The Impact of Anemia on Child Mortality: An Updated Review

Abstract
:1. Introduction
2. Experimental Section
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction Process
2.4. Analytic Procedures
3. Results
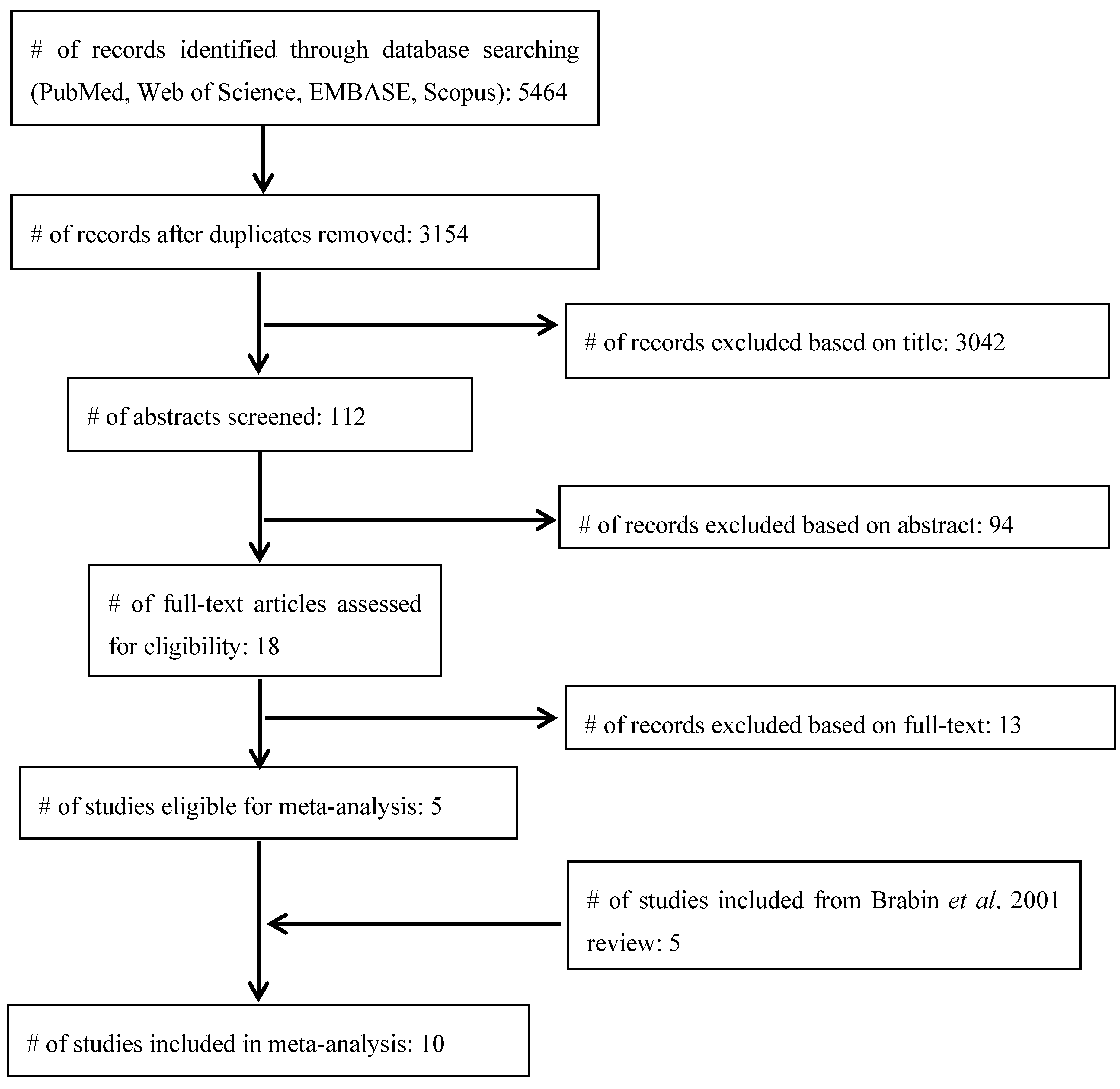
3.1. Article Search and Selection

3.2. Reasons for Exclusion
3.3. Studies Included

{kind=link}
{kind=link}
| Author, Year | Country | n a | Mean Age, Months | Study Design | Hb b (g/dL) | Hb Used for Analysis c (g/dL) | CFR, % (ndeaths/ntotal) | Relative Risk |
|---|---|---|---|---|---|---|---|---|
| Lackritz et al., 1992 [15] | Kenya | 2017 | 10 (median) | Cohort | 3.9–5.0 (not-transfused) | 5.0 | 13 (49/382) | 1.5 |
| 3.9–5.0 (transfused) | 5.0 | 10 (16/159) | 1.2 | |||||
| >5.0 | 8.5 | 8 (136/1,635) | 1.0 (Ref.) | |||||
| Lackritz et al., 1997 [16] | Kenya | 419 | 14 | Case-control | <5.0 (not-transfused) | 5.0 | 41 (48/116) | 2.1 |
| <5.0 (transfused) | 5.0 | 21 (40/187) | 1.1 | |||||
| ≥5.0 | 8.5 | 20 (59/303) | 1.0 (Ref.) | |||||
| Newton et al., 1997 [18] | Kenya | 1446 | 50 | Cohort | ≤5.0 (aparasitemic) | 5.0 | 9 (11/121) | 1.6 |
| >5.0 (aparasitemic) | 8.5 | 6 (74/1,325) | 1.0 (Ref.) | |||||
| ≤5.0 (parasitemic) | 5.0 | 8 (13/159) | 2.3 | |||||
| >5.0 (parasitemic) | 8.5 | 4 (26/735) | 1.0 (Ref) | |||||
| ≤5.0 (parasitemic with malaria) | 5.0 | 8 (11/141) | 2.3 | |||||
| >5.0 (parasitemic with malaria) | 8.5 | 3 (18/535) | 1.0 (Ref.) | |||||
| Mabeza et al., 1998 [24] | Zambia | 291 | 33 | Cohort | 6.0 (mean) | 6.0 | 18 (39/222) | 2.4 |
| 9.2 (mean) | 9.2 | 7 (5/69) | 1.0 (Ref.) | |||||
| Schellenberg et al., 1999 [25] | Tanzania | 2203 | 13 | Cohort | <5.0 | 5 | 6 (10/177) | 2.5 |
| 5.0–8.3 | 6.7 | 5 (8/164) | 1.6 | |||||
| >8.3 | 10.2 | 2 (28/1,239) | 1.0 (Ref.) | |||||
| Ghattas et al., 2003 [19] | Gambia | 777 | 28 day-15 year (mean not reported) | Case-control | <7.0 | 6.0 | 75 (36/48) d | 1.6 |
| 7.0–9.9 | 8.9 | 51 (161/318) d | 1.1 | |||||
| 10.0–10.9 | 10.5 | 46 (89/193) d | 1.0 | |||||
| 11.0–12.9 | 12.0 | 48 (105/218) d | 1.0 (Ref.) | |||||
| Reyburn et al., 2005 [20] | Tanzania | 2191 | 12 | Cohort | <5.0 | 5.0 | 8 (90/1,064) | 2.9 |
| 5.0–8.0 | 6.5 | 3 (33/1,127) | 1.0 (Ref.) | |||||
| Bachou et al., 2006 [21] | Uganda | 217 | 21 | Cohort | <5.0 | 5.0 | 29 (4/14) | 1.3 |
| ≥5.0 | 8.0 | 23 (46/203) | 1.0 (Ref.) | |||||
| Obonyo et al., 2007 [22] | Kenya | 1116 | 16 | Cohort | ≤5.0 | 5.0 | 12 (28/233) | 2.2 |
| >5.0 | 8.5 | 6 (49/883) | 1.0 (Ref.) | |||||
| Phiri et al., 2008 [23] | Malawi | 1134 | 23 | Case-control | 3.6 (mean) (all transfused) | 5.0 | 17 (65/377) | 13.1 |
| 9.6 (mean) | 9.6 | 3 (10/377) | 2 | |||||
| 9.9 (mean) | 9.9 | 1 (5/380) | 1.0 (Ref.) |
| Author, Year | Unique Exclusion Criteria | Sample Description | Comorbidities Present | % with Malaria | Specific Iron Measures | Anemia Etiology Described |
|---|---|---|---|---|---|---|
| Lackritz et al., 1992 [15] | None | Admitted to hospital from 1989–1990 a | Pneumonia (31%), gastroenteritis dehydration (4%), congestive heart failure (4%), sickle-cell (2%), marasmic kwashiorkor (2%) | 76 | No | No |
| Lackritz et al., 1997 [16] | None | Admitted to hospital in 1991 b | Respiratory illness (63%), malnutrition (22%), bacteremia (12%), HIV (8%) | 33 | No | No |
| Newton et al., 1997 [18] | None | (1) asymptomatic, from the community; (2) admitted to hospital for any cause; (3) admitted to hospital with severe anemia, from 1989–1991 a | Fever, GI bleeding, marasmus, sickle cell (10%) | 29 | Yes; plasma iron, Ft, TfR | Yes |
| Mabeza et al., 1998 [24] | Non-malarial causes of altered consciousness | With cerebral malaria, admitted to hospital from 1990–1994 b | Not described | 100 | No | No |
| Schellenberg et al., 1999 [25] | Abnormal CSF | With malaria, admitted to hospital from 1995–1996 a | Splenomegaly, hepatomegaly, hypoglycemia, vomiting, respiratory distress, dehydration | 100 | No | No |
| Ghattas et al., 2003 [19] | Deaths due to accidents | From community, attending regular well-child clinics at medical center from 1950–1997 b | Malnutrition, gastroenteritis, other infections | Not reported | No | No |
| Reyburn et al. 2005 [20] | Anemia due to malignancy or trauma | Admitted to hospital in 2002 with intention to treat for malaria b | Prostration, impaired consciousness, confusion, respiratory distress, jaundice | 47 | No | No |
| Bachou et al., 2006 [21] | None | Severely malnourished, admitted to hospital in 2003 a | Fluid overload, septicemia, pneumonia, tuberculous meningitis, hypothermia, hypoglycemia, hepatitis (1 case), cerebral malaria (1 case), measles (1 case) | 47 | No | No |
| Obonyo et al., 2007 [22] | None | Admitted to hospital in 2002 a | Pneumonia (29%), diarrhea (15%) | 83 | No | No |
| Phiri et al., 2008 [23] | Length <49 cm | Admitted to hospital for severe anemia (cases), other illness (hospital controls) or community of each case (community controls); 2002–2006 b | HIV (11%), edema, septicemia, pneumonia, tuberculous meningitis, drug reactions, hypothermia, hypoglycemia, hepatitis, cerebral malaria, measles | 41-59 | Yes; Ft, TfR | No |
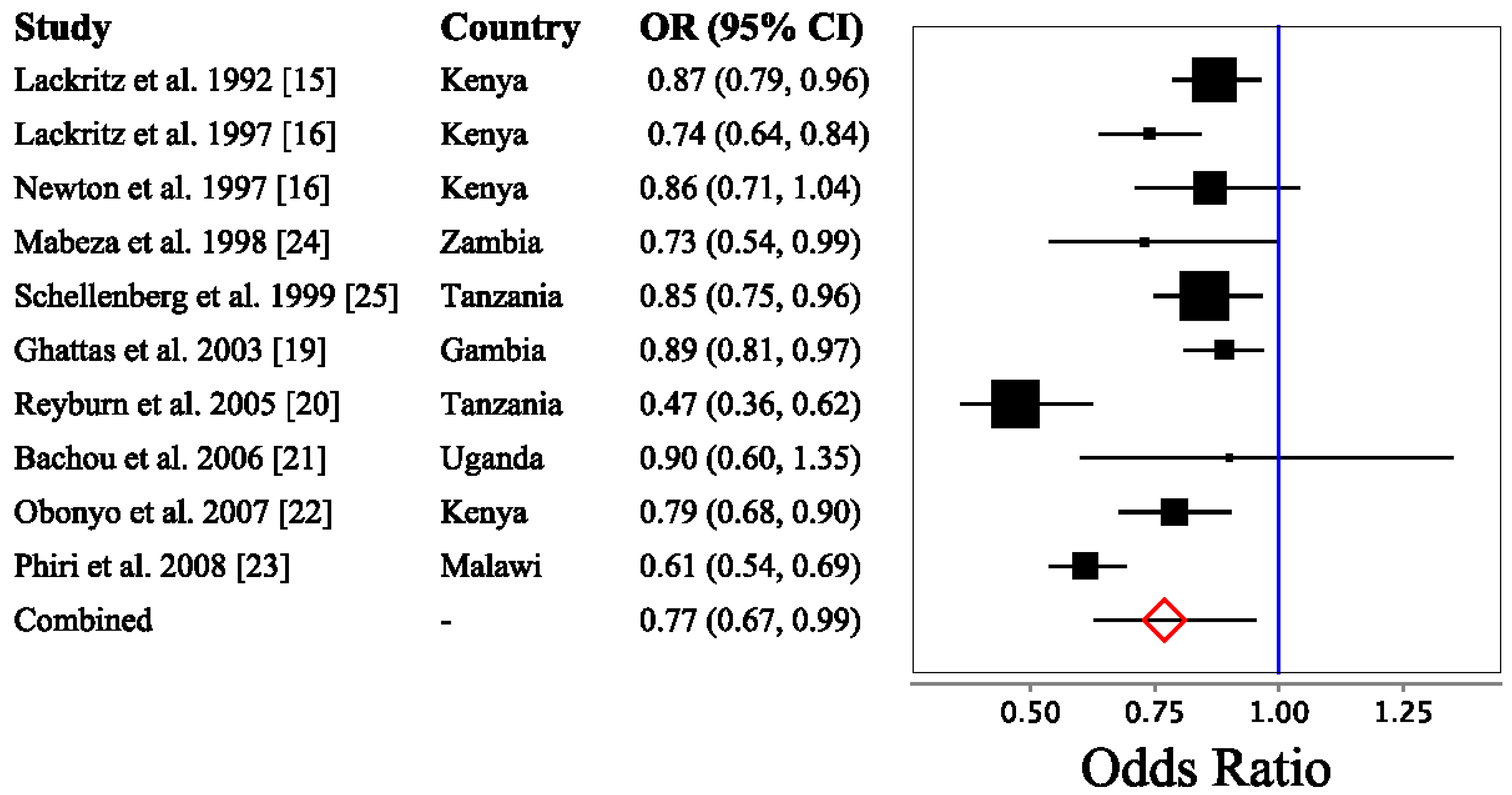
3.4. Logistic Regression Meta-Analysis

3.5. Sub-Analyses of the Effects of Study Quality, Transfusion and Malaria Parasitemia on the Relation between Hb and Mortality
4. Discussion
4.1. Main Finding and Implications
4.2. Iron Interventions in Malaria-Endemic Regions
4.3. Comparison with Other Studies
4.4. Strengths and Limitations
4.5. The Contribution of Malaria to Anemia-Related Child Mortality
4.6. Recommendations for Future Reports
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- WHO—World Health Statistics. 2013. Available online: http://www.who.int/gho/publications/world_health_statistics/2013/en/ (accessed on 30 January 2014).
- UN Millenium Development Goals Report; United Nations: New York, NY, USA, 2012.
- UN Inter-Agency Group for Child Mortality Estimation (IGME), Levels & Trends in Child Mortality; United Nations Children’s Fund: New York, NY, USA, 2013.
- Liu, L.; Johnson, H.L.; Cousens, S.; Perin, J.; Scott, S.; Lawn, J.E.; Rudan, I.; Campbell, H.; Cibulskis, R.; Li, M.; et al. Global, regional, and national causes of child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet 2012, 379, 2151–2161. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Jasrasaria, R.; Naghavi, M.; Wulf, S.K.; Johns, N.; Lozano, R.; Regan, M.; Weatherall, D.; Chou, D.P.; Eisele, T.P.; et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood 2014, 123, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Stoltzfus, R.J.; Mullany, L.; Black, R.E. Iron deficiency anaemia. In Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors; World Health Organization: Geneva, Switzerland, 2004; pp. 163–209. [Google Scholar]
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef] [PubMed]
- McLean, E.; Cogswell, M.; Egli, I.; Wojdyla, D.; de Benoist, B. Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993–2005. Public Health Nutr. 2009, 12, 444–454. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- WHO. Iron Deficiency Anaemia: Assessment, Prevention and Control. A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- De-Regil, L.M.; Jefferds, M.E.D.; Sylvetsky, A.C.; Dowswell, T. Intermittent iron supplementation for improving nutrition and development in children under 12 years of age. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Brabin, B.J.; Premji, Z.; Verhoeff, F. An Analysis of Anemia and Child Mortality. J. Nutr. 2001, 131, 636S–648S. [Google Scholar] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Health Research Institue: Ottawa, ON, Canada, 1999. [Google Scholar]
- Kuss, O. Paper 261-27. How to Use SAS for Logistic Regression with Correlated Data; SAS Users Group International: Cary, NC, USA, 2004. [Google Scholar]
- Lackritz, E.M.; Campbell, C.C.; Ruebush, T.K., II; Hightower, A.W.; Wakube, W.; Steketee, R.W.; Were, J.B. Effect of blood transfusion on survival among children in a Kenyan hospital. Lancet 1992, 340, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Lackritz, E.M.; Hightower, A.W.; Zucker, J.R.; Ruebush, T.K., II; Onudi, C.O.; Steketee, R.W.; Were, J.B.; Patrick, E.; Campbell, C.C. Longitudinal evaluation of severely anemic children in Kenya: The effect of transfusion on mortality and hematologic recovery. AIDS 1997, 11, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Brick, T.; Peters, M.J. Risks and benefits of transfusion for children with severe anemia in Africa. BMC Med. 2014, 12, 68. [Google Scholar] [CrossRef] [PubMed]
- Newton, C.R.; Warn, P.A.; Winstanley, P.A.; Peshu, N.; Snow, R.W.; Pasvol, G.; Marsh, K. Severe anaemia in children living in a malaria endemic area of Kenya. Trop. Med. Int. Health 1997, 2, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Ghattas, H.; Fulford, T.; Prentice, A. Effect of moderate anaemia on later mortality in rural African children. Lancet 2003, 361, 2048–2050. [Google Scholar] [CrossRef] [PubMed]
- Reyburn, H.; Mbatia, R.; Drakeley, C.; Bruce, J.; Carneiro, I.; Olomi, R.; Cox, J.; Nkya, W.M.M.M.; Lemnge, M.; Greenwood, B.M.; et al. Association of transmission intensity and age with clinical manifestations and case fatality of severe Plasmodium falciparum malaria. JAMA 2005, 293, 1461–1470. [Google Scholar] [CrossRef] [PubMed]
- Bachou, H.; Tumwine, J.K.; Mwadime, R.K.N.; Tylleskär, T. Risk factors in hospital deaths in severely malnourished children in Kampala, Uganda. BMC Pediatr. 2006, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Obonyo, C.O.; Vulule, J.; Akhwale, W.S.; Grobbee, D.E. In-Hospital morbidity and mortality due to severe malarial anemia in western Kenya. Am. J. Trop. Med. Hyg. 2007, 77, 23–28. [Google Scholar] [PubMed]
- Phiri, K.S.; Calis, J.C.J.; Faragher, B.; Nkhoma, E.; Ng’oma, K.; Mangochi, B.; Molyneux, M.E.; van Hensbroek, M.B. Long Term Outcome of Severe Anaemia in Malawian Children. PLoS One 2008, 3. [Google Scholar] [CrossRef] [PubMed]
- Mabeza, G.F.; Biemba, G.; Brennan, A.G.; Moyo, V.M.; Thuma, P.E.; Gordeuk, V.R. The association of pallor with haemoglobin concentration and mortality in severe malaria. Ann. Trop Med. Parasitol. 1998, 92, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Schellenberg, D.; Menendez, C.; Kahigwa, E.; Font, F.; Galindo, C.; Acosta, C.; Schellenberg, J.A.; Aponte, J.J.; Kimario, J.; Urassa, H.; et al. African children with malaria in an area of intense Plasmodium falciparum transmission: features on admission to the hospital and risk factors for death. Am. J. Trop. Med. Hyg. 1999, 61, 431–438. [Google Scholar] [PubMed]
- Villamor, E.; Misegades, L.; Fataki, M.R.; Mbise, R.L.; Fawzi, W.W. Child mortality in relation to HIV infection, nutritional status, and socio-economic background. Int. J. Epidemiol. 2005, 34, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Kalanda, B.; Verhoeff, F.; le Cessie, S.; Brabin, J. Low birth weight and fetal anaemia as risk factors for infant morbidity in rural Malawi. Malawi Med. J. 2009, 21, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Zucker, J.R.; Lackritz, E.M.; Ruebush, T.K., II; Hightower, A.W.; Adungosi, J.E.; Were, J.B.; Metchock, B.; Patrick, E.; Campbell, C.C. Childhood mortality during and after hospitalization in western Kenya: Effect of malaria treatment regimens. Am. J. Trop. Med. Hyg. 1996, 55, 655–660. [Google Scholar] [PubMed]
- Commey, J.O.O.; DeKyem, P. Childhood deaths from anaemia in Accra, Ghana. West Afr. Med. J. 1995, 14, 101–104. [Google Scholar]
- Allen, S.J.; O’Donnell, A.; Alexander, N.D.; Clegg, J.B. Severe malaria in children in Papua New Guinea. QJM 1996, 89, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Marsh, K.; Forster, D.; Waruiru, C.; Mwangi, I.; Winstanley, M.; Marsh, V.; Newton, C.; Winstanley, P.; Warn, P.; Peshu, N. Indicators of life-threatening malaria in African children. N. Engl. J. Med. 1995, 332, 1399–1404. [Google Scholar] [CrossRef] [PubMed]
- Holzer, B.R.; Egger, M.; Teuscher, T.; Koch, S.; Mboya, D.M.; Smith, G.D. Childhood anemia in Africa: To transfuse or not transfuse? Acta Trop. 1993, 55, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Van den Hombergh, J.; Dalderop, E.; Smit, Y. Does iron therapy benefit children with severe malaria-associated anaemia? A clinical trial with 12 weeks supplementation of oral iron in young children from the Turiani Division, Tanzania. J. Trop. Pediatr. 1996, 42, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Slutsker, L.; Taylor, T.E.; Wirima, J.J.; Steketee, R.W. In-Hospital morbidity and mortality due to malaria-associated severe anaemia in two areas of Malawi with different patterns of malaria infection. Trans. R. Soc. Trop. Med. Hyg. 1994, 88, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Bojang, K.A.; van Hensbroek, M.B.; Palmer, A.; Banya, W.A.; Jaffar, S.; Greenwood, B.M. Predictors of mortality in Gambian children with severe malaria anaemia. Ann. Trop Paediatr. 1997, 17, 355–359. [Google Scholar] [PubMed]
- WHO Guidelines for the Use of Iron Supplements to Prevent and Treat Iron Deficiency Anemia. Available online: http://www.who.int/nutrition/publications/micronutrients/anaemia_iron_deficiency/1-57881-020-5/en/ (accessed on 14 July 2014).
- International Nutritional Anemia Consultative Group (INACG). Safety of Iron Supplementation Programs in Malaria-Endemic Regions; International Life Sciences Institute: Washington, DC, USA, 1999. [Google Scholar]
- Sazawal, S.; Black, R.E.; Ramsan, M.; Chwaya, H.M.; Stoltzfus, R.J.; Dutta, A.; Dhingra, U.; Kabole, I.; Deb, S.; Othman, M.K.; et al. Effects of routine prophylactic supplementation with iron and folic acid on admission to hospital and mortality in preschool children in a high malaria transmission setting: Community-based, randomised, placebo-controlled trial. Lancet 2006, 367, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Gera, T.; Sachdev, H.P.S.; Nestel, P.; Sachdev, S.S. Effect of iron supplementation on haemoglobin response in children: Systematic review of randomised controlled trials. J. Pediatr. Gastroenterol. Nutr. 2007, 44, 468–486. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. UNICEF Iron Supplementation of Young Children in Regions Where Malaria Transmission Is Intense and Infectious Disease Highly Prevalent; WHO: New York, NY, USA, 2006. [Google Scholar]
- Zlotkin, S.; Newton, S.; Aimone, A.M.; Azindow, I.; Amenga-Etego, S.; Tchum, K.; Mahama, E.; Thorpe, K.E.; Owusu-Agyei, S. Effect of iron fortification on malaria incidence in infants and young children in Ghana: A randomized trial. JAMA 2013, 310, 938–947. [Google Scholar] [CrossRef] [PubMed]
- Calis, J.C.J.; Phiri, K.S.; Faragher, E.B.; Brabin, B.J.; Bates, I.; Cuevas, L.E.; de Haan, R.J.; Phiri, A.I.; Malange, P.; Khoka, M.; et al. Severe anemia in Malawian children. N. Engl. J. Med. 2008, 358, 888–899. [Google Scholar] [CrossRef] [PubMed]
- Boele van Hensbroek, M.; Calis, J.C.J.; Phiri, K.S.; Vet, R.; Munthali, F.; Kraaijenhagen, R.; van den Berg, H.; Faragher, B.; Bates, I.; Molyneux, M.E. Pathophysiological mechanisms of severe anaemia in Malawian children. PLoS One 2010, 5, e12589. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.-S.; Kuo, H.-C.; Wu, C.-C.; Yu, H.-R.; Wang, L.; Chang, H.-W.; Yang, K.D. Risk factors for mortality of pediatric patients without underlying diseases. Pediatr. Neonatol. 2011, 52, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Sutcliffe, C.G.; Scott, S.; Mugala, N.; Ndhlovu, Z.; Monze, M.; Quinn, T.C.; Cousens, S.; Griffin, D.E.; Moss, W.J. Survival from 9 Months of Age among HIV-Infected and Uninfected Zambian Children Prior to the Availability of Antiretroviral Therapy. Clin. Infect. Dis. 2008, 47, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Bloch, E.M.; Vermeulen, M.; Murphy, E. Blood transfusion safety in Africa: A literature review of infectious disease and organizational challenges. Transfus. Med. Rev. 2012, 26, 164–180. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.L.; Murray-Kolb, L.E.; Rosales, F.J.; Solomons, N.W.; Angelilli, M.L. Interpretation of serum ferritin concentrations as indicators of total-body iron stores in survey populations: The role of biomarkers for the acute phase response. Am. J. Clin. Nutr. 2006, 84, 1498–1505. [Google Scholar] [PubMed]
- Christofides, A.; Asante, K.P.; Schauer, C.; Sharieff, W.; Owusu-Agyei, S.; Zlotkin, S. Multi-micronutrient Sprinkles including a low dose of iron provided as microencapsulated ferrous fumarate improves haematologic indices in anaemic children: A randomized clinical trial. Matern. Child. Nutr. 2006, 2, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Schümann, K.; Solomons, N.W. Can iron supplementation be reconciled with benefits and risks in areas hyperendemic for malaria? Food Nutr. Bull. 2013, 34, 349–356. [Google Scholar] [PubMed]
- Brabin, L.; Brabin, B.J.; Gies, S. Influence of iron status on risk of maternal or neonatal infection and on neonatal mortality with an emphasis on developing countries. Nutr. Rev. 2013, 71, 528–540. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scott, S.P.; Chen-Edinboro, L.P.; Caulfield, L.E.; Murray-Kolb, L.E. The Impact of Anemia on Child Mortality: An Updated Review. Nutrients 2014, 6, 5915-5932. https://doi.org/10.3390/nu6125915
Scott SP, Chen-Edinboro LP, Caulfield LE, Murray-Kolb LE. The Impact of Anemia on Child Mortality: An Updated Review. Nutrients. 2014; 6(12):5915-5932. https://doi.org/10.3390/nu6125915
Chicago/Turabian StyleScott, Samuel P., Lenis P. Chen-Edinboro, Laura E. Caulfield, and Laura E. Murray-Kolb. 2014. "The Impact of Anemia on Child Mortality: An Updated Review" Nutrients 6, no. 12: 5915-5932. https://doi.org/10.3390/nu6125915