




Abstract
Peer support may improve self-management among the millions of people with diabetes around the world. A major challenge to international promotion of peer support is allowing for tailoring to population, cultural, health system and other features of specific settings, while also ensuring congruence with standards for what peer support entails. One strategy to address this challenge was used in the Robert Wood Johnson Foundation Diabetes Initiative. Key functions of self-management—Resources and Supports for Self-Management—were identified. Individual programmes were then encouraged to implement these resources and support in ways that were feasible in their settings and responsive to the needs and perspectives of those they serve. Extending this to peer support, three Key functions are (i) assistance in managing and living with diabetes in daily life; (ii) social and emotional support and (iii) linkage to clinical care. International promotion may be advanced by emphasizing these key functions and then encouraging local variation in the specific ways they are addressed. Similarly, evaluation of the general benefits of peer support across several individual programmes may rest on measurement of implementation of the key functions, participants' reports of receipt of them and common end points. Challenges to promoting peer support include integrating peers amidst others in the health care system, harmonizing peers with family and other social networks, maintaining the engagement of peer supporters and those they assist and preventing training, quality improvement and professionalism from distorting the fundamental benefits of support from a peer.
Introduction
Peer support through lay health workers, community health workers and similar interventions has been a widely utilized approach to health promotion.1–7 Within diabetes management, a recent review recognized that current evidence is limited but noted positive effects in terms of improved self-management behaviours and indicators of clinical status8 while a World Health Organization consultation and report laid out the rationale and evidence for peer support in diabetes and identified important directions for research and programme development.9 A recent systematic review found mixed support for peer interventions in a variety of areas.10 The future should see increased evidence regarding peer support in diabetes from several ongoing studies.11–13
In addition to research supporting its importance,14,15 diabetes self-management education has been grounded in identification of key self-management behaviours such as the American Association of Diabetes Educators’ AADE 7 Self-Care Behaviors’™ (http://www.diabeteseducator.org/ProfessionalResources/AADE7/) and an ‘International Curriculum for Diabetes Health Professional Education’ developed by the International Diabetes Federation (http://www.idf.org/home/index.cfm?node=503). Established guidelines16 have identified the importance of ongoing support in diabetes management: ‘Ongoing support is critical to sustain progress made by participants’ through diabetes self-management programmes.
Peer support may be an especially helpful way to provide the ongoing support for which guidelines call.9 Applying management plans in daily life may benefit from discussion with a peer who has first-hand knowledge of the circumstances of one's daily life.17 That diabetes management entails efforts sustained over decades suggests the pertinence of encouragement from someone perceived as understanding ones perspectives and who has the time to develop a supportive relationship.18 Peer support may also facilitate regular attendance at clinical care or facilitate obtaining answers to questions that emerge in daily management.
The emerging worldwide burden of diabetes raises the issue of how peer support might be promoted internationally. However, the ways in which varied health care systems as well as cultural and population factors shape peer support provide a number of challenges to international promotion. Social and cultural factors may exert substantial influence on how peer support is delivered and received. The roles of peers versus paraprofessionals and professionals may vary considerably in different countries. Thus programme models must be flexible so they can be tailored to widely varying settings, populations and social, cultural, organizational and economic contexts. At the same time, international promotion of peer support would require some level of consistency or standardization across cultures and settings in order to clarify what is the peer support being promoted.
Functional definition of key components
The challenge of defining interventions sufficiently to make them meaningful and, at the same time, allowing flexibility and tailoring to local conditions was also faced by the Diabetes Initiative of the Robert Wood Johnson Foundation. To show that self-management programmes can be effective in ‘real-world’ settings, its 14 grantee sites represented very different settings and served very different populations.19 Thus, it faced the challenge of melding (i) sufficient standardization so that there is a clear programme being evaluated, with (ii) provision of sufficient flexibility for local tailoring. It solved this problem by defining self-management in broad functional terms and then encouraging each site to be inventive in its approach to these functions. The broad functional terms were called ‘Resources and Supports for Self-Management’.20 Each site of the Diabetes Initiative was encouraged to address these in ways that made sense for its organizational strengths, population characteristics and settings. The six Resources and Supports for Self-Management and examples of how they were implemented are as follows.
Individualized assessment
Self-management is based on individualized appraisal of diabetes management as well as assessment of skills for self-management, pertinent family, social and cultural perspectives, etc. All the sites of the Diabetes Initiative emphasized this such as in programmes based on the Transtheoretical Model of individuals’ stages of behaviour change.21,22
Collaborative goal setting
Individuals need to be involved in setting goals for their self-management to enhance their commitment to those goals and their pertinence to their daily lives.23,24 Examples include staff training on goal setting25 and reorganizing primary care encounters to provide time for doctor–patient assessment and goal setting for self-management.26
Skills
As articulated in the AADE 7 Self-Care Behaviors™, individuals need diabetes-specific skills (e.g. monitoring, taking medication) and more general skills (e.g. healthy eating, being active, problem solving, reducing risks and healthy coping27). These were emphasized in all the sites through a variety of approaches, including individual education by professionals or community health workers, group self-management programmes,28–30 diabetes self-management classes or a variety of approaches to dealing with depression in diabetes self-management.31
Ongoing follow-up and support
Given that diabetes is for ‘the rest of your life’,18 the tasks of self-management do not end when, e.g., when a 10% weight loss is achieved, but extend for decades. Thus, programmes need to reach and sustain contact with individuals to provide ongoing support for good diabetes management. Approaches varied widely and included training medical assistants to provide follow-up and support, a ‘breakfast club’,32 group medical visits,33,34 promotoras and community health workers or a 10-session, biweekly support group led by promotores for those who had completed a self-management course.35 A culturally specific approach to implementing a support group was a ‘talking circle’ of those with diabetes and others in an American Indian community.
Community resources
Peer- and community-based approaches promoted physical activity and healthy eating among those with diabetes.36 Clinic–community partnerships arranged for indoor walking spaces for physical activity, developed restaurant competitions to encourage diabetes-friendly menu items, advocated for healthy snacks in worksite vending machines and placed diabetes education materials in public libraries.37
Ongoing, quality clinical care
This includes integrating self-management with clinical care, such as in the development of a linkage between a community-based promotora programme and resources of a local health centre, training nurses in goal setting and including a clinical psychologist as part of the diabetes care team,25 tools for measuring organizational capacity for self-management38 and group medical visits.33,34
Sponsored by the US National Institute of Mental Health,39 ‘NIMH Project Accept’, a multi-site study of community-based HIV voluntary counseling and testing (VCT) provides another example of identifying key functions of interventions and facilitating local variation in their implementation. This community randomized trial is being implemented in 34 communities in South Africa, Tanzania and Zimbabwe and 14 communities in Thailand. Planning and conceptualization of the study centred on identifying three key strategies around which to base the intervention. These are viewed as applicable to changing community norms and to reducing risk for HIV infection among all community members, irrespective of whether they participated directly in the intervention. The three key characteristics are as follows: (i) increase access to HIV VCT in community settings through free testing and mobile vans or temporary units in community sites such as market places; (ii) engage the community through outreach and (iii) provide HIV post-test support.
With identification of the three core characteristics identified, variation in culture, demography, geography and the epidemiology of the HIV epidemic across the sites has led to tailoring the intervention to meet local needs and take advantage of local resources and strengths. For the purpose of the community randomized evaluation design, the sites had to standardize the intervention dose provided for each key strategy. However, the ways in which each intervention component was implemented across the different sites varied. For example, with regard to increasing community access to HIV counselling and testing, some sites such as Soweto, Johannesburg adopted the approach of mobile caravans that travelled throughout the community and provided services at designated locations. In contrast, mobile caravans in communities around Chiang Mai in Thailand would be impractical given the local topography. Thus, the team in Thailand used existing community facilities such as community clinics to provide counselling and testing services.
Tailoring to characteristics of different sites also occurred with the key strategy of community mobilization activities. In Kisarawe, Tanzania, there was no previous HIV counselling and testing available in the communities prior to NIMH Project Accept. Thus, this site had to engage in extensive preparatory work in the communities to provide basic information about HIV counselling and testing services. Local volunteers connected to the project were organized to spread information about the services to remote areas of the communities. In contrast, communities in the South African sites had previous exposure to counselling and testing. There, NIMH Project Accept mobilized to increase demand for services by working through traditional chiefs, partnering with pastors and door-to-door and street level mobilization. With this difference in local operational detail, however, community mobilization remained a key component of NIMH Project Accept in each community.
Support for defining intervention by key functions
There are no magic bullets in health promotion. In diabetes management, for example, meta-analyses of self-management programmes conducted by Norris et al. found that the only predictor of success was not any particular programme feature or content, but duration of contact.14,15 The prediction of benefit by length and variety of treatment has also been observed in meta-analyses of smoking cessation interventions40,41 and of a variety of prevention and patient education programmes.42 ‘Self–management’ is dependent on the contexts that surround the individual. This point was put best, perhaps, by Kottke et al. in a major review of the smoking cessation literature in 1988:41
Success was not associated with novel or unusual interventions. It was the product of personalized smoking cessation advice and assistance, repeated in different forms by several sources over the longest feasible period.
… program(s) will probably be most fruitful if focused on how the nonsmoking message can be given clearly, repeatedly, and consistently through every feasible delivery system; personalized advice; printed materials; the mass media; and smoke-free medical, work, school, and home environments. (p. 2882–2889)
The importance of duration of support is also reflected in analysis of smoking cessation from the perspective of behavioural economics.43,44 Some research on social support reflects an implicit model that, were it ‘truly’ effective, the benefits of social support should carry over after the termination of support. The literature does not support this.45 Just as with most interventions, when social support is withdrawn, it shows little sustained impact. (Note parallel: chronic disease requires chronic care.) That benefits are limited to the time it is available suggests that one way in which social support is helpful is by facilitating choices of healthy alternatives. In the case of smoking, the observation that social support is enjoyable, anxiolytic and mood elevating suggests that it may compete with the attraction of nicotine. While support is in place, choices for nicotine are reduced; when the support is withdrawn, the prominence of nicotine is left unopposed. Indeed, social support tends to be a very effective influence on behaviour while it is available. One application of this economic perspective is that what counts in support is its attractiveness and availability more than the credentials of the provider.
That varied, sustained, attractive and available supports are important for maintaining health behaviours has important implications for international promotion of peer support. People with diabetes face the challenge of ongoing diabetes management for 20, 30 or 40+ years of their lives. In supporting and encouraging ongoing management (as opposed to clinical identification of best treatment regimens), what counts most is probably not any single critical ingredient of peer-based support, but the availability and attractiveness of the support, the acceptability of the supporter to the recipient, the time available to get to know and support each other and the common experience of provider and recipient to facilitate collaborative problem solving in adapting diabetes management plans to everyday life.
All of this supports a major rationale behind the value of peer support. As diabetes is ‘for the rest of you life’,18 the development of supportive peer dyads and networks has the opportunity to provide ongoing support indefinitely.
Equifinality
Imagine a health care planner eager to learn about self-management attending a convention of professionals in the field. In symposia, paper sessions, and casual conversations, the planner hears a variety of messages that a particular chronic disease self-management programme has substantial outcome data to support it, that motivational interviewing is the secret for helping people get started in acting to improve their health, that the Transtheoretical Model is the way to develop programmes that address individuals’ readiness for change, that the doctor–patient relationship and goal setting within the medical encounter are critical, that the diabetes educator is central, that nothing will be sustained without social support, that communities and worksites may be critical settings for improving self-management and on and on. We may easily imagine our planner beginning to think that the pharmaceutical formulary looks simple!
The principal of equifinality in organizational behaviour provides a solution for the confused planner. The adoption of interest-bearing checking accounts by a group of banks in St Louis, MO, illustrates this principle.46 Following a state law that first made such accounts legal, each bank made interest bearing accounts available for its customers, but did so in very different ways. This demonstrates equifinality that there are multiple effective approaches to reaching similar ends. Moreover, what is often critical is not the variation in operational detail but the common end or function operations achieve.
The Resources and Supports for Self-Management reflect equifinality in focusing on functional commonalities, not on differences in procedural details. Thus, for example, tailoring of goal setting to the individual may be accomplished by motivational interviewing,47 an intervention based on the Transtheoretical Model,48 or an interactive e-health resource.49 What counts is not which of these is marginally more effective than the others in a university-based research trial, but that the one chosen is generally effective, is feasible in the setting in which it is to be used and is pertinent and acceptable to the population for which it is intended.
Promoting models of peer support with regional and local variation
Table 1 outlines three Key functions of peer support: (i) assistance in managing and living with diabetes in daily life; (ii) social and emotional support and (iii) linkage to clinical care. As indicated in the table, each Key function could be elaborated with a variety of specific approaches to fulfilling it. Thus, under the Key function of social and emotional support, peers may contact each other through phone, face-to-face visits, web or e-mail technology, joint participation in activities such as exercise clubs or support groups, etc. What is critical is that they ‘do’ contact each other! These modes of contact may vary tremendously around the world but, through this variety, frequent contact and the key function of social and emotional support are served. So too the other Key functions listed in Table 1 could be pursued in varied ways but in their aggregate would define peer support operationally.
Key functions of peer support for diabetes management
| Behavioural objectives | Specific operational approaches to behavioural objectives | Outcome/measurement |
| Key function: assistance in managing and living with diabetes in daily life | ||
| Assist problem solving to support regimen adherence in daily life | • Use problem-solving intervention techniques • Share stories of challenges and successes • Assist in changing routines or other adjustments to facilitate adherence | • Audits of topics covered • Participant reports of types interactions addressing problem solving • Participant reports of management tasks addressed |
| Engage in healthy eating, physical activity together | • Share regular modest physical activity (e.g. walking, swimming, tennis, others) ○ Share in healthy eating behaviours (e.g. shop for food, prepare meals, and/or eat meals together) | • Participant reports of shared activities ○ Physical activity ○ Health eating ○ Others |
| Key function: social and emotional support | ||
| Maintain frequent contact | • Face-to-face contact • Telephone contact • Electronic contact (web, e-mail, text message) | • Contact records or reports |
| Encourage, enhance motivation | • Point out progress • Reassure of long-term nature of diabetes management • Reassure that medical care and medications can help • Reassure that one is ‘doing your best’ | • Audits of topics covered • Participant reports of support received/provided using standard measures |
| Provide support in dealing with day-to-day stressors | • Use problem-solving intervention techniques • Share stories of challenges and successes • Be available to listen and discuss problems | • Audits of topics covered • Participant reports of types interactions addressing problem solving |
| Tailoring of support to regional and cultural practices and settings | • Consideration of national, regional and cultural differences in social support, preferences for types and styles of social support • Providing support that is tuned to individual, social and cultural features | • Interviews with program staff and peers to characterize key features of support within their settings and cultures • Participant ratings of their satisfaction with peer support provided and the extent to which support is easily accepted |
| Advocate for and represent those with diabetes | • Serve on advisory committees • Encourage individuals and groups to assert their needs with health providers, community organizations | • Program documentation of ○ Committee and advisory roles ○ Advocacy activities |
| Ethical considerations | • Consideration of individual rights, privacy and limits on roles of peer support within the contexts of different countries, cultures and settings | • Documentation of ethical issues emergent through individual projects • Participant ratings of being treated with consideration for their rights, privacy, etc. |
| Key function: linkage to clinical care | ||
| Develop and maintain linkages care providers | • Organize peer support within primary care or other principal source of clinical care • Maintain active linkages with providers of primary and clinical care such as by referral, meetings to discuss key issues, training, etc. | • Characterization of linkages with primary care and systems of care • Audits of key interactions (e.g. # referrals to peer support, training of peer supporters) between support and care providers • Participant ratings of extent to which peer support is connected to sources of care |
| Encourage regular clinical care, partnership with clinical providers | • Remind each other of times for regular physician visits • Encourage physician visits when circumstances or symptoms warrant • Coordination with clinical practices and guidelines within country and setting | • Audits of topics covered • Participant reports of regular, out-patient clinical care |
| Behavioural objectives | Specific operational approaches to behavioural objectives | Outcome/measurement |
| Key function: assistance in managing and living with diabetes in daily life | ||
| Assist problem solving to support regimen adherence in daily life | • Use problem-solving intervention techniques • Share stories of challenges and successes • Assist in changing routines or other adjustments to facilitate adherence | • Audits of topics covered • Participant reports of types interactions addressing problem solving • Participant reports of management tasks addressed |
| Engage in healthy eating, physical activity together | • Share regular modest physical activity (e.g. walking, swimming, tennis, others) ○ Share in healthy eating behaviours (e.g. shop for food, prepare meals, and/or eat meals together) | • Participant reports of shared activities ○ Physical activity ○ Health eating ○ Others |
| Key function: social and emotional support | ||
| Maintain frequent contact | • Face-to-face contact • Telephone contact • Electronic contact (web, e-mail, text message) | • Contact records or reports |
| Encourage, enhance motivation | • Point out progress • Reassure of long-term nature of diabetes management • Reassure that medical care and medications can help • Reassure that one is ‘doing your best’ | • Audits of topics covered • Participant reports of support received/provided using standard measures |
| Provide support in dealing with day-to-day stressors | • Use problem-solving intervention techniques • Share stories of challenges and successes • Be available to listen and discuss problems | • Audits of topics covered • Participant reports of types interactions addressing problem solving |
| Tailoring of support to regional and cultural practices and settings | • Consideration of national, regional and cultural differences in social support, preferences for types and styles of social support • Providing support that is tuned to individual, social and cultural features | • Interviews with program staff and peers to characterize key features of support within their settings and cultures • Participant ratings of their satisfaction with peer support provided and the extent to which support is easily accepted |
| Advocate for and represent those with diabetes | • Serve on advisory committees • Encourage individuals and groups to assert their needs with health providers, community organizations | • Program documentation of ○ Committee and advisory roles ○ Advocacy activities |
| Ethical considerations | • Consideration of individual rights, privacy and limits on roles of peer support within the contexts of different countries, cultures and settings | • Documentation of ethical issues emergent through individual projects • Participant ratings of being treated with consideration for their rights, privacy, etc. |
| Key function: linkage to clinical care | ||
| Develop and maintain linkages care providers | • Organize peer support within primary care or other principal source of clinical care • Maintain active linkages with providers of primary and clinical care such as by referral, meetings to discuss key issues, training, etc. | • Characterization of linkages with primary care and systems of care • Audits of key interactions (e.g. # referrals to peer support, training of peer supporters) between support and care providers • Participant ratings of extent to which peer support is connected to sources of care |
| Encourage regular clinical care, partnership with clinical providers | • Remind each other of times for regular physician visits • Encourage physician visits when circumstances or symptoms warrant • Coordination with clinical practices and guidelines within country and setting | • Audits of topics covered • Participant reports of regular, out-patient clinical care |
Key functions of peer support for diabetes management
| Behavioural objectives | Specific operational approaches to behavioural objectives | Outcome/measurement |
| Key function: assistance in managing and living with diabetes in daily life | ||
| Assist problem solving to support regimen adherence in daily life | • Use problem-solving intervention techniques • Share stories of challenges and successes • Assist in changing routines or other adjustments to facilitate adherence | • Audits of topics covered • Participant reports of types interactions addressing problem solving • Participant reports of management tasks addressed |
| Engage in healthy eating, physical activity together | • Share regular modest physical activity (e.g. walking, swimming, tennis, others) ○ Share in healthy eating behaviours (e.g. shop for food, prepare meals, and/or eat meals together) | • Participant reports of shared activities ○ Physical activity ○ Health eating ○ Others |
| Key function: social and emotional support | ||
| Maintain frequent contact | • Face-to-face contact • Telephone contact • Electronic contact (web, e-mail, text message) | • Contact records or reports |
| Encourage, enhance motivation | • Point out progress • Reassure of long-term nature of diabetes management • Reassure that medical care and medications can help • Reassure that one is ‘doing your best’ | • Audits of topics covered • Participant reports of support received/provided using standard measures |
| Provide support in dealing with day-to-day stressors | • Use problem-solving intervention techniques • Share stories of challenges and successes • Be available to listen and discuss problems | • Audits of topics covered • Participant reports of types interactions addressing problem solving |
| Tailoring of support to regional and cultural practices and settings | • Consideration of national, regional and cultural differences in social support, preferences for types and styles of social support • Providing support that is tuned to individual, social and cultural features | • Interviews with program staff and peers to characterize key features of support within their settings and cultures • Participant ratings of their satisfaction with peer support provided and the extent to which support is easily accepted |
| Advocate for and represent those with diabetes | • Serve on advisory committees • Encourage individuals and groups to assert their needs with health providers, community organizations | • Program documentation of ○ Committee and advisory roles ○ Advocacy activities |
| Ethical considerations | • Consideration of individual rights, privacy and limits on roles of peer support within the contexts of different countries, cultures and settings | • Documentation of ethical issues emergent through individual projects • Participant ratings of being treated with consideration for their rights, privacy, etc. |
| Key function: linkage to clinical care | ||
| Develop and maintain linkages care providers | • Organize peer support within primary care or other principal source of clinical care • Maintain active linkages with providers of primary and clinical care such as by referral, meetings to discuss key issues, training, etc. | • Characterization of linkages with primary care and systems of care • Audits of key interactions (e.g. # referrals to peer support, training of peer supporters) between support and care providers • Participant ratings of extent to which peer support is connected to sources of care |
| Encourage regular clinical care, partnership with clinical providers | • Remind each other of times for regular physician visits • Encourage physician visits when circumstances or symptoms warrant • Coordination with clinical practices and guidelines within country and setting | • Audits of topics covered • Participant reports of regular, out-patient clinical care |
| Behavioural objectives | Specific operational approaches to behavioural objectives | Outcome/measurement |
| Key function: assistance in managing and living with diabetes in daily life | ||
| Assist problem solving to support regimen adherence in daily life | • Use problem-solving intervention techniques • Share stories of challenges and successes • Assist in changing routines or other adjustments to facilitate adherence | • Audits of topics covered • Participant reports of types interactions addressing problem solving • Participant reports of management tasks addressed |
| Engage in healthy eating, physical activity together | • Share regular modest physical activity (e.g. walking, swimming, tennis, others) ○ Share in healthy eating behaviours (e.g. shop for food, prepare meals, and/or eat meals together) | • Participant reports of shared activities ○ Physical activity ○ Health eating ○ Others |
| Key function: social and emotional support | ||
| Maintain frequent contact | • Face-to-face contact • Telephone contact • Electronic contact (web, e-mail, text message) | • Contact records or reports |
| Encourage, enhance motivation | • Point out progress • Reassure of long-term nature of diabetes management • Reassure that medical care and medications can help • Reassure that one is ‘doing your best’ | • Audits of topics covered • Participant reports of support received/provided using standard measures |
| Provide support in dealing with day-to-day stressors | • Use problem-solving intervention techniques • Share stories of challenges and successes • Be available to listen and discuss problems | • Audits of topics covered • Participant reports of types interactions addressing problem solving |
| Tailoring of support to regional and cultural practices and settings | • Consideration of national, regional and cultural differences in social support, preferences for types and styles of social support • Providing support that is tuned to individual, social and cultural features | • Interviews with program staff and peers to characterize key features of support within their settings and cultures • Participant ratings of their satisfaction with peer support provided and the extent to which support is easily accepted |
| Advocate for and represent those with diabetes | • Serve on advisory committees • Encourage individuals and groups to assert their needs with health providers, community organizations | • Program documentation of ○ Committee and advisory roles ○ Advocacy activities |
| Ethical considerations | • Consideration of individual rights, privacy and limits on roles of peer support within the contexts of different countries, cultures and settings | • Documentation of ethical issues emergent through individual projects • Participant ratings of being treated with consideration for their rights, privacy, etc. |
| Key function: linkage to clinical care | ||
| Develop and maintain linkages care providers | • Organize peer support within primary care or other principal source of clinical care • Maintain active linkages with providers of primary and clinical care such as by referral, meetings to discuss key issues, training, etc. | • Characterization of linkages with primary care and systems of care • Audits of key interactions (e.g. # referrals to peer support, training of peer supporters) between support and care providers • Participant ratings of extent to which peer support is connected to sources of care |
| Encourage regular clinical care, partnership with clinical providers | • Remind each other of times for regular physician visits • Encourage physician visits when circumstances or symptoms warrant • Coordination with clinical practices and guidelines within country and setting | • Audits of topics covered • Participant reports of regular, out-patient clinical care |
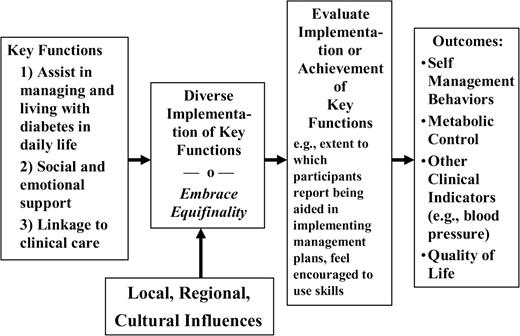
Figure 1 outlines a process in which the Key functions are implemented as modified by local, regional and cultural influences that include the health care system, government programmes and policies and population characteristics. Describing and promulgating varied operational approaches to each Behavioural Objective in Table 1 could facilitate local development of programmes, provide for knowledge exchange among programmes and cultivate incrementally a refined and perfected set of key functions and ways of addressing them. This could be done internationally through web-based exchange of programme models, training curricula, patient education materials, etc. Individual sites and projects could then draw from these and develop their own programme approaches which combine (i) tailoring to their settings, populations and specific strengths and challenges; (ii) taking advantage of up-to-date international knowledge and experience and (iii) comprehensiveness in their attention to each of the Key functions.
Model for International Dissemination and Evaluation of Peer Support
An example of broad functions and cultural specificity in social support
An example of how variation in implementation or local manifestation of a pattern may occur amidst underlying generality of basic functions across cultures lies in research on a distinction between Non-directive and Directive Support. Fisher et al. have carried out a number of studies of these two types of support:
Non-directive Support—cooperating without taking over, accepting recipient's feelings and choices, e.g. ‘Ask if you need help’ or ‘Make it easy to talk about anything’.
Directive Support—taking control, prescribing ‘correct’ feelings and choices, e.g. ‘Take charge of your problems’ or ‘Push you to get going on things’.
In general, Non-directive Support is associated with better metabolic control, better emotional status and better quality of life among adults with diabetes and a number of other groups, including adults with HIV/AIDS, lupus, several cancers, etc.44,50–54 However, Directive Support appears to be advantageous in urgent circumstances or those in which the recipient lacks the skills or resources to cope with a particular challenge. Consider several phases of dealing with cancer. The night you are waiting for the results of a biopsy, you need someone just to ‘be there’ for you and not to tell you what to do. The night you come home from surgery, you need someone to ‘take charge’ and tell you ‘all you have to do is worry about yourself, I'll take care of everything else’.
Recently, the measure of social support has been used in samples from several cultures. In a study of older adults as part of the Thai Family Well-Being Study (Nittaya Kotchabhakdi and colleagues from the National Institute for Child and Family Development at Mahidol University), we examined whether items that reflect Non-directive and Directive Support in US samples also reflect these among Thai adults. Several differences were illuminating. Items such as ‘Solve problems for you’ and Take charge of your problems that US respondents rate as Directive Support were rated by Thai adults as Non-directive. These kinds of actions tend to be viewed as intrusive in US culture. However, they appear to be accepted within Thai culture in which support providers are expected to know how to help without asking recipients to clarify what they want. This is reflected in a figure of speech within Thai culture, ‘Don't ask to feed the monk’. In offering food and other alms to monks walking through neighbourhoods in the morning, one does not ask if they wish the offering, one merely makes it. This does not mean, however, that the distinction between Directive and Non-directive support is not meaningful within Thai culture. As in US samples, ‘Tell you what to do’ was rated by Thai adults as clearly Directive.
These are preliminary findings, but they illustrate an important pattern. Broad categories like Non-directive and Directive Support or Key functions of peer support may transcend different cultures. However, the details of how those categories or functions may be manifest within a particular culture may be very specific. Thus, one might develop peer support interventions with emphasis on Non-directive support, but, in doing so in Thailand, one would recognize that exactly what typifies Non-directive support may be somewhat different than in the US and other countries.
Structure of peer support programmes and connection to health systems
Heisler55 has identified several implementation models for peer support, including peer coaches or mentors, peer community health workers, telephone peer support, web- and e-mail-based support and peer leadership of group self-management programmes. Peer support may vary in level of structure and connection to the health care system from highly structured, formalized and integrated (e.g. group visits led by clinicians or peer coaches working as extenders of professionals), to informal and detached from clinical systems (e.g. a resident of a village to whom others turn for health advice or two friends with diabetes encouraging each other to walk more often). More formalized programmes and those more integrated into health care systems have been easier to implement, study and evaluate.
Group visits have been broadly applied to clinical care in the context of diabetes, chronic low back pain, prenatal and well child care and tobacco cessation.56–58 This type of intervention integrates well into larger clinical practices. For example, seeing 10 patients with diabetes can easily be scheduled through the same 2-hour, group visit, using six to eight appointment slots instead of 10. The patients will have the benefit of the doctor's care and expertise, but can also share real-life challenges and solutions with peers. The visit can be billed in the customary fashion. Studies of this type of group care have shown high satisfaction with care59 and, in diabetes, improved metabolic control.33,34
A variation on this group care is the use of a ‘buddy system’ within the clinical group. Another variation on the clinical group has been utilized in a programme for patients with chronic back pain by encouraging randomly selected groups to meet informally between groups for exercise and conversation, providing facilities for both. This intervention showed improvements in some quality of life measures.56
Peer support providers, sometimes ‘model patients’ selected by a physician or health educator, are often hired as paid programme staff, undergoing some formal training (10–40 hours). Peers can contribute to group or individual intervention formats. This type of peer support is usually well integrated into the delivery system.
Informal peer support that is not integrated into health care is arguably most common. This can be in the form of peer organized support groups or friends and neighbours with similar conditions. Patients are often referred to such support groups by a health care professional. These types of peer groups operate at minimal cost and may take advantage of health system or community meeting space. Along with substance abuse and depression,60 diabetes is a common conditions for which such peer support groups are used. Perhaps, the most pervasive example of a peer support programme is Alcoholics Anonymous, with morethan 2 000 000 members in over 180 countries and 114 000 local groups [Welcome to Alcoholics Anonymous. URL http://www.aa.org/lang/en/catalog.cfm?origpage=10&product=83 (accessed on December 21, 2008)]. Meta-analyses indicate that, in combination with other types of addiction treatment, these programmes improve abstinence.61,62
New models of peer support have emerged as health systems use technology to improve efficiency. These include telephone- and internet-based support, results of which are promising.63–65 Some of these approaches are created and supported by health systems. Others, such as web-based chat rooms, are initiated by communities of affected individuals. The application of technologies can also help bridge distance for people with rare conditions.
Implications for evaluation
As the challenges of curriculum development are increased by the goal of international dissemination, so too are those of evaluation. Recognizing that there would be great variability in programmatic details and designs of individual evaluation studies across multiple settings, evaluation would be challenged to quantify dimensions or features of programmes that can be measured in different sites and linked to outcomes such as metabolic control or quality of life.
As with programme development, focusing on the Key functions of peer support rather than operational details provides one way of addressing the challenge of international evaluation. Key functions of peer support could provide a structure for evaluation. Assessing the extent to which each Key function is addressed provides a way of assessing common functions across differing programmes. Table 1 provides examples of outcomes and measures for such evaluation.
Figure 1 includes an outline of how implementation of Key functions may be examined as a predictor of self-management, clinical and quality-of-life outcomes. Participants from a group of programmes may all report the extent to which Key functions have been implemented. Controlling for a host of other variables (baseline values, demographics, socio-economic factors, available clinical delivery systems, etc.), this measure of extent of delivery of Key functions can be correlated with measures of clinical status and quality of life in a ‘dose–response’ analysis.
Additionally, it is possible to evaluate the extent to which each Key function contributes above and beyond the aggregate contributions of the others to the overall benefit of peer support. This would provide estimates of the value of specific aspects of peer support. Such analyses might also explore how different Key functions may be more or less helpful in different settings as a function, say, of cultural factors, level of poverty, demographic characteristics such as age and sex, duration/progression of diabetes or characteristics of primary care and systems of care.
Cross-site, overall evaluation.
Individual projects may be evaluated with experimental designs using control groups, wait-list control groups, comparison groups, etc. Complementary to these, an overall, cross-site evaluation could integrate observations across multiple individual projects. Multivariate statistical techniques developed over the past several decades can integrate data from experimental and non-experimental studies along with a wide range of other data. This could include the following:
intervention data (e.g. dose of intervention reported by participants);
individual-level data (e.g. clinical measures and demographics);
organizational level data (e.g. clinical management resources, type of health care system, linkage between peer support activities and health care providers, extent of available self-management resources other than peer support);
local and regional data (e.g. local poverty levels, employment opportunities, food practices in culture and region).
A hypothetical model for evaluating peer support is depicted in Figure 2. Analyses to test such a model would estimate the strength of each of the arrows depicted in the figure, at once controlling for the effects of all the others. This would yield strong estimates of the contributions of peer support such as in the arrows connecting ‘Breadth and Extent of Implementation’, ‘Intervention Exposure, Engagement’, ‘Self-Management Behaviours’ and ‘Clinical Status and Quality of Life’. With model estimates all well specified by virtue of being based on perhaps thousands of cases, estimates of benefits of intervention and intervention dose can be quite reliable and strong.
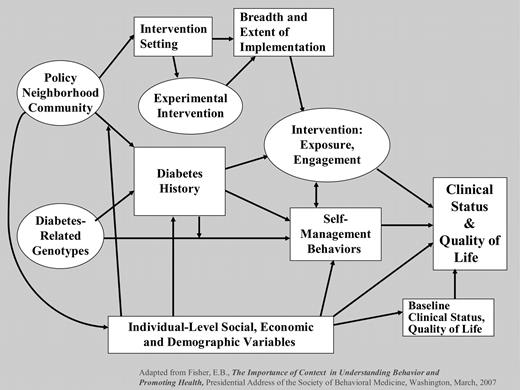
Possible multilevel, multivariate evaluation of peer support
Challenges for peer support programmes
As noted above, the roles of professionals, paraprofessionals and peers in health care may vary considerably across different countries and in different health care systems. Moreover, violations of or perceived threats to expected or claimed roles and prerogatives may elicit considerable conflict. Within this framework, a particular challenge is the extent to which peer support includes education regarding details of diabetes management or whether it is confined to enhancing motivation, providing encouragement and assisting in problem solving around adherence to self-management plans. This is likely an issue around which different countries would vary. In some, the prominence of information sources other than health care professionals is well established; in others, it is highly provocative and likely to antagonize professionals. This is a prime example of how programme models and curricula would need to leave room for international variation in the roles of peer support.
In addition to conflict over roles of those in the health care system, peer support interventions might conflict with social and cultural expectations of the roles of individuals living with diabetes, their families and communities. If cultural norms emphasize individual autonomy, the contributions of a peer might be viewed as threatening individual identity. In other settings that place great emphasis not on individual goals and needs but on those of the family, a peer support intervention that focused on the rights or needs of the individual would not be well accepted. Cultures which accord village or tribal or clan leaders authority over members’ lives and choices would need peer support to be integrated with such authority structures.
Attendance or participation in peer support may constitute another challenge. Although the majority of participants may attend a limited programme of six or eight self-management group classes, including those run by peers,66,67 maintaining such attendance to scheduled group events over the decades of diabetes management poses substantial problems. Informal, varied and flexible approaches to offering support may have advantages in maintaining engagement over such time periods. Reflections on ongoing follow-up and support from the Diabetes Initiative of the Robert Wood Johnson Foundation18 indicate the importance of both (i) support scheduled to convenience or on demand in order to fit within the individual's lifestyle and preferences, as well as (ii) proactive support to maintain contact with individuals, communicate continued interest and encouragement and keep individuals from falling out of contact with the care system.
As maintaining patterns of disease management may be advanced by peer support, maintaining sources of peer support may, itself, pose challenges. The tendency towards ‘burn-out’ in providing care of chronic diseases is not limited to professionals. Recognition, honoraria, opportunities for exchange of case material with other peer supporters, in-service training to enhance skills and, thus, satisfaction in effective work and other strategies may enhance retention of peer supporters in their roles. More broadly, programmes should anticipate that remaining a peer supporter for many years may be uncommon and, so, should normalize, anticipate and provide for limited tenure of individual supporters and constant replenishment of their ranks.
Training of peer supporters raises an interesting paradox. In the interest of enhancing their skill and expertise, is there a risk that excessive training or professionalism might compromise their ‘peerness’? This appears not to be a problem in programmes that offer extensive training that includes training in how to be effective in providing encouragement and support as well as knowledge about disease management. Still, one may wonder whether professionalism may raise problems. For example, might training peers in enforcing confidentiality stifle natural, free flowing support among informal social networks within neighbourhoods, churches, worksites or other organizations?
Summary and conclusions
That peer support might enhance diabetes management is based on substantial literature on peer support in other areas of health,1–7,10 modest evidence from a relatively small number of studies with adults with diabetes8 and a strong rationale based on the day-to-day demands of diabetes management and the likelihood that peer support might assist with daily management, maintaining motivation and dealing with emotional challenges and staying connected to clinical care.9
Following the principal of equifinality, focusing on the key functions of peer support may enhance both promotion across different cultures and settings as well as general evaluation of peer support. International promotion may be advanced by emphasizing the key functions of peer support—assistance in daily management, social and emotional support, linkage to clinical care—and then encouraging local variation in the specific ways they are addressed. By characterizing implementation of these key functions from programme records, survey of participants’ reports of receipt of the key functions and measurement of common end points, evaluation may span across diverse programmes and characterize the general benefits of peer support and the extent its several functions contribute to them.
Among many challenges are integrating peer support among the roles of professionals within health care, likely to vary widely across different countries and health systems, harmonizing the role of peers with family and others in individuals’ networks and communities, maintaining the engagement of both peer supporters and those they assist and keeping training and attention to quality of service delivered from distorting the fundamental characteristics of support from a peer.
Clearly, the challenges of promoting peer support in diabetes management internationally are substantial, but meeting them may not only enhance diabetes care around the world but also increase our understanding of how peer support is shaped by its contexts in cultures, families, neighbourhoods and health care systems, as well as shedding light on the contributions peer support may make to health in general.
Declaration
Funding: Robert Wood Johnson Foundation, Princeton, NJ, through its support of the National Program Office of its ‘Diabetes Initiative’ at Washington University in St Louis and the University of North Carolina at Chapel Hill. American Academy of Family Physicians Foundation and the Eli Lilly and Company Foundation through their support of Peers for Progress and its Program Development Center at the University of North Carolina at Chapel Hill.
Ethical approval: None.
Conflicts of interest: None.
References
Author notes
Fisher EB, Earp JA, Maman S and Zolotor A. Cross-cultural and international adaptation of peer support for diabetes management. Family Practice 2010; 27: i6–i16.

{kind=link}
{kind=link}