Article Text

Statistics from Altmetric.com
Summary box
While antibiotic misuse and overuse has often been the focus of antimicrobial resistance (AMR) science and policy, clinical microbiology in the Middle East is turning to evaluating war and conflict as drivers to antimicrobial resistance.
War has been implicated in the emergence of antimicrobial resistance as far back at the 1940s and these conditions have since persisted and intensified, with contemporary conflicts pressuring microbes with selective environments that contain unique combinations and concentrations of toxic heavy metals and antibiotics and providing niches and dissemination routes.
Iraq experienced a sequence of conflicts since the 1980s, and reports point to a progressive deterioration of Iraq’s national healthcare system, lack or limitation in trained staff, infection prevention and control, access to antibiotics as well as sanitation control and debridement of highly contaminated wounds from explosives or burns, as well as inappropriate diagnoses and drug regimens, all potential contributors to the rising rates of AMR in Iraq.
AMR co-selection from heavy metals is becoming more strongly implicated due to conflict-driven environmental contamination, as with lead, mercury, chromium, copper, lead nickel and zinc used to coat bullets, missiles, gun barrels and military vehicles, while antimony, barium and boron are used as weapon-priming compounds.
The rise of AMR in Iraq, with indications of regional and global spread, remains direly understudied, where clinical, microbiological, historical, ethnographic and environmental research is needed to conclusively establish the roles that war and conflict play in the rise of multidrug-resistant organisms.
Understanding the link between AMR and conflict is essential for a global response to AMR, especially with little indication that global conflict will abate in years to come.
Introduction
Antimicrobial resistance (AMR) is rising globally at an alarming rate and, if left unaddressed, expected to cause 10 million deaths per year by 2050.1 This growing threat has widely been attributed to the overuse and misuse of antibiotics and/or the use of substandard antibiotics in humans, livestock and as a byproduct of environmental contamination. While antibiotic use has often been the focus of AMR science and policy, only recently has clinical research in microbiology turned to evaluating other biocides, such as heavy metals and quaternary ammonium compound disinfectants (QACs), as potential drivers that co-select for resistant pathogens.2 In the Middle East, spiking rates of antibiotic resistance, especially in Gram-negative pathogens such as Acinetobacter baumannii, Pseudomonas aeruginosa and Klebsiella pneumoniae, have also implicated another underinvestigated pathway for AMR: the direct and indirect roles of wars and conflicts, and their associated implications to healthcare (these can include, but are not limited to, the breakdown of healthcare systems, the loss of skills healthcare personnel, deteriorating infection and sanitation controls in healthcare settings, and difficulty of access to effective therapy, therapeutics and diagnostics), in driving the emergence of resistant pathogens.
Investigating the relationship between wars, conflicts and transformations in antimicrobial susceptibility and resistance patterns is not unprecedented. War has been implicated in the emergence of AMR as far back at the 1940s, when widespread industrial-scale mass production and application of arsenicals, sulfonamides and disinfectant QACs, as well as the mass introduction of penicillin as a prophylactic and in the treatment of soldiers’ injuries during World War II, set the stage for the selection for drug resistance.3 These conditions and consequences have persisted and may have even intensified, with subsequent conflicts. Contemporary conflicts, waged in urban and industrialised landscapes, pressure microbes with selective environments that contain unique combinations and concentrations of toxic heavy metals and antibiotics, while simultaneously providing niches and dissemination routes for microbial pathogens. These can include the high number of wounded, the nature of wounds, refugee displacement, collapse of sanitation controls, loss of diagnostics and skilled healthcare personnel, the dismantlement of healthcare infrastructures and the placement of often under-resourced and improvised field hospitals where both injured combatants and civilians are exposed to harmful pathogens with limited care and resources to properly recover.4–6
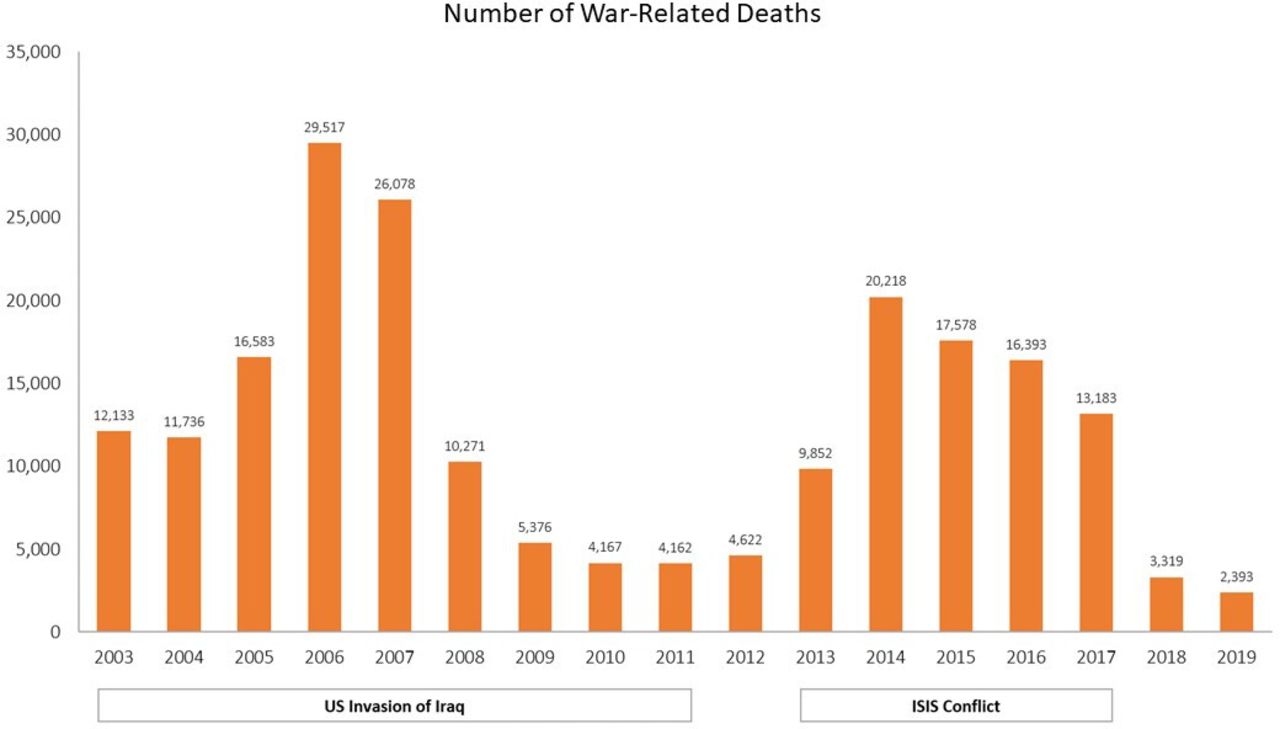
Despite increased attention to AMR, however, the specific role of current armed conflicts and the resistance-inducing properties of non-antibiotic antimicrobials, such as heavy metals and QACs, in the development and proliferation of this phenomenon continue to be poorly understood. Iraq experienced a sequence of conflicts since the 1980s that coincided with the emergence and spread of pathogens with specific antibiotic resistance patterns (figure 1, online supplemental table 1). In what follows, we piece together literature on AMR and conflict in Iraq in order to explore the specific contexts and potential drivers for antimicrobial resistance during two phases of this history: the US invasion and occupation of Iraq (2003–2011) and the conflicts with the Islamic State of Iraq and Syria (ISIS) starting in 2014. In-depth historical, ethnographic, epidemiological, and clinical and molecular microbiological research is still needed to understand the contingencies of these resistance mechanisms and the roles played by the specific conflicts in which they emerged, as well as the overall process of conflict-driven antimicrobial resistance.
Supplemental material
{kind=link}
Frequency of war and conflict-related deaths in Iraq (2003–2019). ISIS, Islamic State of Iraq and Syria.
AMR in the history of conflict in Iraq
Iraq witnessed devastating conflicts over the last four decades, prominently including the Iran-Iraq war (1980–1988), First Gulf War in 1991, the United Nations economic sanctions on Iraq following the Iraqi invasion of Kuwait (1990 until 2003), the US invasion and occupation of Iraq (2003–2011), including a period of militarised violence (2005-2007), and the conflicts with the ISIS (2014–2017). Although data on antimicrobial susceptibility in Iraq from the 1980s are scarce, literature from Iran during the same period indicate an emergence of resistant Gram-negative pathogens among Iranian soldiers throughout the Iran-Iraq war, with declining susceptibility to antibiotics commonly used at the time.7 8 Scientific literature on conflict-related antimicrobial resistance emergence in more prominence during and after the US invasion and occupation of Iraq since 2003, with both US military medicine research, situated in combat support hospitals and war theatres in Iraq, along with research conducted by humanitarian organisations such as Medecins Sans Frontières (MSF), document an emergence and spread of antimicrobial resistance in tandem with the conflict in Iraq.6 As bombings, unsafe living conditions and destruction of public infrastructure became commonplace in Iraq, these factors overlapped with a catastrophic worsening of AMR, potentially the result of a broader ecology of war that has been decades in the making.9
US invasion and occupation (2003–2011)
During the US occupation, both the WHO and MSF reported growing concerns over severe shortages of both medicine and medical staff, a situation that dates back to UN economic sanctions on Iraq imposed after Iraq’s invasion of Kuwait in 1990. By 2006, however, two-thirds of doctors reported unavailability of essential drugs and equipment more than half of the time and more than 90% reported lacking skilled health workers in their facilities and reduced quality of care.10 Many healthcare workers fled from Iraq since 2003, with many reporting violent attacks on health facilities or personnel as a primary driver.10 With a lack of a well-established antimicrobial stewardship system, especially compromised by the conditions of war faced by the country’s healthcare system, the administration of broad-spectrum antibiotics as empirical therapy for war wounds was widespread, leading to selection for highly resistant organisms.11 Moreover, the administration of even broader-spectrum drugs for the treatment of multidrug-resistant (MDR) infections further contributed to AMR by increasing the potential for nosocomial transmission. In one example of the extent of the problem of AMR during the US invasion, Murphy et al found that 55% of patients with suspected osteomyelitis had an MDR organism at their time of admission to the hospital and that there was a significant association between patient history of more than two surgical procedures performed in Iraq and having a positive MDR isolate.12
P. aeruginosa, Staphylococcus aureus, K. pneumoniae and A. baumannii were identified as major contributors to multidrug resistance in Iraq and were problematic for both military and civilian doctors.11 Drug resistance in these four microbes was exacerbated in such contexts as burn and field hospitals,13 with indications of regional and international transmission and spread.14 Currently available articles indicate that, although there are no mentions of A. baumannii in Iraq in the 1980s, resistant A. baumannii was detected by Iranian researchers among Iranian soldiers returning from the Iraqi warfront to a hospital in Shiraz.8 Sadeghi explained the emergence of resistant Acinetobacter as part of a general trend towards growing nosocomial spread of Gram-negative pathogens with reduced susceptibility to antibiotics in Iranian hospitals throughout the period of the Iran-Iraq war.8 Resistant A. baumannii is now of growing global concern, having gained the moniker ‘Iraqibacter’ following its spectacular rise as a resistant and nosocomial pathogen in Iraq and spread, via injured soldiers, to hospitals in the USA and the UK, constituting a global ‘pathology of intervention’.15 In-depth historical and phylogenetic analysis is still needed to ascertain whether resistance mechanisms in these pathogens first emerged as early as the Iran-Iraq war in the 1980s and gained traction thereafter, or first appeared during the US invasion and occupation of Iraq.
ISIS conflict (2014–2017)
In 2014, ISIS’s armed conflict against the Iraqi state led to the wounding and killing of hundreds of civilians and the displacement of thousands throughout the course of the Syrian conflict16 and further contributed to the dismantlement of what remained of the state’s economic, social and healthcare infrastructures once more.
Continued research is needed to understand the full effect of the ISIS conflict on AMR and in what ways it may have coincided or differed from previous conflicts. Reporting during the ISIS conflict was predominantly undertaken by humanitarian organisations active in Iraq at the time. In a report issued by MSF in 2019, for example, a hospital in East Mosul, a city heavily affected by the ISIS crisis, reported that 90% of patients with a microbiologically confirmed infection had been infected with an MDR microorganism.17 The same four bacteria (P. aeruginosa, S. aureus, K. pneumoniae and A. baumannii) that emerged during the US invasion were also prevalent during the conflict with ISIS. However, resistance to other classes of antimicrobial agents had since been further noted. For example, a study conducted by Lafi et al in a hospital in Ramadi revealed that while S. aureus and P. aeruginosa were still one of the most common isolates in wounds, S. aureus had developed growing resistance to vancomycin and P. aeruginosa to imipenem.18 Similarly, in 2016, Ghaima et al studied the antimicrobial susceptibility of A. baumannii from burns and wounds in patients in Baghdad hospitals and found that resistance had increased, especially to colistin.19
It is likely that drug resistance had been further aggravated during the ISIS conflict by long-standing shortages of healthcare workers, precarity of medical institutions and the nature of wounds among civilians and combatants alike. It is worth mentioning that tactics used during the ISIS conflict further blurred the lines between civilians and combatants and led to thousands being wounded and seeking treatment in the context of limited resources. The protracted conflict against ISIS has led to displacements of large groups of people, many of whom travelled widely within the country and abroad in the pursuit of healthcare. This, along with the movement of refugees, may continue to contribute to the spread of resistance genes and resistant infectious agents for years to come. In-depth ethnographic and epidemiological research, especially ones that stretch across regional and international borders, are still needed to ascertain the roles that the nature of wounds, environmental contamination, and the precarity of access to healthcare played in the development of chronic infections with MDR organisms during this phase of conflict in Iraq.
AMR in conflict settings: a pressing concern
Protracted conflict in Iraq has had adverse implications to population health. And yet, it is worth noting that Iraqi institutions have rarely been the source of information on AMR in Iraq across these conflict periods. Rather, what we know about AMR in Iraq is largely sourced from US military medicine during the period of the US invasion and occupation and from humanitarian organisations operating in Iraq throughout these conflict period. One of the legacies of British rule in Iraq was the establishment of an expansive healthcare system that attracted patients region-wide for medical treatment in Iraq.20 Armed conflicts since the 1990s have accompanied a progressive deterioration of Iraq’s national healthcare system, leading to lack or limitation in trained staff, infection prevention and control, access to many classes of antibiotics and proper clinical microbiology for guiding clinicians.21 Iraq’s biosurveillance and laboratory capacities have also been impacted, leading to gaps in core capacities and national disease surveillance.22 Wounds from explosives or burns may be highly contaminated with bacteria. Additionally, lack of training in proper wound debridement and lack of patient follow-up can lead to higher rates of health complications.23 Surgeons and healthcare personnel are often tasked with stabilisation as opposed to long-term care for wounds and infections. In such time-sensitive and under-resourced settings, all of the above, along with inappropriate diagnoses and drug regimens administered with expired or outdated drugs, may all be contributing to the rising rates of AMR in Iraq.
Conflict settings exacerbate bacterial spread due to insufficient sanitary resources to meet basic hygiene needs. In conflict settings, civilians and combatants suffer from the lack of access to proper water, sanitation and hygiene (WASH), thus increasing their exposure to pathogenic microbes. Furthermore, growing attention is being paid to the roles that heavy metal contamination might play in triggering drug resistance. Heavy metals used in weapons persist in the environment, with explosives, for example, harbouring huge amounts of lead and mercury.24 25 In addition, metals such as chromium, copper, lead nickle and zinc are used to coat bullets, missiles, gun barrels and military vehicles, while antimony, barium and boron are weapon-priming compounds.26 27 In general, the use of heavy metals in weapons has increased since the end of World War II25 and many bacterial species have been shown to have evolved resistance mechanisms to combat heavy metals’ toxicity.28 These mechanisms are encoded by resistant genes to heavy metals and antimicrobial agents that are physically linked on mobile genetic elements. More importantly, heavy metals can induce selective pressure on microbial populations leading to AMR through a mechanism called ‘co-selection’ which occurs via three major ways: co-resistance, cross-resistance and co-regulatory resistance.
Taken together, a destroyed healthcare infrastructure, inappropriate microbial therapies, limited resources, high heavy metal contamination in humans and the environment,29 30 and lack of WASH, combined, likely play instrumental roles in the catastrophic rise of AMR in Iraq and, by extension, regionally and globally. This remains, however, direly understudied. Clinical, microbiological, ethnographic and environmental research is needed to conclusively establish the multiple and compounding roles that wars and conflicts play in the rise of multi-drug resistant organisms. It is imperative for future research to address gaps in understanding how AMR came to be historically constituted across time, in interaction with social, political and economic processes and events. Understanding these linkages between AMR and conflict, especially across time, is essential for a global response to AMR, especially as there is little indication that conflict, worldwide, will abate in years to come.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Press release
Footnotes
Handling editor Seye Abimbola
Contributors AAF, AR, SES, NKJ, AA and MK performed the literature search and the analysis of the data. AAF, AR, SES, NKJ, MK, OD, VKN and ZAS wrote and proofread the article.
Funding This study was funded by the Center for Research and Education in the Ecology of War (CREEW).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.