Article Text

Abstract
Aims: To estimate the incidence of active tuberculosis (TB) and study the use of chemoprophylaxis for latent TB in children in Wales, and to identify potential areas for improving prevention and management.
Methods: Active surveillance for TB in children aged 0–15 years from July 1996 to December 2003, using the Welsh Paediatric Surveillance Scheme.
Results: A total of 232 children, 102 with active TB (2.3 per 100 000) and 130 with latent TB (2.9 per 100 000), were identified. Nearly half (45%) belonged to ethnic minorities (19% were of black African origin), a much higher proportion than the base population. Pulmonary disease was the most common presentation (47%), including six (9%) children who were sputum smear positive. There were 10 cases of disseminated TB, nearly all in white children under 10 years of age. Less than two thirds of eligible children (27/46, 59%) were known to have received BCG immunisation. The source of infection was an adult household contact in most cases, but was not known in 44 cases, particularly among teenagers. Four community outbreaks occurred during the surveillance period, including three in high schools.
Conclusion: TB incidence in children in Wales remains low, but the epidemiology is changing with an increasing proportion of cases in black African children. The high proportion of patients with disseminated TB is of particular concern. TB in teenagers was often associated with school outbreaks. Many eligible children do not receive BCG immunisation, indicating further scope for prevention.
- ISC, Indian subcontinent
- TB, tuberculosis
- WPSS, Welsh Paediatric Surveillance Scheme
- chemoprophylaxis
- disease management
- health surveillance
- tuberculosis
- Wales
Statistics from Altmetric.com
Tuberculosis (TB) is an important cause of morbidity and mortality in children worldwide, especially in resource poor countries.1 In England and Wales, annual TB notification rates declined steadily for over a century but levelled off in the mid 1980s and have increased gradually since, particularly in urban areas and among recent immigrants.2,3 Childhood TB remains relatively uncommon except in certain parts of London where rates of over 40/100 000 have been reported.4 Nevertheless, any child presenting with TB is an important sentinel event, usually indicating recent transmission from an infectious adult.5 Infected children also represent a pool from which a large proportion of future adult TB cases will arise. Understanding the epidemiology of childhood TB is therefore important in an effort to control and ultimately eliminate the disease. TB in children also poses unique challenges for the clinician. Diagnosis is often more difficult than in adults, particularly as regards microbiological confirmation, and young children are more likely to develop disseminated disease.5
Routine TB surveillance in the United Kingdom (UK) is based on statutory notification. However, only limited data are collected and the system is affected by under-reporting.6 A retrospective study of childhood TB in Wales from 1986 to 1992 highlighted deficiencies in both reporting and clinical management.7 Since 1996, we have conducted active, prospective surveillance for TB through the Welsh Paediatric Surveillance Scheme (WPSS) in order to estimate the incidence, describe the epidemiology, and promote better case management.
METHODS
The WPSS was established in 1994 to study the epidemiology of uncommon childhood disorders in Wales.8 Its work complements that of the British Paediatric Surveillance Unit and uses similar methodology.9 Approximately 100 cards are sent out monthly to consultant paediatricians and senior clinical medical officers in Wales who are requested to send the cards back even if there are no cases to report. A negative reply is thus as important as a case report. Reminders are sent to all doctors who have not returned their cards for two consecutive months. The return rate for the WPSS is over 95%.8 We prospectively identified cases of active or latent TB from July 1996 to December 2003 using the WPSS and a monthly mailing to all chest physicians in Wales. The latter practice was discontinued in 1999 after reports of patients managed exclusively by chest physicians ceased. Participants were asked to report any patient less than 16 years of age newly diagnosed with active or latent TB.
Case definitions and data collection
Patients were classified as confirmed, probable, or possible active TB (disease) or latent TB (infection requiring chemoprophylaxis) on the basis of clinical, radiographic, and microbiological findings (see appendix). A positive tuberculin test was defined as induration of 5 mm or greater for a Mantoux test (0.1 ml of 1:1000 tuberculin PPD solution) or grade 2–4 reaction for a Heaf test.10 The tester was responsible for making the diagnosis. When the WPSS received a case report, the reporting doctor was sent a detailed postal questionnaire both to confirm diagnosis and to obtain further information about the case. This included questions on age, sex, ethnic origin, diagnostic category, specimens examined, chest x ray, tuberculin test results, site of disease, treatment details, BCG immunisation status, whether notified, and contact history.
Data analysis
Data were analysed by time, place, and person. We calculated incidence rates using 2001 population census denominators. Disease site was classified as pulmonary (lung), other respiratory (intra-thoracic lymph nodes, pleura), or non-respiratory. Treatment and chemoprophylaxis regimens were compared with British Thoracic Society guidelines.11,12 These recommend 6 months of treatment comprising rifampicin, isoniazid, pyrazinamide, and ethambutol for the initial 2 months followed by rifampicin and isoniazid for 4 months. Ethambutol may be omitted in patients unlikely to be isoniazid resistant (previously untreated white patients likely to be HIV negative and not contacts of a drug resistant case). Treatment with rifampicin and isoniazid should be extended to 12 months in patients with central nervous system involvement. Chemoprophylaxis should be either with isoniazid alone for 6 months or with rifampicin and isoniazid for 3 months. The programme was not submitted for ethics approval since at the time the study commenced, this was not required for public health surveillance schemes.
RESULTS
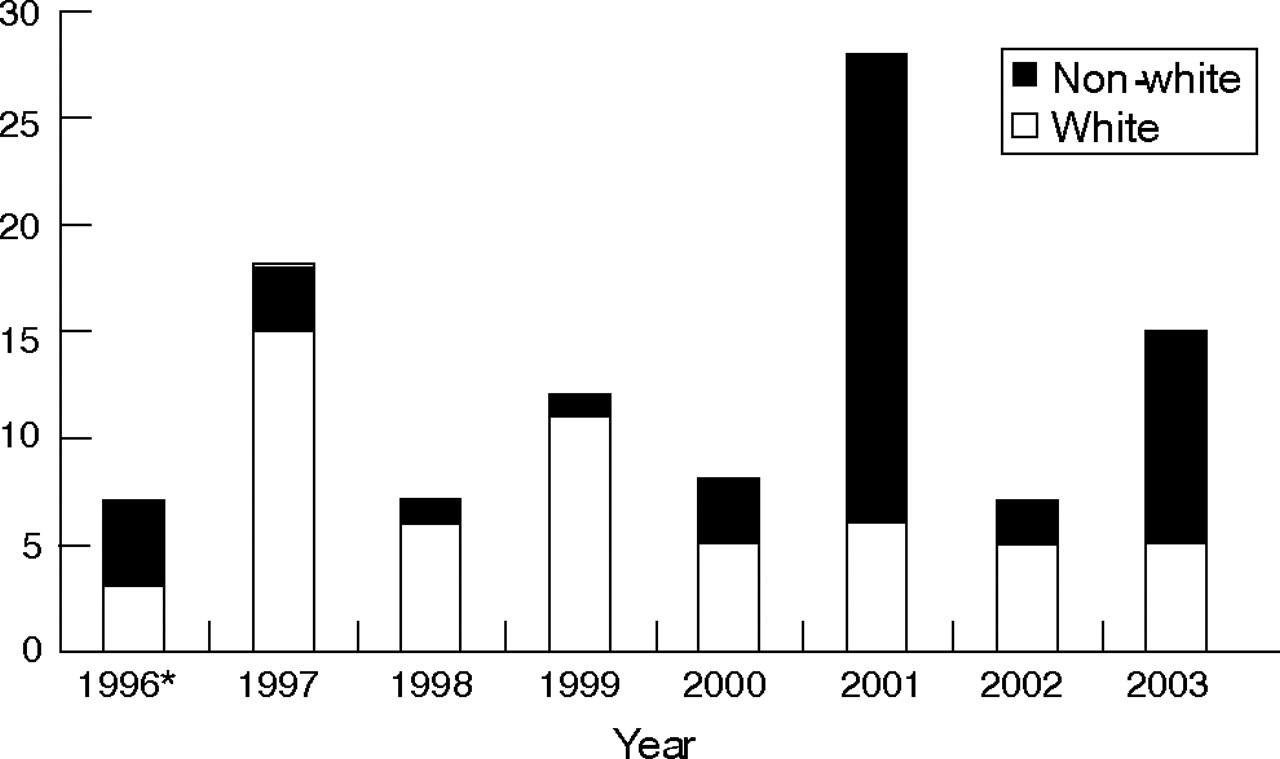
A total of 239 cases were reported. Seven reports were excluded because they were either duplicates or referred to opportunistic mycobacterial infection. The remaining 232 reports concerned 102 active TB cases (20 confirmed, 63 probable, 19 possible) and 130 latent TB cases. The mean annual incidence for active TB was 2.3 per 100 000 children, but numbers of cases varied considerably by year (fig 1). The mean annual number of reports of latent TB was 2.9 per 100 000. There were four outbreaks: a community outbreak in Pontypridd in 1997 involving adults and a small number of children infected through household contact, and three unlinked high school outbreaks in 2001. The schools were in Cardiff (two) and Newport (one). Each school had a high proportion of pupils from ethnic minority groups, and the TB cases occurred almost exclusively in non-white, male teenagers with extensive social contact outside school.

{kind=link}
Number of cases of tuberculosis in children by ethnic group, Wales, 1996–2003. *Part year.
Most active TB cases were in children aged 10–16 years, with one third aged 0–4 years, and one quarter aged 5–9 years (table 1).
Personal characteristics of cases of active and latent TB, Wales, 1996–2003
Non-white ethnic groups, mostly Pakistani or black African, accounted for 45% (46/102) of cases, increasing to 68% (34/50) during the last 3 years of the reporting period (fig 1). Twenty one (21%) patients were born outside the UK, mostly in Africa, particularly Somalia, reflecting the sizeable Somali communities in Cardiff and Newport. None were born in the Indian subcontinent (ISC). Of those born outside the UK, seven (33%) were diagnosed within a year of entry and 12 (57%) within 5 years. Only 10 cases travelled abroad in the 6 months before diagnosis, including six who had visited the ISC.
Clinical and diagnostic features
Pulmonary TB (47%, 48/102) was the most common presentation (table 2). White and non-white children had similar proportions of respiratory and peripheral lymph node disease. Ten patients had disseminated disease (seven with TB meningitis and three with miliary TB), including nine aged less than 10 years and eight white children. Most patients had a tuberculin test (60 Heaf only, 27 Mantoux only, six both), which was positive in 28/33 (85%) who had a Mantoux test and in 59/66 (89%) who had a Heaf test (table 3). Tuberculin strength used for the Mantoux test was occasionally not recorded.
Site of TB disease by ethnic group, Wales, 1996–2003
Site of TB disease and diagnostic findings, Wales, 1996–2003
Chest x ray was reported as abnormal in 75 cases, including 65 patients with respiratory TB, two with TB meningitis, three with miliary TB, and five with disease site reported as unknown. Only 20 patients had culture confirmed disease. Thirty children had at least one sputum sample submitted, including 21/48 (44%) children with pulmonary TB. Six children (20%) were positive on sputum microscopy (all pulmonary TB cases), and 12 (40%) were culture positive (10 pulmonary TB, one miliary TB, one intra-thoracic lymph node TB) (table 4).
Specimen type* and microbiology results for TB cases (n = 102)
Treatment
Most patients were managed by a paediatrician alone (74%, 75/102) or jointly with a chest physician (21%, 21/102). Data on treatment were available for 100 patients, of whom 86 received an appropriate drug combination. Almost all patients were treated for at least 6 months with rifampicin and isoniazid combined. During the initial treatment phase, 90 patients also received pyrazinamide and 45 patients received both pyrazinamide and ethambutol. Two patients were treated with rifampicin, isoniazid, and ethambutol (because of side effects with pyrazinamide) and one with rifampicin, pyrazinamide, and ethambutol (because of isoniazid resistance). However, eight patients received only rifampicin and isoniazid, and six non-white patients were treated with triple rather than quadruple therapy during the initial phase. Eleven patients were treated for too long (>6 months), but only three of seven patients with TB meningitis were treated for long enough (12 months). Supplemental pyridoxine was used in seven children. Two patients were reported to have multi-drug resistant TB and one child, a black African, was reported to be HIV positive.
Public health aspects
Neonatal BCG immunisation is recommended for children of immigrants from countries with a high prevalence of TB.10 In total, fewer than two thirds of eligible children (27/46, 59%) were known to have received BCG immunisation, although immunisation status was frequently not recorded (table 5). The proportion was highest among black African children (13/19, 68%) and ISC children (10/20, 50%), and in children aged 5–9 years (13/25, 52%). Of the 10 children with disseminated TB, only one (a Pakistani child) had been vaccinated with BCG. Most TB cases (75/102, 74%) were notified and this proportion did not differ by ethnic group or by age.
BCG immunisation, notification, and contact history for TB cases by age group, Wales, 1996–2003
Contact tracing identified a presumed source case for just over half of the patients, usually an adult member of the same household or a non-household adult family member. The source case was most likely to be an adult for children under 10 years of age (59%, 35/59), but for older children the source was as likely to be another child. In 43% (44/102) of patients, the source case was not identified, rising to 58% (25/43) of patients aged 10–16 years.
Latent TB
Of the 130 children with latent TB, 75 (58%) had a single positive tuberculin test, 26 (20%) had recent tuberculin conversion, six (5%) were close contacts aged under 2 years without BCG immunisation, and no further details were available for 23 (18%). Patients with latent TB were similar in sex, age distribution, and ethnicity to those with active TB, except for black African children (8% for latent TB v 19% for active TB) (table 1). One hundred and one patients (78%) received chemoprophylaxis with isoniazid and rifampicin, 26 (20%) with isoniazid alone (mostly children aged 0–4 years), and no details were available for three. Altogether, 104 (80%) patients received chemoprophylaxis for the recommended duration. Rifampicin with isoniazid was given for 3 months to 81/101 (80%) patients, but for over 3 months to 18 patients (including 15/18 who had a 6 month course) and for less than 3 months to two patients. Isoniazid alone was used for 6 months in 23/26 (88%) patients, but for a shorter duration in three.
DISCUSSION
The mean annual incidence of TB in Wales over the study period was 2.3 per 100 000 children, nearly double the incidence for 1986–1992,7 and higher than the incidence of 1.9 per 100 000 found by the National TB Survey in England and Wales in 1998.13 Overall, most cases of TB occurred in white children, although the proportion among non-white children increased substantially during the second half of the reporting period. The greatest increase was seen in black African children, followed by Pakistani children. Most black African children were born outside the UK in contrast to the Pakistani children, all of whom were UK born. No cases in black African children were identified in our previous study.7 This is similar to national trends in both children and adults, particularly in urban areas.13–15
Active surveillance methods are likely to have identified more cases than the retrospective data collection carried out for our previous study.7 However, the increased incidence is explained largely by three high school outbreaks during 2001 that affected older teenagers from non-white ethnic groups (black African in one outbreak and ISC in the other two).16 The peak in case numbers in 1997 was due partly to a community outbreak in a post-industrial community in the south Wales valleys affecting mostly white children from poorer socioeconomic backgrounds.17
Pulmonary disease accounted for 47% of cases of whom 29% had smear positive disease, all of whom were children over 10 years of age. However, no sputum samples were obtained in 56% of pulmonary TB patients. In some children where there is contact history with a positive index case, microbiological investigations may not be pursued in order to minimise the distress of nasogastric washout. Efforts to obtain samples for microbiological culture will assume increasing importance in future with the advent of routine molecular typing of TB isolates in Wales, since culture confirmation will not only be helpful for diagnosis but may also provide important epidemiological information on the source of infection. The proportion of pulmonary disease is similar to that found in the 1998 National TB Survey,13 but in our study there was no preponderance of non-respiratory disease in white children. In contrast, eight of 10 patients with disseminated TB were white children. BCG immunisation provides effective protection against disseminated TB,18 but since the UK offers selective neonatal BCG immunisation for high risk groups only, none had received BCG immunisation. The study also found that less than two thirds of non-white patients with active TB had been immunised, indicating a lost opportunity for prevention. BCG immunisation is not routinely monitored in the UK, unlike the remainder of the childhood immunisation programme, and several studies have shown sub-optimal uptake.19,20
Patient management conformed closely to British Thoracic Society guidelines,11 an improvement on previous findings.7 Most patients received an appropriate drug regimen and pyridoxine was used only rarely. However, some patients with active TB were treated with dual therapy only, and triple rather than quadruple therapy was used in the initial treatment phase for some non-white children. A fourth drug, usually ethambutol, is recommended in the latter situation because of the increased risk of isoniazid resistance. Several children were overtreated with unnecessarily prolonged chemotherapy or chemoprophylaxis courses. In contrast, patients with TB meningitis (who require a 12 month course) were mostly undertreated.
Although TB is a notifiable disease by law,12 only three quarters of cases were definitely notified. While this compares favourably with the 65% notified in our previous study,7 and with TB notification rates generally,6 it may nevertheless have led to delayed contact tracing or failure to identify an infectious source case. Contact tracing usually identified a household contact or an adult family member as the index case, although in older children the source was often another child. Older children were also more likely to be smear positive, a reminder that children can potentially cause extensive transmission.21,22 In a substantial minority of patients, an index case could not be identified.
The ratio of latent to active TB cases was 1.3:1, rather less than might be expected.23 This may be a consequence of incomplete reporting of latent TB to the scheme or, of greater concern, it may indicate incomplete contact tracing. Delayed notification of adult cases, incomplete contact investigations, and failure to document sputum conversion were all factors that led to preventable disease in one study of childhood TB.24 Without chemoprophylaxis, 40–50% of infants and around 15% of older children with infection go on to develop disease in 1–2 years.25 In the long term, chemoprophylaxis for infected children is as important as treating active cases in order to achieve TB elimination.24
What is already known on this topic
-
Most cases of tuberculosis in low incidence areas are in white children and pulmonary disease is the most common clinical presentation.
-
Chemotherapy is often sub-optimal and joint management of patients by a paediatrician and chest physician is recommended.
What this study adds
-
Cases of tuberculosis in black African children are rising even in low incidence areas, and may be associated with school outbreaks.
-
Problems remain with low uptake of BCG immunisation in high risk groups, undernotification of tuberculosis, failure to identify the index case, and excessive duration of chemotherapy or chemoprophylaxis.
Our study illustrates the changing epidemiology of TB. Wales has a relatively small ethnic minority population and a low incidence of TB. Most cases have historically occurred in the indigenous white population, but the proportion of cases in black African children is rising rapidly. Another striking feature is the different epidemiology in teenagers, reflected by differences in source and by TB outbreaks in high schools. Similar school outbreaks have been described elsewhere in the UK and emphasise the importance of maintaining effective services for TB prevention, treatment, and control.22,26 Effective TB surveillance in children remains a vital tool for monitoring the changing epidemiology of TB in the UK.
APPENDIX
CONFIRMED CASE
Culture confirmed disease, due to Mycobacterium tuberculosis complex infection (M tuberculosis, M bovis, M africanum).
PROBABLE CASE
In the absence of culture confirmation: (a) signs and/or symptoms compatible with tuberculosis, (b) treatment with two or more anti-tuberculous drugs, and (c) either microscopic/histological evidence of mycobacterial infection or positive tuberculin test result.
POSSIBLE CASE
In the absence of culture confirmation, microscopic/histological evidence of mycobacterial infection or positive tuberculin test result: (a) signs and/or symptoms compatible with tuberculosis and (b) treatment with two or more anti-tuberculous drugs.
TB CHEMOPROPHYLAXIS
Contacts with strongly positive Mantoux or Heaf test reactions but no clinical or radiological evidence of tuberculosis disease such as: (a) those under the age of 16 years who have had BCG immunisation and who have positive a Mantoux test greater than 5 mm or Heaf test grade 2–4, (b) those in whom recent tuberculin conversion has been noted, and (c) those under 2 years of age who are close contacts of smear positive cases and who have not had BCG immunisation, irrespective of their tuberculin status.
Acknowledgments
Several people were involved in making this surveillance study possible. We thank the WPSS team and all the clinicians who report to the scheme. We are also indebted to Hayley Phillips for providing administrative assistance, to TB specialist nurses Pat Stevens and Elizabeth Weeks for their contributions, and to paediatric sister Stella Young.
REFERENCES
Footnotes
-
Published Online First 31 May 2006
-
Competing interests: None declared.