Article Text

Abstract
Objective To evaluate a quality improvement (QI) programme to increase the use of maternal breast milk (MBM) in preterm infants.
Design Interrupted time series analysis.
Setting 17 neonatal units in the East of England (EoE) Perinatal Network; 144 in the rest of the UK Neonatal Collaborative (UKNC).
Patients Infants born ≤32+6 weeks gestation admitted to neonatal care between 2009 and 2012.
Intervention A ‘care bundle’ to promote MBM in the EoE.
Outcomes Percentage of infants receiving exclusive or any MBM at discharge and care days where any MBM was received.
Methods Data were extracted from the National Neonatal Research Database; outcomes were compared preintervention and postintervention, and in relation to the rest of the UKNC.
Results Exclusive and any MBM use at discharge increased from 26% to 33% and 50% to 57% respectively in the EoE, though there was no evidence of a step or trend change following the introduction of the care bundle. Exclusive MBM use at discharge improved significantly faster in EoE than the rest of the UKNC; 0.22% (95% CI 0.11 to 0.34) increase per month versus 0.05% (95% CI 0.01 to 0.09, p=0.007 for difference). The percentage of infants receiving MBM at discharge and care days where any MBM was received was not significantly different between EoE and the rest of the UKNC.
Conclusions This QI programme was associated with some improvement in MBM use in preterm infants that would not have been evident without the use of routinely recorded national comparator data.
- care bundle
- quality improvement
- breast milk
- preterm
- Nutrition
Statistics from Altmetric.com
What is already known on this topic
-
Maternal breast milk (MBM) is beneficial to preterm infants and improves short-term and long-term outcomes.
-
Quality improvement (QI) programmes using ‘care bundle’ methodology where multiple interventions work synergistically to improve outcomes.
-
Evaluation of QI programmes is important but analytical quality is variable, often with a lack of comparator groups and failure to consider underlying trends.
What this study adds
-
The East of England (EoE) perinatal network successfully implemented a care bundle to promote MBM feeding across 17 neonatal units.
-
During the study period, the rate of exclusive MBM at discharge improved significantly faster in EoE than the rest of the UK Neonatal Collaborative.
-
Using interrupted time series methodology and population-based data as a comparator are feasible, cost-effective, robust methods to evaluate QI programmes in the UK.
Introduction
The benefits of maternal breast milk (MBM) are widely recognised and include reduction in late-onset sepsis and necrotising enterocolitis1–4 and improved neurodevelopment.5 The wide variation in breast feeding at discharge among mothers delivering preterm suggests that intervention may be beneficial. Quality improvement (QI) programmes such as ‘care bundles’, a group of evidence-based interventions that, when executed together, result in better outcomes than when implemented individually, offer opportunities through altered clinical behaviours across multidisciplinary teams to deliver cohesive and consistent good practice. The East of England (EoE) perinatal network introduced a care bundle to increase the use of MBM in preterm infants. The development and implementation of the care bundle have been previously described.6 Here, we present an evaluation of the impact of the care bundle.
Methods
Setting: neonatal units
The National Health Service (NHS) in England delivers neonatal care through clinical networks. The EoE perinatal network includes 17 neonatal units, with approximately 70 000 births a year. Comparator data were drawn from the rest of the UK Neonatal Collaborative (UKNC). At the time of analysis, the UKNC consisted of 161 out of 166 neonatal units in England that contribute electronic operational clinical data to the National Neonatal Research Database (NNRD).
Study population: patients
Data on all infants born ≤32+6 weeks gestation admitted to participating neonatal units were included.
Intervention: care bundle
A summary of the components of the care bundle is provided in table 1; the project conception and implementation outline is provided in online supplementary table S1. The care bundle consists of four elements: promotion of early milk expression, ongoing support for expressing and breast feeding up to discharge, standardised enteral feeding practice and an aseptic non-touch technique for milk preparation.
Components of the care bundle
Outcome measures
The following outcomes were evaluated for infants born ≤32+6 weeks gestation:
-
(1) Monthly percentage of infants receiving exclusive MBM at discharge
-
(2) Monthly percentage of infants receiving any MBM at discharge
-
(3) Monthly percentage of care days where any MBM was received.
Data extraction
Data were obtained from the NNRD. The NNRD is created from extracts from a real-time patient management system and managed by the Neonatal Data Analysis Unit. It is approved by the National Research Ethics Service (ref 10/H0803/151), the Confidentiality Advisory Group of the Health Research Authority (ref 8-05(f)/2010) and the Caldicott Guardians of each contributing NHS trust.
As the care bundle was not implemented in neonatal units outside of the EoE, the rest of the UKNC served as a natural comparator group. For outcomes (1) and, (2), data were extracted for infants discharged from neonatal care between 2009 and 2012 and assigned to month of discharge. Readmissions to neonatal care were not included. For outcome (3), data were extracted on care days occurring between 2009 and 2012 and assigned to month of occurrence.
Data quality
From the second quarter of 2011, data validation studies were conducted in the EoE as part of data quality assurance to determine agreement between the NNRD and medical notes for 12 variables (including discharge feeding). Studies were conducted on 34 infants per month (two per neonatal unit) who had been discharged from neonatal care the previous month. Findings relating to data accuracy and completeness were fed back through the monthly newsletters.
Data analysis
Data were analysed using interrupted time series (ITS), a technique to test whether an effect observed after the introduction of the care bundle was different from any pre-existing trend.7 The intervention was introduced in January 2011 and was fully implemented by March 2011; therefore, February 2011 was used as the ‘interruption’ time point. This provided data for the 25-month period preimplementation (January 2009 to January 2011) and the 23-month period postimplementation (February 2011 to December 2012). Segmented linear regression was used to estimate the step change and trend change. Autocorrelation (the correlation of errors which are closer together in time) was assessed using residual plots, and the Breusch–Godfrey test.8 ,9 If evident, first-order autocorrelation was accounted for using the Prais–Winsten procedure.10 MBM feeding outcomes for the EoE were compared with the rest of UKNC, by including an interaction term, to test whether the time trend was significantly different in the two regions. If there was no evidence of either a trend change or a step change, the change over the whole 4-year period was evaluated. SAS V.9.2 and STATA 11 were used for the analyses; statistical significance was set at p=0.05.
Adjusted analysis
To investigate whether the results were influenced by confounding factors (gestation, birth weight, sex, multiple birth, maternal age and maternal smoking during pregnancy), segmented logistic regression was performed on the individual-level data. Higher order terms were tested if graphical investigation indicated a non-linear relationship. SEs were estimated with the cluster bootstrap procedure to account for correlated outcomes within multiple birth sets. It was not possible to adjust for differences in neonatal characteristics3 as the longitudinal analysis required was not computationally feasible for a dataset of this size. Sensitivity analyses were performed to assess the impact of missing data assuming ‘best-case’ (all infants with missing data received MBM) and ‘worst-case’ scenarios (no infants with missing data received MBM).
Results
Compliance with the care bundle
As previously reported, compliance improved steadily in the first 6 months following implementation to a peak of 90% in August 2011.6
Data quality
Completeness of NNRD discharge feeding data improved from 81%–85% to 96%–99% and the agreement with handwritten medical notes improved from 51%–57% to above 80% towards the end of the study (table 2). It became apparent from the data validation study that electronic operational clinical data from which the NNRD is constructed were being increasingly used to replace handwritten documentation in the medical notes. Therefore, rather than comparing the NNRD against medical notes as ‘gold standard’, we assessed the agreement between the two sources of data.
East of England (EoE) discharge feeding data extracted from the National Neonatal Research Database (NNRD): completeness and agreement with medical notes
Patient characteristics
Discharge feeding data from 3680 infants born ≤32+6 weeks gestation from the EoE region and 29 492 infants from the rest of the UKNC were included for the analysis of outcomes (1) and (2). Daily data on around 330 000 care days for the EoE and 2.85 million care days from the rest of the UKNC were included in the analysis for outcome (3). Population characteristics are shown in table 3. Statistically significant differences between the EoE region and the rest of the UKNC were noted for birth weight, sex, multiple birth and maternal age, though these were not clinically relevant.
Population characteristics for infants born ≤32+6 weeks gestation and discharged from neonatal care during 2009–2012
Outcomes (1) (exclusive MBM) and (2) (any MBM) at discharge
Table 4 shows the annual MBM feeding rates at discharge in the EoE and UKNC. This shows an increase in exclusive (26%–30% EoE and 30%–31% UKNC) and any (50%–57% EoE and 49%–51% UKNC) MBM at discharge between 2009 and 2012.
Annual maternal breast milk (MBM) feeding rates at discharge by East of England and rest of UK Neonatal Collaborative (UKNC)
East of England
Results of the ITS analysis for the EoE alone are shown in table 5. There was no evidence of a significant time trend before or after the intervention, nor was there evidence of a step change or trend change for outcomes (1) or (2). Figure 1A shows a scatter plot of the percentage of infants exclusively MBM fed at discharge against month, with superimposed lines to indicate estimated preintervention and postintervention trends; figure 1B shows the same for any MBM feeding. Adjustment for potential confounders using logistic regression did not alter the conclusions (see online supplementary table S2).
Segmented regression analysis of East of England data
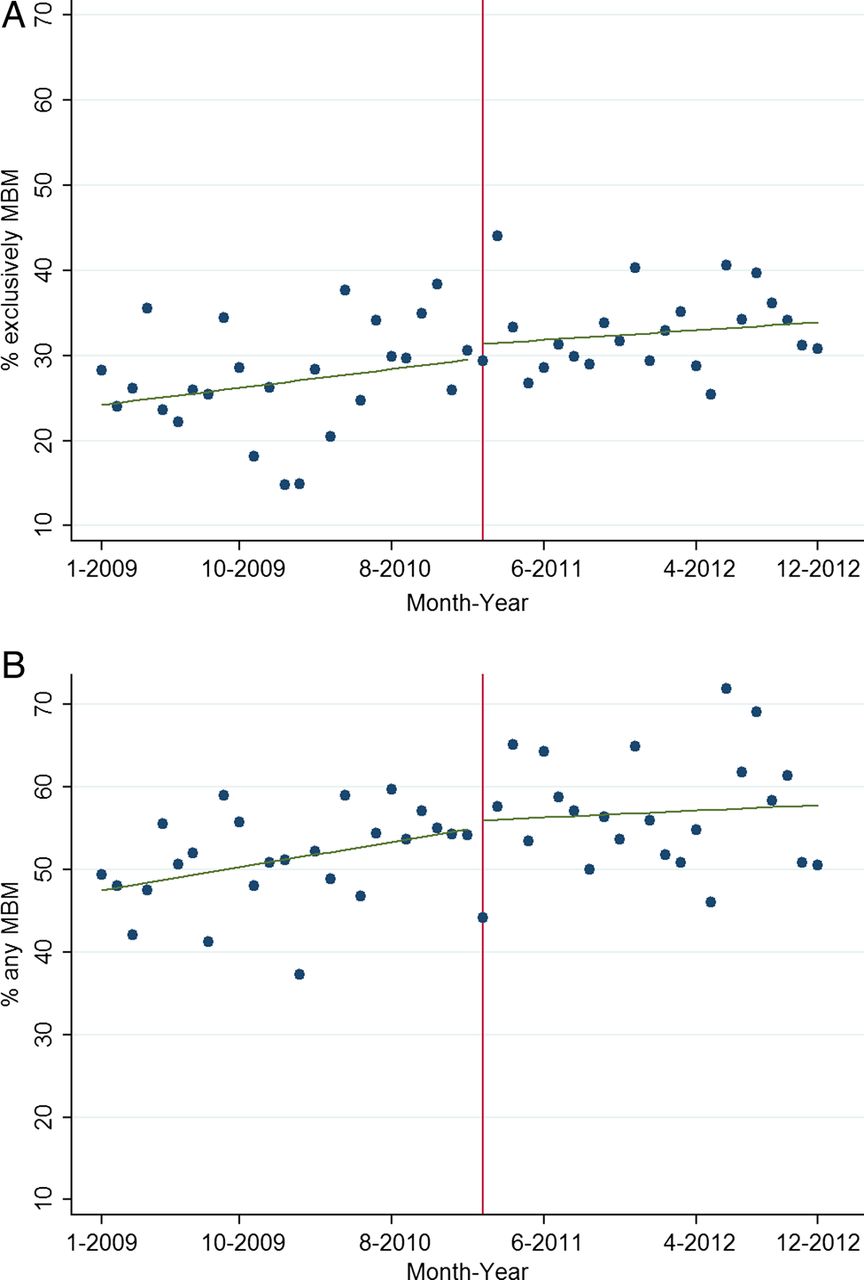
(A) Percentages of infants fed exclusive maternal breast milk (MBM) at discharge in the East of England (EoE) region by month of discharge. The red line indicates the point when the intervention was introduced; the green lines are trends estimated by the segmented regression. Note that there was no statistically significant difference in the preintervention and postintervention trends, or in the step or trend change at the intervention. (B) Percentages of infants fed exclusive or any MBM at discharge in the EoE region by month of discharge. The red line indicates the point when the intervention was introduced; the green lines are trends estimated by the segmented regression. Note that there was no statistically significant difference in the preintervention and postintervention trends, or in the step or trend change at the intervention.
Comparison with UKNC
Outcome (1) (exclusive MBM at discharge): The percentage of infants who were exclusively MBM fed on discharge increased significantly faster in the EoE compared with UKNC; 0.22% (95% CI 0.11, 0.34, p<0.001) per month in the EoE versus 0.05% (95% CI 0.01 to 0.09, p=0.01) per month in the rest of the UKNC (figure 2). The difference in time trend was statistically significant (p value for interaction between region and time=0.007). At the start of the study, the rate of exclusive MBM feeding at discharge was 5.1% (95% CI 1.7 to 8.5, p=0.004) higher in the rest of the UKNC compared with EoE, but this difference was no longer apparent by the end of the period (UKNC 3% lower, 95% CI −6.3, 0.3, p=0.07). Adjustment for potential confounders using logistic regression did not alter the conclusions.
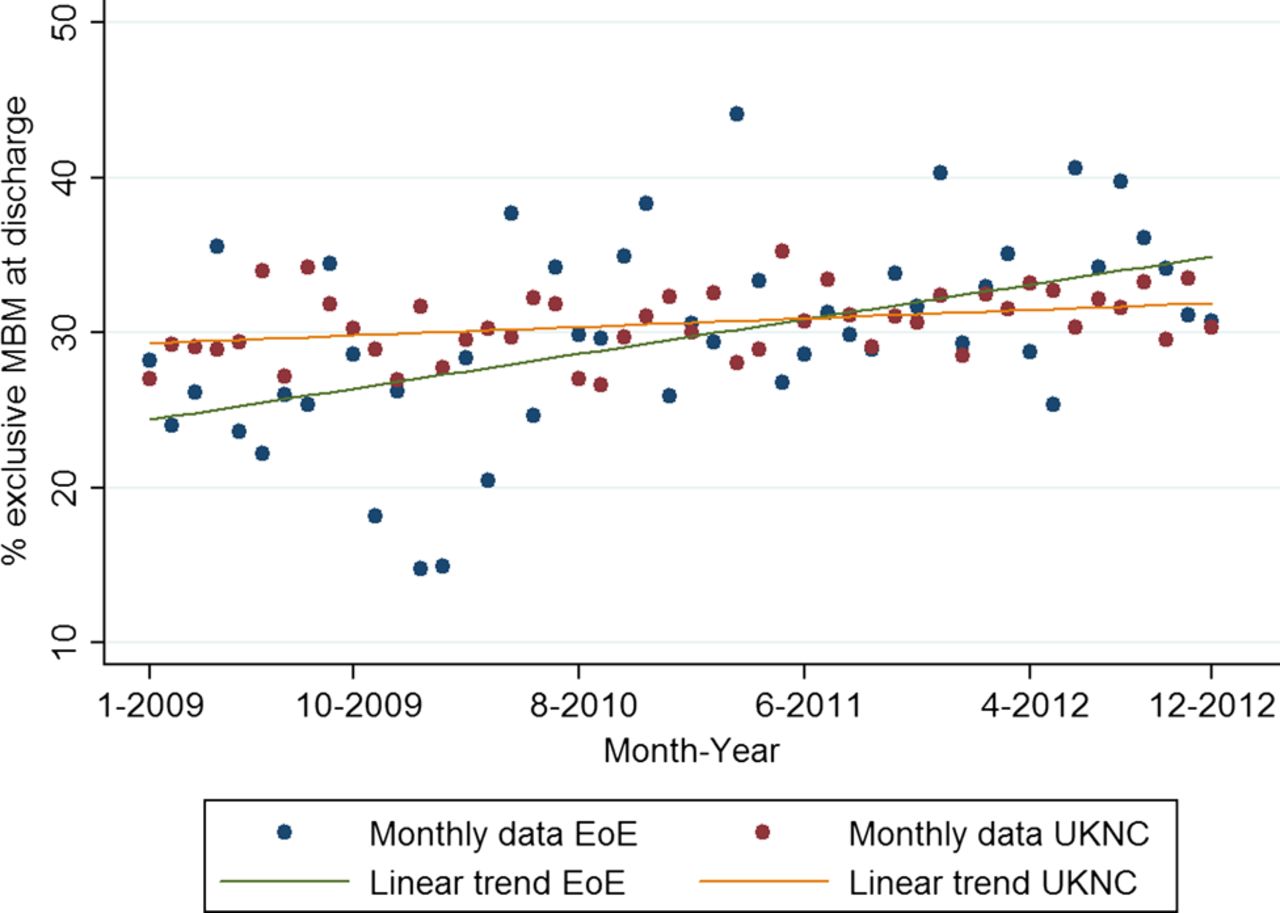
Monthly percentages of infants exclusively fed maternal breast milk (MBM) in the East of England (EoE) region (blue dots for data, green line for estimated trend from regression) and the rest of the UK Neonatal Collaborative (UKNC) (red dots for data, yellow line for estimated trend from regression) by month of discharge.
Outcome (2) (any MBM at discharge): The rate of any MBM feeding at discharge in the EoE increased by 0.23% per month (95% CI 0.10 to 0.36, p<0.001) compared with 0.15% (95% CI 0.11 to 0.20, p<0.001) in the rest of the UKNC. This difference in trends was not statistically significant (p value for interaction between region and time=0.26). Adjustment for potential confounders using logistic regression did not alter the conclusions.
Outcome (3) (percentage of care days with any MBM)
East of England
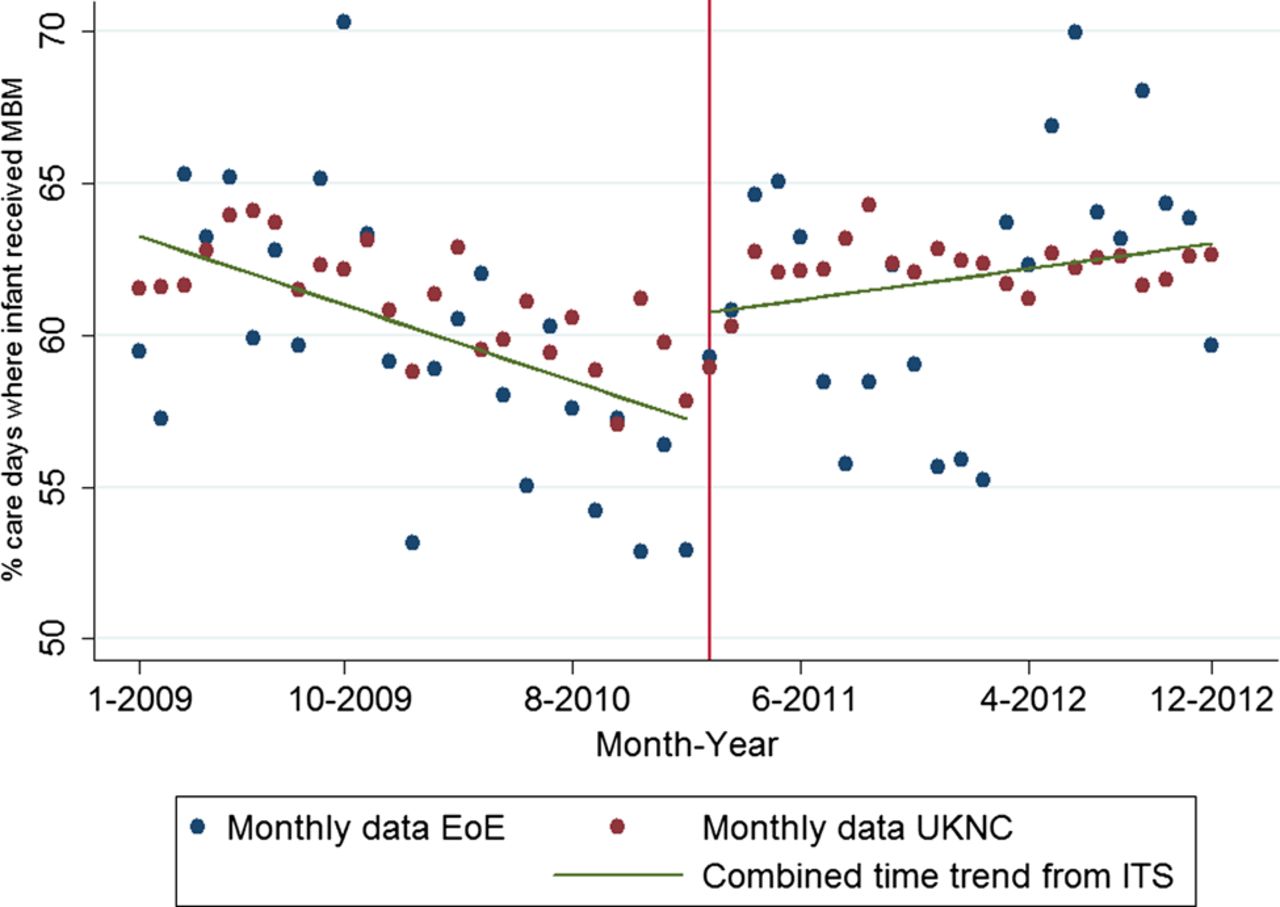
The ITS analysis showed that the percentage of care days with any MBM was in slight decline prior to the introduction of the bundle (−0.3% per month, 95% CI (−0.6, −0.06), p=0.02). The step change at the point of introduction was not significant (5% increase (−0.6, 11), p=0.08), nor was the trend after introduction (0.2% per month (−0.2, 0.5), p=0.4). However, the change in trend from preintroduction to postintroduction did show a significant improvement (difference in trends 0.5% (0.04, 1.0), p=0.03).
Comparison with UKNC
Similar patterns were observed in the UKNC data with a significant improvement in trend (0.2% (0.09, 0.35), p=0.001). There was also a step change of 2.7% (95% CI (1.0, 4.4), p=0.002). There was no significant difference in trends between the EoE and UKNC, and so we used ITS to estimate combined trend (figure 3).

{kind=link}
{kind=link}
{kind=link}
Monthly percentages of care days where infants were fed any maternal breast milk in the East of England (EoE) region (blue dots) and the rest of the UK Neonatal Collaborative (UKNC) (red dots) by month of discharge. The red line indicates February 2011, the care bundle ‘interruption’ time point in the EoE. Both EoE and UKNC showed a significant trend change after February 2011, but as there were no significant differences between EoE and the rest of the UKNC, trends from the interrupted time series from the combined analysis are shown (green line).
Missing data and sensitivity analysis
Data on MBM feeding at discharge were missing for 5% of infants and 4% of care days. The sensitivity analyses for missing data did not yield differing conclusions.
Discussion
We show that exclusive MBM at discharge increased in both the EoE and the UKNC over the 4-year evaluation period in relation to the introduction of a care bundle, but the rate in the EoE improved significantly faster. Rates of improvement were similar before and after the care bundle was introduced so it is likely that the pattern during implementation was a continuation of an existing underlying trend. For MBM during the neonatal stay, EoE data showed a significant improvement in the time trend after the bundle was introduced but a similar pattern also occurred in the rest of the UKNC. Therefore, although notable improvements were seen in the use of MBM in the EoE, these cannot be attributed with certainty to the introduction of the care bundle.
Implementation does not translate into immediate adoption and compliance requires time, involving a complex process of changes in practices, culture and beliefs. It is conceivable that delays embedding the care bundle compromised ability to detect a step change as a result of the intervention. Other factors may have influenced preterm breast feeding in the rest of the UKNC and attenuated the differences with EoE. These included an increase nationally in the uptake of the UNICEF Baby Friendly Initiative, the launch of a national programme to promote breast feeding by the Best Beginnings charity (personal communication) and in some regions the introduction of a Commissioning for Quality and Innovation payment to incentivise breast feeding. In addition, the care bundle was widely presented outside the EoE, with information packs made available and it is plausible that the adoption by other neonatal units may have also led to an attenuation of differences between EoE and the UKNC.
Our study has several strengths. To our best knowledge, this is the first reported QI project related to preterm infant feeding using ITS methodology and population-based data as a comparator. In our study, rates of MBM feeding at discharge were increasing before the intervention. If a ‘before and after’ design with single time points had been employed, as is widely practised, the underlying trend would not have been identified and it may have been inferred wrongly that the improvement in outcomes was definitely attributable to the care bundle. Independent factors coinciding with the intervention can also influence outcomes. We were able to compare data in the EoE with population-based data from the rest of the UKNC which reflect other changes occurring concurrently independent to the intervention. Although small and unlikely to be of clinical relevance, we found statistically significant differences in birth weight, sex, multiple birth and maternal age between EoE and the rest of the UKNC. The availability of these and other variables allowed for adjustment of confounding factors giving greater confidence in the inferences drawn. We conducted sensitivity analyses which showed that the conclusions were unaffected by missing data. We were unable to control for confounding in the analysis of daily feeding data, although the same pattern was seen in the EoE and the UK, and little difference in neonatal characteristics was seen over the period.
Assessing QI programmes requires high quality data and rigorous analysis to minimise bias as is accepted practice for intervention studies.11 ,12 We were able to analyse population-based feeding data from the NNRD that contain information from over 95% of neonatal units in England. Data that are routinely available facilitate rigorous and robust evaluation reducing both cost and burden to busy health professionals. However, this approach requires data that are complete and accurate. For example, the paradoxical declining trend in MBM use during admission in both EoE and UKNC prior to February 2011 was an unexpected finding as both exclusive and any MBM at discharge were increasing over the same time period. Sensitivity analyses excluded the possibility that this was due to missing data. Formal data validation was undertaken in EoE but inaccurate data in the rest of the UKNC may have contributed to this paradoxical finding.
Wider acceptance of QI programmes is likely to derive from clear demonstration of impact and can be argued is essential where public resources are being used. We recommend careful advance consideration to define methods for evaluating QI programmes prior to their implementation in the NHS. The use of existing national comparator data offers a unique opportunity for UK neonatal services to conduct high quality evaluations.
Acknowledgments
We thank the care bundle champions in the EoE who developed and implemented the care bundle, the EoE neonatal teams who contributed to the data validation studies, and the support of neonatal unit managers. We acknowledge assistance from Ian Long, EoE data analyst, Daniel Gray and Yevgeniy (Eugene) Statnikov, Neonatal Data Analysis Unit analysts and manager Richard Colquhoun, and the support of members of the Neonatal Data Analysis Unit Steering Board, and the Medicines for Neonates Programme Steering Committee (Jane Abbott, Deborah Ashby, Peter Brocklehurst, Kate Costeloe, Elizabeth Draper, Michael Goldacre, Jacquie Kemp, Azeem Majeed, Stavros Petrou, Andrew Wilkinson, Alys Young, Vimal Vasu, Jacquie Dopran, Jon Dorling, Alex Allwood).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Collaborators Data from the following UK Neonatal Collaborative neonatal networks (neonatal units: lead neonatal clinician) were included in this study: East of England Perinatal Network (Basildon Hospital: Dr N Sharief; Bedford Hospital: Dr R Kadalraja; Broomfield Hospital: Dr R N Mahesh Babu; Colchester General Hospital: Dr S Dalton; Hinchingbrooke Hospital: Dr H Dixon; Ipswich Hospital: Dr M James; James Paget Hospital: Dr V Jayalal; Lister Hospital: Dr J Kefas; Luton & Dunstable Hospital: Dr S Skinner; Norfolk & Norwich University Hospital: Dr M Dyke; Peterborough City Hospital: Dr S Babiker; Princess Alexandra Hospital: Dr T Soe; Queen Elizabeth Hospital: Dr S Rubin; Rosie Maternity Hospital: Dr A Ogilvy-Stuart; Southend Hospital: Dr A Khan; Watford General Hospital: Dr C Ramesh; West Suffolk Hospital: Dr I Evans). Rest of the UKNC by network: Cheshire & Merseyside (Arrowe Park Hospital: Dr O Rackham; Countess of Chester Hospital: Dr S Brearey; Leighton Hospital: Dr A Thirumurugan; Macclesfield District General Hospital: Dr I Losa; Ormskirk District General Hospital: Dr T McBride; Warrington Hospital: Dr C Zipitis; Whiston Hospital: Dr L Amegavie). Greater Manchester (North Manchester General Hospital, Royal Oldham Hospital, Salford Royal: Dr J Moise; Royal Albert Edward Infirmary: Dr C Zipitis; Royal Bolton Hospital: Dr P Settle; St Mary's Hospital: Dr N Edi-Osagie; Stepping Hill Hospital: Dr C Heal; Tameside General Hospital: Dr J Birch; University Hospital of South Manchester: Dr F Al-Zidgali). Kent & Medway (Darent Valley Hospital: Dr A Hasib; Maidstone, Tunbridge Wells Hospital: Dr H Kisat; Medway Maritime Hospital: Dr A Soe; Queen Elizabeth the Queen Mother Hospital, William Harvey Hospital: Dr M Kumar). Lancashire & Cumbria (Furness General Hospital, Royal Lancaster Infirmary: Dr J Fedee; Lancashire Women and Newborn Centre, Burnley: Dr M Lama; Royal Preston Hospital: Dr R Gupta; Victoria Hospital: Dr Rawlingson). Midlands Central (George Eliot Hospital: Dr RC de Boer; Kettering General Hospital: Dr. P Rao; Northampton General Hospital: Dr S Thompson; Queen's Hospital Burton on Trent: Dr A Manzoor; University Hospital Coventry: Dr K Blake; Warwick Hospital: Dr A Upponi). Midlands North Staffordshire, Shropshire and Black Country (Manor Hospital: Dr AK Bhaduri; New Cross Hospital: Dr C Halahakoon; Royal Shrewsbury Hospital: Dr Deshpande; Russells Hall Hospital: Dr A Mohite; Staffordshire General Hospital: Dr KK Tewary; University Hospital of North Staffordshire: Dr K Palmer). Midlands South West (Alexandra Hospital, Worcestershire Royal Hospital: Dr A Gallagher; Birmingham City Hospital: Dr J Nycyk; Birmingham Heartlands Hospital, Good Hope Hospital: Dr P Simmons; Birmingham Women's Hospital: Dr I Morgan; Hereford County Hospital: Dr HC Underhill). North Central London (Barnet Hospital, Chase Farm Hospital: Dr T Wickham; The Royal Free Hospital: Dr V van Someren; University College Hospital: Dr S Watkin; Whittington Hospital: Dr R Blumberg). North East London (Homerton Hospital: Dr N Aladangady; King George Hospital, Queen's Hospital: Dr B Sharma; Newham General Hospital, North Middlesex University Hospital: Dr L Alsford; The Royal London Hospital, Whipps Cross University Hospital: Dr C Sullivan). North Trent (Barnsley District General Hospital: Dr S Hamdan; Bassetlaw District General Hospital, Diana Princess of Wales Hospital, Scunthorpe General Hospital: Dr P Adiotomre; Doncaster Royal Infirmary: Dr JS Ahmed; Chesterfield & North Derbyshire Royal Hospital: Dr A Foo; Rotherham District General Hospital: Dr R Talekar; The Jessop Wing, Sheffield: Dr A Gibson). North West London (Chelsea & Westminster Hospital: Dr M Thomas; Ealing Hospital: Dr R Mathur; Hillingdon Hospital: Dr M Cruwys; Northwick Park Hospital: Dr P Mannix; West Middlesex University Hospital: Dr H Ariff). Northern (Cumberland Infirmary, West Cumberland Infirmary; Dr Whitehead and M Ben-Hamida; Darlington Memorial Hospital, University Hospital of North Durham: Dr M Garbasa; James Cook University Hospital, Friarage: Dr M Lal; Queen Elizabeth Hospital, Gateshead: Dr D Bosman; Royal Victoria Infirmary: Dr A Fenton; South Tyneside District Hospital: Dr AR Bolton; Sunderland Royal Hospital: Dr M Abu-Harb; University Hospital of North Tees: Dr B Reichert; Wansbeck General Hospital: Dr J Olivier). Peninsula (Derriford Hospital: Dr J Larson; North Devon District Hospital: Dr Y Cherinet; Royal Cornwall Hospital: Dr P Munyard; Royal Devon & Exeter Hospital: Dr N Osbourne; Torbay Hospital: Dr M Raman). South East London (Guy’s & St Thomas’ Hospital: Dr T Watts; King's College Hospital: Dr Hannam; Princess Royal University Hospital, Queen Elizabeth Hospital: Dr S Walter; University Hospital Lewisham: Dr J Kuna). South West London (Croydon University Hospital: Dr YL Chang; Epsom General Hospital, St Helier Hospital: Dr R Shephard; Kingston Hospital: Dr D Lindo; St George's Hospital: Dr C Huddy). South Central South Coast (North & South) (Basingstoke & North Hampshire Hospital: Dr R Wigfield; Dorset County Hospital: Dr P Wylie; Milton Keynes Foundation Trust Hospital: Dr I Misra; Oxford University Hospitals, Horton Hospital & John Radcliffe Hospital: Dr N Shettihalli; Poole Hospital NHS Foundation Trust: Dr M Khashu; Princess Anne Hospital: Dr M Hall; Queen Alexandra Hospital: Dr C Groves; Royal Berkshire Hospital: Dr P de Halpert; Royal Hampshire County Hospital: Dr D Schapira; Salisbury District Hospital: Dr S Kinsey; St Mary's Hospital: Dr S Butterworth; St Richard's Hospital: Dr N Brennan; Stoke Mandeville Hospital: Dr G Whitehead; Wexham Park Hospital: Dr R Sanghavi). Surrey and Sussex (Conquest Hospital, Eastbourne District General Hospital: Dr G Whincup; East Surrey Hospital: Dr K Khader; Frimley Park Hospital: Dr A Mallik; Princess Royal Hospital, Royal Sussex County Hospital: Dr P Amess; Royal Surrey County Hospital: Dr C Godden; St Peter’s Hospital: Dr P Reynolds; Worthing Hospital: Dr N Brennan). Trent (King's Mill Hospital: Dr V Noble; Lincoln County Hospital and Pilgrim Hospital: Dr AS Rao; Nottingham City Hospital, Nottingham University Hospital (QMC): Dr S Wardle; Royal Derby Hospital: Dr M Ratnayaka). Western (Gloucestershire Royal Hospital: Dr J Holman; Great Western Hospital: Dr S Zengeya; Royal United Hospital: Dr S Jones; Southmead Hospital: Dr R Wach; St Michael's Hospital: Dr J Tooley; Taunton & Somerset Hospital: Dr RJ Mann; Yeovil District Hospital: Dr M Eaton). Yorkshire (Airedale General Hospital: Dr M Babirecki; Bradford Royal Infirmary: Dr S Seal; Calderdale Royal Hospital: Dr K Schwarz; Dewsbury & District Hospital, Pontefract General Infirmary (Pinderfields): Dr D Gibson; Harrogate District Hospital: Dr C Jampala; Hull Royal Infirmary: Dr P Pairaudeau; Leeds Neonatal Service: Dr L Miall; Scarborough General Hospital: Dr M Qunib; York District Hospital: Dr G Millman). The Neonatal Data Analysis Unit: Jane Abbott, Deborah Ashby, Peter Brocklehurst, Kate Costeloe, Elizabeth Draper, Michael Goldacre, Jacquie Kemp, Azeem Majeed, Stavros Petrou, Andrew Wilkinson, Alys Young, Vimal Vasu, Jacquie Dopran, Jon Dorling, Alex Allwood.
-
Contributors CB, SS and NM developed the study protocol, SS analysed the data and CB wrote the first draft of the paper. MU was the care bundle QI programme lead, LR wrote the standardised feeding guideline and JB was medical lead. All authors reviewed the paper, suggested revisions and approved the final version submitted; NM is the guarantor.
-
Funding CB and SS receive salary support from the National Institute for Health Research through a Programme Grant for Applied Research Programme Grant, Medicines for Neonates (RP-PG-0707-10010) held by NM. MU and LR received support from the EoE Perinatal Network.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms