient safety
- Surgery
- Checklists
Statistics from Altmetric.com
Introduction
Surgical safety checklists are intended to ensure consistency in patient perioperative safety and to introduce or maintain a culture that values achieving it.1 The use of these checklists is associated with increased patient safety awareness, improved communication, reduction of surgical claims and reduction in the number of postoperative complications including mortality.2–10 It cannot, however, be assumed that the mere application of the checklist will automatically lead to improved safety.11–13 Reported compliance with checklist items is assumed to be correlated with the impact of surgical safety checklists.10 ,14 Consequently, the clinical effectiveness of the checklist will vary with the implementation success.15 ,16
The implementation of new guidelines and safety interventions has been shown to be difficult in various healthcare sectors, which highlights the importance of the implementation process.17–19 Several studies have reported high levels of participation and checklist completion (ranging from 12% to 100%).20 However, the implementation is more than merely ‘checking the box’. A discrepancy between ticking off checklist items and the performance of the actions results in poor fidelity as regards the checklist's intentions.21–29 The implementation of a surgical safety checklist is a complex social intervention. Factors influencing the dissemination and uptake of evidence-based interventions or technological innovation may, therefore, not apply. In order to increase the understanding of the user-related barriers to, and facilitators of, the implementation of surgical safety checklists, we conducted a systematic review of the qualitative literature.
Methods
Design
A synthesis of the qualitative evidence synthesis was formulated by means of thematic synthesis.30 The strength of this methodology is its potential to enable conclusions to be drawn on the basis of common elements of otherwise heterogeneous studies. Conclusions drawn from thematic analysis fulfil an important research aim of qualitative research by generating hypotheses for which traditional systematic reviews are poorly suited.30
Search strategy
The search was performed in MEDLINE (from inception to March 2015) using the following query: (“Surgical Procedures, Operative”[Mesh] OR “surgical” OR “surgery” OR “operative)” AND (“checklist”[MeSH] OR “checklist” OR “time-out)” AND (“fidelity” OR “implementation” OR “adherence” OR “compliance” OR “barriers” OR “facilitators” OR “incentives”). Broad search terms were applied without date restrictions in order to make the search strategy as sensitive as possible. Methodological filters for study design were not used because they reduce the sensitivity of searches.31 ,32 The reference lists of all of the papers were scrutinised, and a cited reference search was made in the Web of Science for additional papers on the subject.
Inclusion criteria
Qualitative studies that explored the perspectives and experiences of stakeholders with the implementation of surgical safety checklists were included. These stakeholders were nurses, surgeons, anaesthesiologists, residents, implementation leaders, administrators and any others directly involved in, or affected by, the implementation. Following the guidance of the Cochrane Qualitative Research Methods Group, which considers critical appraisal to be a technical and pragmatic exercise, we restricted the type of qualitative studies included in this review.33 Only empirical studies with a description of the sampling strategy, the data collection procedures and the type of data analysis were included. These empirical studies had to report the methodology chosen and the methods or research techniques opted for since this facilitates the systematic use of critical appraisal as well as a more pragmatic appraisal process. Therefore, descriptive papers, editorials and opinion papers that were not based on actual experiences related to the implementation of surgical safety checklists were excluded. No language or country restrictions were applied.
Quality assessment
The primary goal of our quality assessment was to highlight the quality of the published literature on the subject. The full texts of the included articles were reviewed by two independent authors (JB and PS) using the Qualitative Assessment and Review Instrument (QARI).34 The 10 QARI criteria do not relate to validity or bias in the process-orientated methods as regards the reviews of effects, their purpose being to establish the nature and appropriateness, the methodological approach, the specific methods and the representation of the voices or meanings of the study participants.35 However, given that there is no accepted method for excluding qualitative studies from the syntheses on the basis of their quality, we did not exclude studies based on the QARI scoring.36 ,37
Extracting data from studies
A data extraction form was developed cataloguing the author, year of publication, journal, method of data collection, phenomena of interest, study setting, country of study, data analysis and main conclusions. In syntheses of qualitative research, the ‘informants’ are the authors of the individual studies rather than the participants in these studies. Therefore, the authors’ interpretations—presented, for example, by themes and categories—constitute our data. While the authors’ interpretations were collected primarily from the results sections, data found in the discussion sections were also extracted when relevant and well supported by data.
Thematic synthesis
Thomas and Harden described thematic synthesis as “a tried and tested method that preserves an explicit and transparent link between the conclusions and text of the primary studies; as such it preserves principles that have traditionally been important to systematic reviewing”.30 Thematic analysis has three stages: (a) line-by-line coding of the findings of primary studies to extract the key concepts, (b) organisation of these key concepts into related areas to construct ‘descriptive’ themes that formed the backbone of the structure of the analysis and (c) development of ‘analytical’ themes based on the synthesis of the experiences and recommendations of authors of the original articles. While the development of descriptive themes remains close to the primary studies, the analytical themes represent a stage of interpretation in which the reviewers go beyond the primary studies and generate new interpretive constructs, explanations or hypotheses.
QSR International's NVivo 10 software was used to organise the codes into hierarchical structures.38 The text of each included study (results and discussion section) was imported into the software verbatim. One of us (JB) developed a set of descriptive codes inductively by coding each line of the text of all of the included studies. We looked for similarities and differences between the codes in order to start grouping them into a hierarchical tree structure, and new codes were created to catalogue the meaning of groups of initial codes. This process resulted in a tree structure with several layers in order to organise the descriptive themes. The groupings were then further refined by discussion and rechecking of the original studies (JB, FL and PS). Successive drafts of a narrative that described the themes seen in the findings were then discussed by the wider study group (JB, FL, PS, AV and DV) and further refined. All of the stages of the process were checked by various experts (an organisational psychologist, safety culture experts and patient safety experts) to ensure accuracy and control of bias in the analysis.
Results
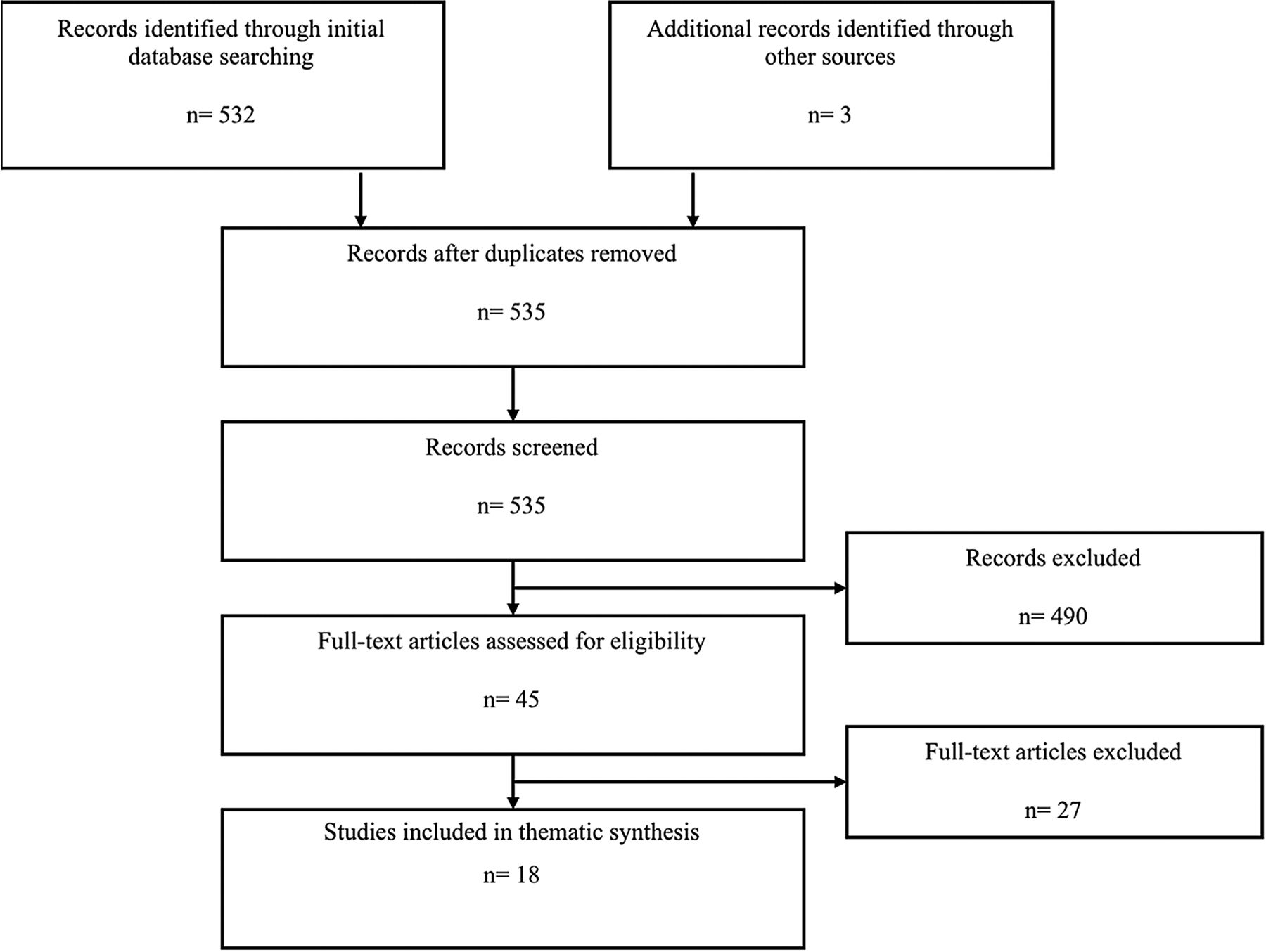
The search strategy yielded 535 papers. Screening for eligible and inconclusive abstracts reduced this list to 45 papers. After full-text review, 27 studies21 ,22 ,27–29 ,39–60 were excluded from the final analysis (see online supplementary appendix 1 for further explanation). We included 18 studies involving >700 healthcare professionals (see figure 1).25 ,61–77 The studies involved 18 different countries. The data in these studies had been collected using interviews, focus groups, observations and open-ended surveys. A detailed overview of the study characteristics is provided in online supplementary appendix 2.

PRISMA diagram.
Quality assessment
Overall, the selected studies scored well on the QARI (see online supplementary appendix 3 for an overview of QARI scoring). Nevertheless, only 4 of the 18 papers stated the cultural and/or theoretical location of the researcher, so it was difficult to appraise his/her potential influence on the study findings and vice versa. Adequate representation of the participants, and their opinions, was not provided in five studies, and the congruity between the stated philosophical perspective and the research methodology was often difficult to evaluate. No additional exclusions were made after the technical appraisal.
Synthesis findings
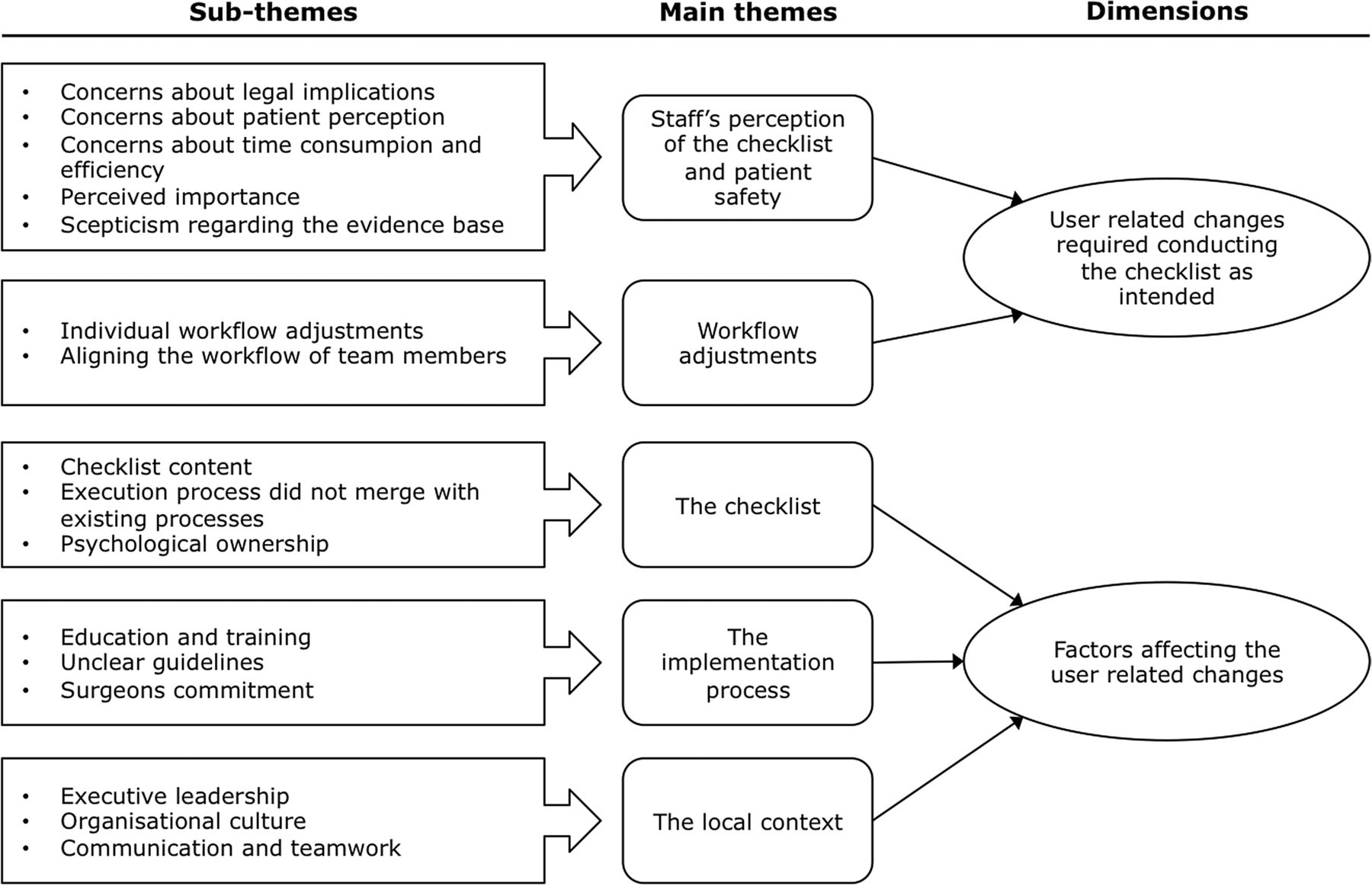
The thematic analysis of the primary articles revealed five main themes with respective subthemes. Two of these main themes—staffs’ perception of the checklist and patient safety, and workflow adjustments—represent user-related changes required to conduct the checklist as intended (dimension one). The other three main themes—checklist, implementation process and local context—constitute factors affecting the user-related changes (dimension two). Figure 2 shows our data structure. It provides a graphical representation of how we progressed from subthemes (the result of grouping key concepts from the primary studies) to main themes describing the two dimensions.
{kind=link}
{kind=link}
Data structure.
User-related changes required to conduct the checklist as intended
In order to implement the checklist and assure it is used as intended, changes on the user level (ie, doctors and nurses) are needed. In what follows, we describe the main themes and subthemes related to this first dimension. Illustrative quotations for each of the themes are provided in table 1.
Themes describing user-related changes required conducting the checklist as intended with exemplary citations from the study findings
Staffs' perception of the checklist and patient safety
The perception of the staff of the checklist and its items, and the perception of patient safety in general, determines the individual willingness to use the checklist. Healthcare providers expressed concerns about legal implications, which hampered their willingness to use the checklist. Participants, especially nurses, expressed concerns about patient perception, which led to the omission of items they perceived as causing stress in patients (eg, expected blood loss) or performing the checks without verifying out loud. Most of the studies reported concerns about time consumption and efficiency. Participants felt, or presumed, that checklist execution consumed too much time and thereby hampered operating theatre efficiency. The perceived importance of the checklist items varied across professions and individuals, which led to varying usage and support among surgeons, anaesthesiologists and nurses. The perceived importance is strongly related to understanding the intentions and aims of the checklist. In addition, risk perception plays an important role in the conviction that risks assumed by the checklist exist in the immediate work environment. Finally, scepticism regarding the evidence base was expressed. Surgeons and anaesthetists, in particular, believed that the existing evidence was inconclusive and did not support general implementation of surgical safety checklists.
Workflow adjustments
Implementation of the checklist requires modification of operating theatre staffs’ workflow. Proper execution of the safety checks introduced by the checklist involves changes in the workflow of the operating theatre staff, which was often experienced as an increased workload. Besides individual workflow adjustments, alignment between the workflows of surgeons, anaesthesiologists and nurses is needed in order to execute the brief stops (ie, sign in, time out and sign out) required to complete the checklist. Aligning the workflow of team members is difficult to achieve. In addition, the checklist sometimes entails the repetition by nurses or doctors of one or more safety checks—as some are already included in existing procedures—the redundant registration thus creating an administrative burden. As a result, doctors and nurses might experience the checklist as an additional, often unnecessary, task.
Factors affecting the user-related changes
Several factors act as a barrier or facilitator to the user-related changes required to precede checklist usage. In what follows, we describe the main themes and subthemes related to this second dimension. Illustrative quotations for each of the themes are provided in table 2.
Themes describing the factors affecting the user-related changes with exemplary citations from the study findings
The checklist
A first theme emerged around design problems influencing staff perception and workflow. Many healthcare providers found the content somehow irrelevant to their setting or suggested rewording certain items to create a better fit with actual usage. Layout and form factor issues (eg, inconvenient format or complex computer applications) were also expressed. Second, respondents found that the execution process did not merge with existing processes. This created redundant safety checks and administration or even conflicting workflows. Linked to beliefs and prejudices, as previously mentioned, professionals need to experience psychological ownership, meaning that they must have the feeling that the intervention is created, or at least tailored, to their needs. This sense of ownership seems crucial in convincing doctors to use the checklist. Even though the checklist is supported by evidence and is endorsed by leading organisations (eg, professional associations), individuals may have a different opinion on its usefulness and importance. Some parts or items of the checklist are perceived as relevant only to specific professionals, which diluted the sense of shared responsibility.
The implementation process
The implementation process refers to the joint activity of implementing the checklist by actors who, in relation to checklist implementation, engage in particular ways of relating over time.78 This process must create a clear transition period supporting the acquisition of the new workflow. A large part of the implementation effort entails education and training. Participants from the original studies found explaining why the checklist is necessary, providing clear communication on organisational intentions, and addressing the concerns expressed by staff to be of vital importance for creating support and willingness prior to the actual implementation. In addition, participants found it important to show them how they must use the checklist. Healthcare providers found that unclear guidelines hampered checklist execution. Therefore, the introduction needs to be supported with clear guidelines and training on how, when and who will execute the checklist. During the implementation process, the commitment of all of the professionals is required to sustain checklist usage. Nurses found surgeon commitment to be imperative. Given the hierarchical context within the operating theatre, senior surgeons’ leadership is of undeniable importance.
The local context
The local context refers to the local historical-relational context of checklist implementation that is always partly created in the joint activity that the actors engage in.78 Participants expressed that, in addition to general leadership, executive leadership is needed to communicate the importance of the checklist and patient safety in general. Executive leadership needs to be exercised in order to create a context in which doctors and nurses feel supported. Across studies, respondents saw the organisational culture as a major barrier but also as a potential facilitating element. Both the hospital-wide and the immediate organisational culture play a mediating role. Although checklist usage is expected to change the safety culture, there is a very complex relationship between the checklist, the procedures, the context, the culture and the behavioural changes.72 With the deepening of the culture, respondents found that communication and teamwork issues hamper checklist execution. These issues often stem from a hierarchical team culture that obstructs the open culture and communication required to execute the checklist correctly. The social interaction between team members has a great impact on nurses’ decision to participate in checklist usage. They seem to adjust their team involvement according to the practical, social and professional conditions in their work environment.
Analytical themes
Up to this point, we have produced a synthesis that kept very close to the original findings of the studies. ‘Going beyond’ the content of the original studies has been identified by some as the defining characteristic of synthesis.30 With the development of analytical themes, we ‘went beyond’ the findings of the primary studies and generated additional concepts, understandings or hypotheses.
Disrupted routines and conflicting priorities
The introduction of a checklist in the operating theatre involves doctors and nurses changing existing routines.25 Workflows on the individual, professional or team level have to be altered and aligned in order to create a brief moment of reflection to review the safety checks collectively.25 ,61–63 ,74 ,76 ,77 The workflow introduced by the checklist often collides with existing routines.61 ,63 This creates conflicts as existing workflows are established in function of different priorities (eg, efficiency or productivity).61 ,62 ,66 ,68 ,77 Hence, the priority of patient safety, introduced by the checklist, has to compete with the already existing clinical and organisational priorities. Conflicts between priorities compel doctors and nurses to weigh using the checklist against other priorities. When a conflict in priorities emerges, the perceptions of operating theatre staff regarding patient safety drive their ultimate decision about whether or not to use the checklist.66
Different perspectives and motives
The motivation for implementing a surgical safety checklist differs between healthcare providers and hospital management.62 ,70 ,75 ,77 The use of a surgical safety checklist is often part of hospital-accreditation requirements or other quality-improving programmes. Management feels, with the perspective of obtaining accreditation, that it is necessary to apply the checklist very strictly. Healthcare providers, however, feel that some of the checklist items have little or no relevance in their specific setting. Without clear communication about the motives of hospital management, perspectives drift apart and resistance towards the checklist develops. The perspective and motivation of the doctors may also differ from those of the nurses. Because of organisational requirements, nurses feel it necessary to use the checklist while doctors may not always concur with these requirements.66
The checklist is implemented as a simple technical intervention
The implementation of checklists is more than requiring that box be checked off: it is a complex social intervention with an expectation of interaction and cooperation between surgeons, anaesthetists and nurses.63 ,66 ,75 However, this important aspect is often poorly addressed during implementation. Implementation teams should, therefore, promote and support inter-professional communication when introducing the checklist. If not, the checklist will be used as a tick-off exercise.79
Discussion
This systematic review comprehensively investigates user barriers and facilitators to the implementation of surgical safety checklists. Although the themes have been presented separately, implementation problems are multifactorial, highly interdependent and affected by considerable clinical complexity. Many themes were common to papers regardless of interstudy differences in geographical or clinical setting.
It was found that the implementation of a surgical safety checklist requires change in perception of the operating theatre staff regarding the checklist and its items, and the perception of patient safety in general. In addition, doctors and nurses need to adjust their workflows. These changes are impeded or advanced by characteristics of the checklist, the implementation process and the local context.
Based on the experience of high-reliability organisations, characteristics of the checklist (eg, length, layout and design, and content) are important.44 The content of the checklist needs to be supported by scientific evidence and written in clear, understandable words preferably embedded within existing processes. The checklist must precisely mirror the intended operation without creating ambiguity or confusion. The checklist and its items must be relevant to the applied setting. Exporting a checklist to situations in which it was not meant to be used may impede further checklist implementation.63 Obstacles stemming from the checklist apply not only to the content but also to psychological ownership. Doctors and nurses need to feel as though the checklist has become a part or an extension of their selves. In other words, they have to feel that it is ‘mine’ or ‘ours’.80 Even better is collective psychological ownership, with the entire operating theatre staff feeling that the checklist is part of them and their work.81
The implementation process itself can act as a barrier and so create aversion. As with any new procedure or guideline implementation, the checklist creates uncertainty and questions. Lack of consensus guidelines will lead to personal interpretations and enhance confusion. Therefore, the introduction needs to be supported by clear guidelines on how, when and who will execute the checklist. These guidelines need to be formalised in a written procedure, and the execution of the checklist also needs to be demonstrated. Small-scale tests can familiarise doctors and nurses with the checklist and experiment with workflow adjustments. Reactions to these tests can be used to alter or clarify checklist guidelines and procedures. Surgeons, who play the central role during the procedure, are often seen as leaders in the operating theatre. Research on the broader context of patient safety has shown that senior staff may not always be the best source of patient safety knowledge and skills.82 This suggests that surgeons not only need to be supported but also to be educated. A promising approach to deal with the difficulties associated with changing routines can be found in team learning.83 Successful implementers used enrolment to motivate the team, designed preparatory practice sessions and early trials to create psychological safety (ie, a shared belief that the team is safe for interpersonal risk taking) and encourage new behaviours, and thus promote shared meaning and process improvement through reflective practices.83 ,84
The local context in which the checklist has to be implemented is important. The organisational culture—that is, a social-organisational phenomena, in terms of behaviour or attitudes, that emerges from a common way of sense making, based on shared values, beliefs, assumptions and norms85—influences the behaviour and perception of doctors and nurses. People often view themselves as members of a community of practice with established norms and processes that can change only when the entire group changes. For example, a new workflow practice or technology standard may be difficult to adopt unless the entire group agrees at the same time to use the system. To improve the safety culture in the operating theatre, interventions should aim at minimising the hierarchy and empowering nursing staff in addition to standardising and structuring the practicalities concerning the use of the checklist. Such initiatives need to be performed by the operating theatre management.66 Second, leadership (ie, the process of social influence in which one person can enlist the aid and support of others in the accomplishment of a common task86) from senior staff and the chief surgeon has been frequently presented as a key to successful implementation.25 ,62–64 ,66 ,68 ,69 ,72 In addition, participants found executive leadership equally important. It is important to show that patient safety is regarded as a priority in the hospital.62 ,64 ,66 ,69 ,72 Finally, communication and teamwork have a profound influence on checklist usage. The existence of a professional hierarchy in medicine and the differential status accorded to those in different disciplines hampers teamwork and communication. Profession-derived status is associated with psychological safety, so it is important to have a sense of confidence that the team will not embarrass, reject or punish someone for speaking up when noticing a real or potential safety problem. Psychological safety is a key antecedent of speaking up and learning behaviour in healthcare teams.87 It is suggested that leader inclusiveness moderates the relationship between status and psychological safety.87
We found that the workflow introduced by the checklist often collides with existing routines.61 ,63 This creates conflicts as existing workflows are established to achieve different priorities (eg, efficiency or productivity). The effect of disrupted routines has previously been recognised during the implementation of new technology in hospitals.83 Conflicts between priorities compel doctors and nurses to balance using the checklist against other priorities. When a conflict in priorities emerges, the perceptions of the operating theatre staff regarding patient safety drives their ultimate decision whether or not to use the checklist. We found that stakeholders’ perspectives and motives towards the checklist often differ. These different views create tension and aversion. In order for a checklist to be considered a priority, staff's perceptions and attitudes regarding it and patient safety in general must be supportive. Therefore, the safety checklist will be of little value if disruptive attitudes and behaviours are not addressed.88 This is in line with the establishment of a climate of safety (ie, shared perceptions among the staff concerning the policies, procedures, practices and kinds of behaviours that will be rewarded and supported with regard to safety89 ,90). This requires that a good safety climate must be established prior to, and during, implementation. New routines require adjustment and training. An important feature of checklists is the combination of checks ensuring adherence to proven practices (eg, administration of antibiotics and use of pulse oximeters) and other non-technical items (eg, team introductions and confirmation of procedures). The principal purpose of these non-technical items is to promote specific aspects of teamwork, communication and situational awareness.72 However, education and training during checklist implementation often neglects these non-technical items. The importance of team learning and training in order to modify teamwork and communication has been implemented with positive effects.91
The checklist is in essence a complex social intervention aimed to improve communication and teamwork in a strictly hierarchical context. Even when initial perceptions and attitudes regarding the checklist are positive,92 it does not guarantee long-term improvement.93 The existing hierarchies and the tribal affiliations of professional groups must be altered in order to create psychological safety. Each member has to be allowed to take interpersonal risk by speaking up if any concern about safety arises without being afraid of being embarrassed, rejected or punished.87 ,94 Implementation is much more complex than addressing the barriers and enabling the facilitators found in this review. Implementation is an ever-changing process for change in one aspect can generate a reaction in one or several other aspects and thereby create a wholly new environment. Hence, it is not enough to have a list of barriers and facilitating factors: we also need to deal with the interaction between them.
Strengths and limitations of this study
The results of this thematic synthesis should be interpreted within certain limitations. First, only one electronic database (MEDLINE) was consulted. To mitigate the potential loss of relevant articles, a cited and citing reference study in Web of Science was conducted. Second, assessing the quality of the included studies remains controversial in qualitative reviews. The QARI was selected because it is referred to as the most coherent instrument for evaluating the validity of qualitative research.34 Last, this review specifies a list of themes that are believed to influence checklist implementation but does not specify the interactions between them.
The current research also has some notable strengths. First, to the best of our knowledge, this is the first overview of qualitative research on the barriers and facilitating factors regarding the implementation of checklists. The results of this study present the barriers and facilitators that play during the implementation of many patient safety initiatives in healthcare and, therefore, present a valuable learning opportunity. Second, the use of thematic synthesis enabled the synthesis of the results of otherwise heterogeneous studies.
Conclusions
Implementation of a checklist requires structural changes in workflow of the operating theatre staff workflow, as well as in their perceptions regarding the checklist and patient safety in general. The required changes are impeded or advanced by three main factors: the checklist, the implementation process and the local context. However, the complex reality in which the checklist is implemented requires an approach that includes more than getting rid of the barriers and supporting facilitating factors. Implementation leaders must facilitate team learning to foster mutual understanding of the perspectives and motivation and the adaptation of existing routines. This paper provides a pragmatic overview of the constructs upon which theories, hypothesising potential change strategies and interactions, can be developed and tested empirically.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
- Data supplement 3 - Online appendix 3
Footnotes
Contributors Study concept and design: JB and DV. Acquisition of data: JB, PS and AV. Collection, analysis and interpretation of data: JB, FL, PS, AV and DV. Draft of the manuscript: JB. All authors contributed substantially in reviewing the manuscript and approved the final version.
Funding Limburg Sterk Merk.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.