Article Text

Abstract
Introduction Power shapes all aspects of global health. The concept of power is not only useful in understanding the current situation, but it is also regularly mobilised in programmatic efforts that seek to change power relations. This paper uses summative content analysis to describe how sexual and reproductive health (SRH) programmes in low-income and middle-income countries explicitly and implicitly aim to alter relations of power.
Methods Content analysis is a qualitative approach to analysing textual data; in our analysis, peer-reviewed articles that describe programmes aiming to alter power relations to improve SRH constituted the data. We searched three databases, ultimately including 108 articles. We extracted the articles into a spreadsheet that included basic details about the paper and the programme, including what level of the social ecological model programme activities addressed.
Results The programmes reviewed reflect a diversity of priorities and approaches to addressing power, though most papers were largely based in a biomedical framework. Most programmes intervened at multiple levels simultaneously; some of these were ‘structural’ programmes that explicitly aimed to shift power relations, others addressed multiple levels using a more typical programme theory that sought to change individual behaviours and proximate drivers. This prevailing focus on proximate behaviours is somewhat mismatched with the broader literature on the power-related drivers of SRH health inequities, which explores the role of embedded norms and structures.
Conclusion This paper adds value by summarising what the academic public health community has chosen to test and research in terms of power relations and SRH, and by raising questions about how this corresponds to the significant task of effecting change in power relations to improve the right to SRH.
- Maternal health
- Public Health
- AIDS
- Review
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Power shapes all aspects of global health: from the policies governing healthcare availability, accessibility, acceptability and quality to the health status of populations. Existing reviews on power in sexual and reproductive health (SRH) examine discrete elements of how SRH interventions address power.
WHAT THIS STUDY ADDS
We identified key trends and themes, including a prevailing focus on behaviour change strategies, and the related use of research approaches that are focused on detecting changes therein. At the same time, especially in the context of HIV and/or gender-based violence, there are many programmes that seek to effect change on multiple levels and use complicated study designs that harness epidemiological approaches to assess change.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Further development of these approaches and increased programme and research attention to power relations at the community, organisational and policy/governance levels would complement the behaviouralist research. This should be done in a way that links research back to its purpose: producing a body of evidence that together can start to answer the question of how to shift power dynamics in favour of the right to SRH.
Background
Power shapes all aspects of global health: from the policies governing healthcare availability, accessibility, acceptability and quality to the health status of populations and inequities therein. This is by no means a novel assertion. Researchers, activists and policy-makers working across contexts recognise the centrality of power for understanding global health (eg, see Gore et al1–5). Current work builds on diverse streams of earlier theoretical and empirical work, such as explorations of the social determinants of health undertaken in the 19th century by German pathologist Rudolf Virchow and the 20th-century Indian Dalit rights leader, Dr B R Ambedkar.6 7 Over the past 20 years, the concept of power has been evoked—explicitly or implicitly—in a range of multilateral agenda-setting efforts in global health, such as the WHO Commissions on Macroeconomics and Health8 and the Social Determinants of Health9 to efforts more specific to sexual and reproductive health (SRH), like the Unified Accountability Framework for the UN Secretary General’s Global Strategy for Women’s Children’s and Adolescents’ Health.10
Power operates at all levels and ultimately gets translated into what services are delivered and in what manner, who gets access and on what terms, and who is excluded. Thus, the concept of power is not only useful in understanding the current situation, but also it is regularly mobilised in programmatic efforts, including those that seek to change power relations that work to limit people’s access to or use of services. Such programmes are common in SRH, a distinct field within global health where the role of power dynamics, such as how gender relations are ladened with power, has long been recognised (eg, see Boydell et al.11–14 Programmatic efforts aiming to alter power relations in SRH involve diverse actors and encompass a wide range of approaches, like non-governmental organisation (NGO)-led efforts to empower marginalised groups, national governmental strategies to shift power dynamics within households (eg, regarding violence against women) and grassroots efforts to demand a greater role in health policy-making for particular constituencies. Yet, while power is the subject of increasing attention in research describing the status quo, as well as strategies and programmes seeking to change the status quo, it has not been deeply explored in evidence reviews. Existing reviews look only at discrete elements of how SRH interventions address power, such as how they try to shift gender norms (eg, see Ruane-McAteer et al15). This gap is likely due to the breadth of the concept of power and the associated challenges in defining research questions and ensuring that findings are useful to individuals working in programme design, who may seek a more parsimonious approach.
This paper uses summative content analysis to describe how SRH programmes in low-income and middle-income countries (LMICs) described in the peer-reviewed literature explicitly and implicitly aim to alter relations of power. The focus is on how programmes seek to change power relations rather than whether or not programmes in SRH successfully change power relations. We contribute to answering a broad research question: ‘how do programmes seek to change power relations in order to promote the right to SRH?’ In this bounded paper, we address a component of that question; that is, ‘how do programmes documented in the peer-reviewed literature address power relations in order to promote the right to SRH?’
The paper is necessarily incomplete, as many efforts seeking to change power dynamics are not described in the peer-reviewed literature and others will not be responsive to our search terms. Most of what does appear in the peer-reviewed literature is research and evaluation, rather than overarching programme descriptions. Our analysis does not address the ways that power shapes SRH programmes and research, but rather starts downstream, looking at how programmes documented in the peer-reviewed literature seek to harness or change power dynamics.
This paper focuses on LMICs. We recognise that questions related to power are also salient for high-income countries (HICs). We chose to focus on LMICs for two reasons: first, because there are several strands of global agenda setting and policy implementation related to SRH that were primarily focused on LMICs, such as the 1994 Cairo International Conference on Population and Development (ICPD) and its subsequent reviews every 5 years; second, for the most part, the programmes we review have been designed for implementation and potential replication in the LMIC context. This reflects a broader siloing between LMICs and HICs in global health, which is in itself a reflection of power dynamics in global health governance.
This summative content analysis is a first step towards summarising what has been tried, in what SRH domains it has been tried, how it was framed (eg, human rights, legal empowerment and structural interventions) and what lessons were learnt about power. The paper will lay groundwork for additional research, policy-making and action on power dynamics as a determinant of the right to SRH, including reproductive rights.
The concept of power
Power as a concept has deep and rich conceptual antecedents spanning many disciplines. Power is a complex construct, but many theories of power point to two key dimensions: power as a force that creates structures of formal and informal control, such as laws and social norms; and, second, power as a resource to be generated and mobilised for individual and collective transformation, as in self and collective efficacy, rights claiming, and empowerment.14 16 Social scientists often describe these two dimensions as structure and agency. Thus, power is not inherently good or bad for population health, but it is omnipresent, influencing law and policy, organisations, norms and beliefs, interpersonal relations and individual decision space.14
Research to understand how structure and agency are created, change and operate to influence health is similarly wide-ranging. This research builds mostly on theories and approaches from the social sciences, such as political science, anthropology, demography and social epidemiology, and has produced a rich evidence base examining the explicit and/or implicit role of power dynamics in phenomena such as health agenda-setting; health policy implementation; the influence of political trends on population health; and the impact of social hierarchies on health workers, health behaviours and status, access to care and quality of care received (eg, 12 17–23). Such descriptive and exploratory work sheds light on why things are the way they are and how they came to be that way. Within the confines of public health programme research, exploration of structure and agency is generally more limited, as such research is often based in a biomedical paradigm and consequently focuses on factors that are considered to be modifiable by public health actors.
Among the domains of global health, SRH has attributes that make a power lens particularly apt. Donor, governmental, organisational and individual understandings and approaches to sexuality and fertility reflect social norms and mores regarding gender roles and reproduction.11 12 24–26 These norms are part of the structure, influencing agency for all people engaged in SRH programme and service design, implementation and use. Structure and agency are not static. Rather, power is dynamic, and the SRH terrain is often contested, with tensions and conflict regarding SRH occurring within households and communities, within and among organisations, and within and among governments.11 14 26
However, there are important areas of agreement among global and national policy-makers. At the ICPD held in Cairo in 1994, the international community coalesced around a vision of SRH that foregrounds reproductive autonomy, as opposed to population control.27 Similarly, there is general consensus regarding the need to eradicate reproductive coercion and to promote equity in SRH service access, quality and outcomes.27 However, factors such as gender hierarchies, political and national ideologies, and deeply held beliefs about appropriate motherhood and non-procreative sex continue to influence how public health evidence is (or is not) reflected in policies, programmes and practice.
Since the ICPD in 1994 and with the advent of unprecedented funding and global health activism accompanying the HIV pandemic, new approaches to addressing power within SRH policies, funding and programmes have been tried, often called structural interventions. The limited impact of efforts focused on individual behaviour change was emphasised by those advocating for structural interventions, which aim to change the context within which health and illness are produced, and factors at the community, organisational (eg, health system), and law and policy levels.28–31
Methods
Since we were interested in how programmes seek to change power relations rather than whether they changed power relations, our search focused on papers that describe programmes that aim—implicitly or explicitly—to address power, even if results are not provided.
Perhaps because power is a complex and not especially bounded or discrete construct, it is not always explicitly discussed. Thus, we sought a method that would allow us to find and compare keywords and content, and to interpret the context in which those keywords and content are used.32 To achieve this, we conducted a summative content analysis. Content analysis is a qualitative approach to analysing textual data; in our analysis, peer-reviewed articles describing programmes aiming to alter power relations to improve SRH constituted the data.33 Summative content analysis has not been widely used in global health, but among the analysis and review methodologies, its focus on summation and ability to assess what is both explicit and implicit in the text was well suited to our research question.
This summative content analysis explores two questions: (1) how do programmes that seek to change power relations try to do so? and (2) what are the reported lessons learnt from these programmes in relation to power?
As summarised in table 1, search words were chosen to encompass the three concepts central to our question, namely, programme, SRH and power.
Search terms applied
We selected the keywords working from articles already known to the authors to be relevant to the study objective; we then piloted and refined the search terms for programme, SRH and power. The words included in the SRH search terms were intended to capture all elements of SRH. We limited our power-related inclusion criteria to factors, activities and constructs whose relationship to power were explicitly described in the paper or implied, such as respectful maternity care and reproductive autonomy. The authors had multiple discussions regarding what constituted ‘addressing power’; the final inclusion and exclusion criteria are provided in table 2.
Inclusion and exclusion criteria
We included papers where any element of the programme met our inclusion criteria. We searched PubMed, Scopus and Academic Search Complete and, based on title and abstract and excluding duplicates, imported 342, 15 and 60 papers to Zotero for full review, respectively. We looked only at papers that were published after 1994, reflecting the watershed event of ICPD and its acknowledgement of human rights, gender equity and reproductive autonomy as germane to reproductive health and rights, population and development, as an important transition in the field. At the start of the full-review process, three authors independently assessed the same 10 studies to determine inclusion or exclusion to confirm that criteria were clear and being applied consistently. We then read the articles in their entirety, eliminating those that did not meet our criteria. At the end of this process, we had 91 articles. We did not apply criteria related to language, but our search produced only English language results.
We found that we had some papers relating to the same programme, such as protocols and results for the same programme. We linked these records, and only kept both papers where they yielded new information. For example, often the protocol had greater detail about the content of the programme, while the results paper provided information about the lessons learnt about power. In a few cases, we had two or more papers describing programmes implemented by a single NGO that were related but distinct; we classified these as separate programmes.
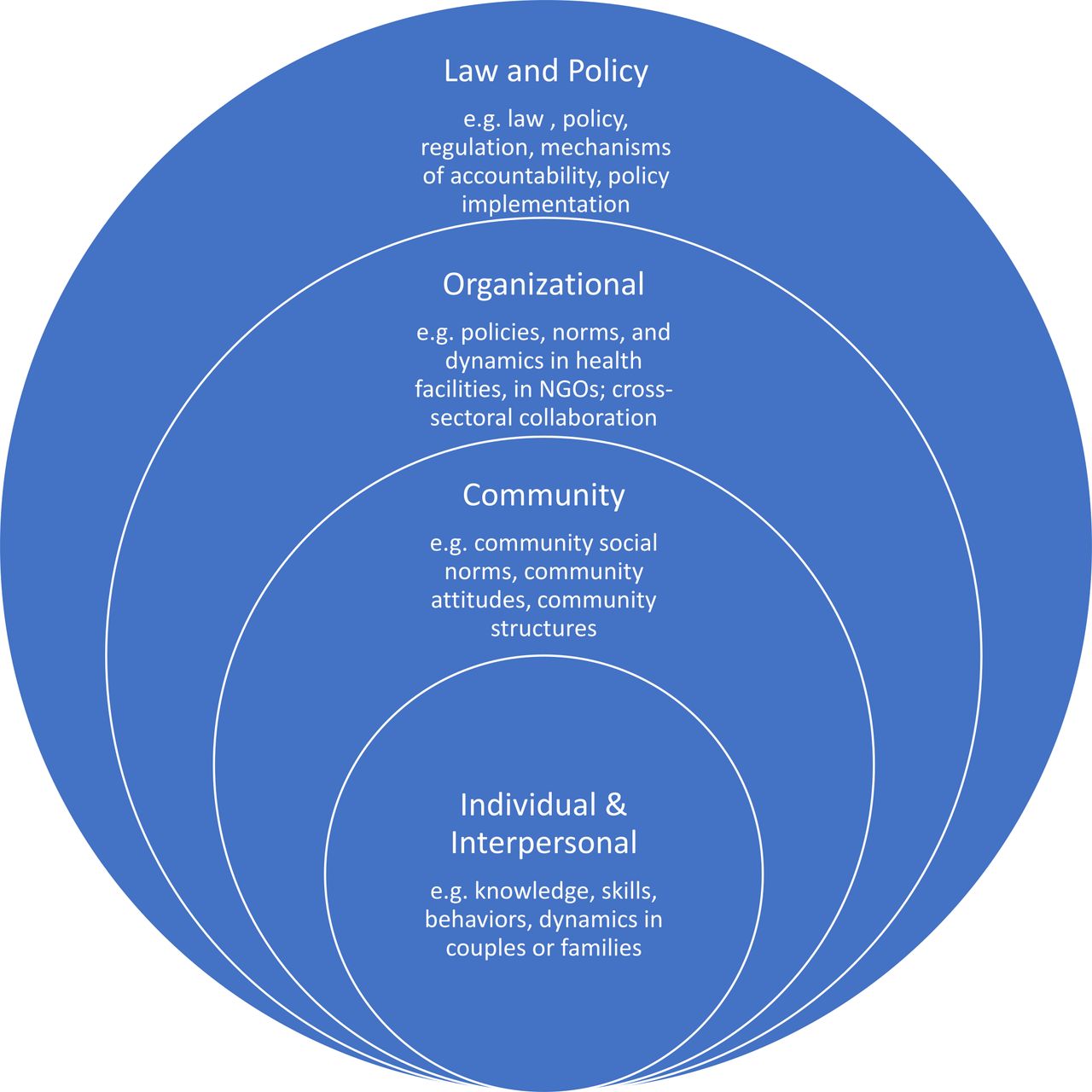
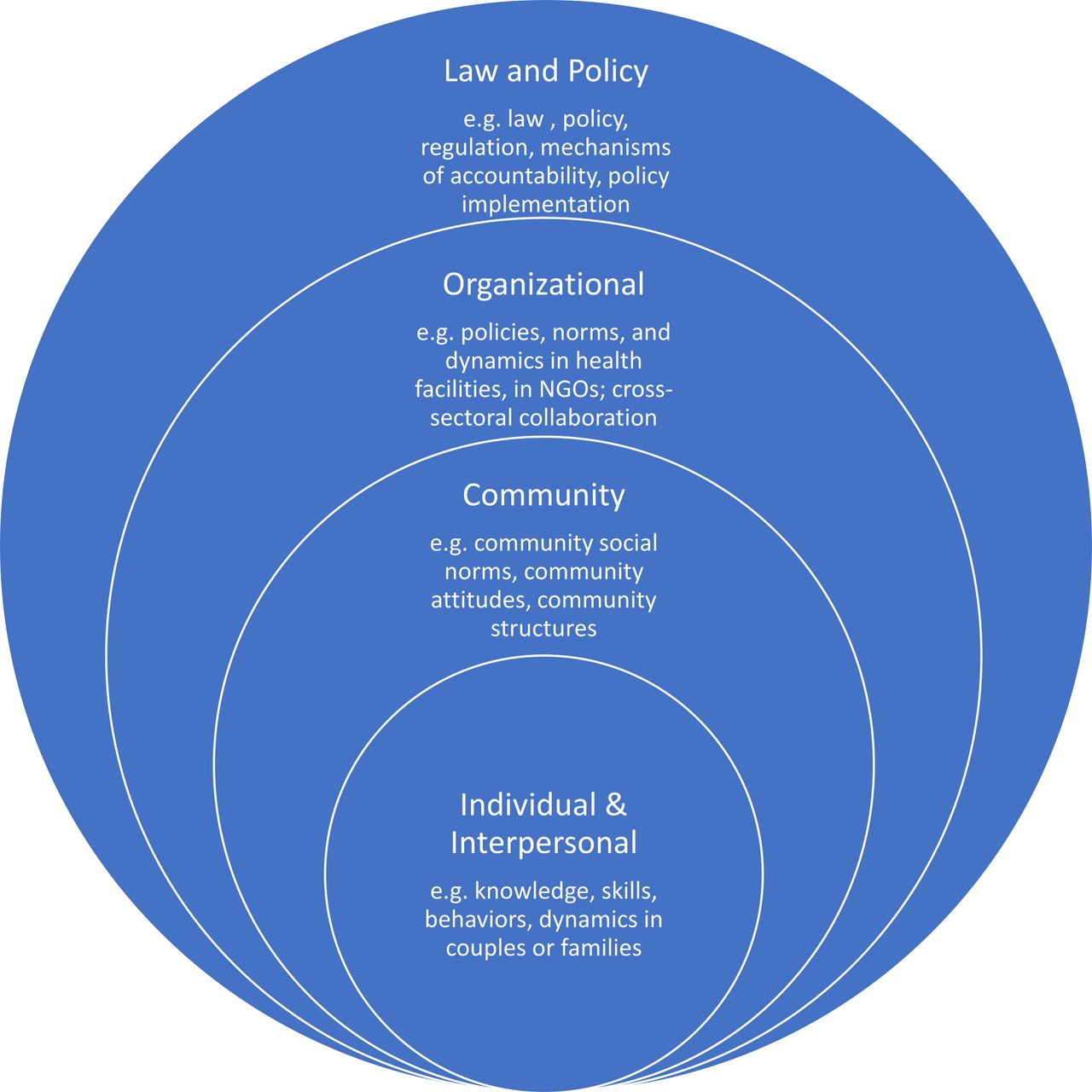
We then entered the articles into an extraction tool (a spreadsheet) that included basic details about the programme and lessons learnt about power as a result of the programme, if provided. We also indicated what level of the social ecological model—as defined in figure 1—the programme activities addressed. Social ecological models are used to illustrate the multiplicity of factors—including the individual, social and other structural factors—that shape health, as well as domains of intervention and change.34 We included four levels in our approach to the social ecological model: individual/interpersonal, community, organisational and law/policy. Based on our background reading, we collapsed individual and interpersonal into a single level because we realised many of the interventions aimed to affect both levels through one activity, for example, training and equipping commercial sex workers to learn about sexually transmitted infections and to demand that their partners use condoms. We used the programme description and the outcome measures specified in the respective papers as a basis for deciding at which levels of the social ecological model the programme intended to intervene.
{kind=link}
The social ecological model. NGO, non-governmental organisation.
Then, we undertook a final search by looking at the citations of included papers, as well as adding papers that the authors knew would meet the inclusion criteria, but due to the heterogeneity and complexity of the construct(s), were not captured in earlier searches. Following another around of inclusion screening of the newly identified papers, we added 17 articles to our extraction table. A total of 108 articles regarding 93 different programmes were included in our analysis.
As this content analysis is summative, our analysis largely consisted of summarising the extraction tool and identifying themes. The results section is in a large part a narrative summary of what was recorded in the extraction tables. To synthesise the broad swath of ‘lessons learnt’, we grouped all lessons learnt listed in the extraction table into categories that emerged from the data, for example, ‘resistance’ and ‘stigma’.
We analysed the articles working from the premise that power dynamics could be addressed at any level, including systemic power dynamics. For example, a programme that reached a large number of people could contribute to social norm change. In our summation, we also explore the distribution of programmes within the social ecological model, including to what extent programmes address multiple levels or directly address law, policy and institutional practices.
We do recognise that, in practice, programmes are not implemented in a vacuum; they are implemented in a political economic context where other programmes, social movements and geopolitical trends shape the right to SRH. These factors outside of the programme will shape how effectively a programme effects changes in power dynamics, so it is simplistic to assert that a programme addressing one level of the social ecological model is necessarily more effective than another.
Finally, the themes emerging from the data were discussed among the first three authors and subsequently elaborated in brief memos through an iterative process that required returning to the articles. These memos were then collapsed into broader categories and developed into the discussion section.
We ensured trustworthiness by triangulating among papers as we identified and elaborated themes and being attentive to discrepant findings. Moreover, since our intent is descriptive rather than a meta-analysis of findings, threats to validity are less of a concern.
Patient and public involvement
Because this paper is not directly related to patient care, this research was done without patient involvement. Patients were not invited to comment on the study design and were neither consulted to develop patient-relevant outcomes or interpret the results nor invited to contribute to the writing or editing of this paper for readability or accuracy.
Given the somewhat academic nature of the research question, the public were not invited to participate. However, public participation in some form might be appropriate for future work that addresses some of the gaps and tensions identified in this paper.
Results
We present some basic attributes of the included papers, and then go on to present the programmes by level of the social ecological model.
Overview
For simplicity, we refer to ‘programmes’ in this paper, though some of these may have been described as ‘interventions’ or ‘efforts’ in the papers we reviewed. The papers included describe programmes undertaken in diverse regions that address different elements of SRH, and for which power functions in manifold ways. Online supplemental table 1 presents a high-level overview of the results, including the countries where the programme was implemented, the levels of the social ecological framework the programme engaged, the theoretical and other bases provided for the intervention, and the primary SRH domain of intervention.
Supplemental material
Most of the programmes took place in Africa (n=56), with South Africa (n=15), Kenya (n=8) and Uganda (n=7) being the most represented. Twenty-nine of the programmes were in Asia, with the majority (n=24) in India. There were five programmes in Latin America and one in Eastern Europe. There were no papers regarding the Western Pacific region. In terms of SRH domains addressed, HIV prevention and services to prevent and/or support survivors of intimate partner violence (IPV) or another type of violence were the most common, with 17 interventions focused on HIV prevention only, 11 focused on HIV and IPV/other violence and 29 focused on IPV/other violence only. None of the papers focused on comprehensive abortion care. Most papers reported experimental, quasi-experimental or quantitative preapproach–postapproaches to assessing impact (n=72), and were largely based in a biomedical or positivist framework. Twenty-one papers used exclusively qualitative methods or did not report an evaluation or study but simply described a programme. Of the programmes reviewed, only two were described as a governmental effort35 36; the rest were seemingly implemented by NGOs and/or universities (n=106), although these efforts typically collaborated with public sector facilities and other public sector actors. Discussion of the agency/institution implementing the programme was generally very limited, consistent with the biomedical orientation that the programme itself is an ‘exposure’, not the entity implementing the programme. On the other hand, some papers included more in-depth discussions of which organisation(s) implemented the programme, the context of the organisation and the implications for the programme.25 37–46
Theoretical basis
Many of the papers did not explicitly report the theoretical basis of the programme described, but they did summarise the extant evidence base and/or describe formative research as data that informed programme design (n=34). Others referenced one or more theories or models underlying the programme (n=39). As reflected in online supplemental table 1, many of the theoretical underpinnings were from the behavioural sciences and social cognitive theories; others used the theory of gender and power or Freirean approaches, and a few relied on diffusion or other theories focused on social networks. Many of the theory-based programmes were focused on the individual/interpersonal level, but some addressed multiple levels. Moreover, many programmes referred to multiple theories. Finally, several programmes were derived from more participatory or other bottom-up processes (n=6).
Several papers examined their study outcomes in the broader context of the evolving evidence base and theory regarding unresolved issues such as the link between IPV and women’s economic empowerment, and the combination of gender segregated and mixed gender groups in spurring change in gender norms.47–49
Individual/interpersonal
Most programmes addressed more than one level of the social ecological model. Approximately, a third (n=31) of the interventions were focused on the individual/interpersonal level only, and 36 others addressed the individual/interpersonal in combination with others. Most programmes provided counselling or education sessions to individuals and/or couples, often with a role-playing component or similar activity that aimed to help participants to enact the principles taught.50–69
Other counselling, training or awareness raising sessions intervening at the individual/interpersonal level aimed to change the behaviour of individuals in a position of power in a given context, including men in the community, school personnel or parents of girls.70–72 Regardless of the participants, programmes aiming to change the behaviour of individuals typically had some explicit content related to power dynamics, such as recognising and changing gender hierarchies,51 53 56 70 72–75 understanding the health impacts of gender and other power dynamics,73 76 human rights77 and joint financial decision-making.52 To promote implementation of the lessons taught, many programmes aimed to enhance participants’ commitment and capacity to act differently in their interpersonal interactions by teaching strategies ranging from problem-solving techniques and more assertive communication50 51 58 60 64 73 74 to self-defence,61 62 and enacting positive masculinity through anger management and conflict resolution.53 54 56 78 79 Some of the activities were for groups convened by the project, such as groups of students in school or classes for multiple families at once, but seemingly targeted groups for reasons of efficiency, or to promote discussion about personal concerns rather than to engender any collective action or change in a community level variable.36 56 66 73 77–82
Organisational
Twenty-eight programmes, just under a third of the total, addressed the organisational level. Some programmes explicitly aimed to build organisational capacity to identify and address power dynamics and how these constrain autonomy in the context of SRH.83 84 The most common organisational structure addressed was health facilities. For example, several programmes entailed health facility-led efforts to engage communities in expressing their priorities regarding quality of care; some of these had an explicit health facility accountability component.35 37 42 85–88 Other health sector programmes aimed to create change in the way organisations operate, including health facilities89–92; health and allied professional associations and other organisational stakeholders in SRH, including law enforcement93–95; schools96; and factories.97 For example, a school-based programme in Uganda supported teachers to exercise respectful leadership, such as through the practice of non-punitive discipline.96
Another group of programmes addressed organisations or entities that bridge the state–society intersection (meaning that they are governed by public sector and community actors), such as hospital committees or village health and sanitation committees. The desired impacts ranged from changing these organisations’ behaviours regarding SRH98 to creating new organisations or committees bridging state and society.99
Some programmes sought to build the capacity of community-based organisations to work on a particular area related to power and SRH, such as facilitating the right to a legal remedy for sex workers who experience GBV.100 One multicountry effort in Southern Africa did this on a regional level by engaging a variety of organisations, including health facilities, schools, local organisations and religious groups, with the particular constellation of groups engaged depending on the context. Specifically, the programme aimed to improve these organisations’ capacity to reorient HIV prevention activities to focus more on the ‘choice disabled’.83
Programmes intervening at the organisational level intended to influence power dynamics that were manifest at the organisational level as well as other levels, such as in interpersonal interactions. Many of the health facility-focused programmes aimed to foster the provision of respectful (maternity) care, such as programmes aiming to improve communication between providers and patients and their families; to ensure that providers do not employ condescending, demeaning or discriminatory language; and to support community monitoring of health facilities to prevent and document disrespect.91 92 101 102 To effect such change, some programmes created mechanisms of communication between health providers/facilities and communities to increase health system responsiveness,35 44 89 103 or introduced a birth companion or care navigator to change the dynamics of power between the patient and providers.104
Community
Fifty-three of the programmes—almost 60% of the total—addressed the community level; 11 of them focused solely on the community. Some of the analyses sought to compare programmes that engaged the community with those that did not.89 105 Most of the community-focused activities included community mobilisation and/or dialogue.38 42 71 83 87 89 97 103 105–109 In some cases, this mobilisation and dialogue was described as the community component of a programme trying to impel health system responsiveness to community SRH concerns.37 38 42 85–87 89 103 105
Other mobilisation efforts used community-based activities to shift community norms in ways that promote SRH equity, including through community theatre, community action groups and repeated community dialogues regarding issues such as the acceptability of IPV, gender norms and HIV stigma.25 47 83 95 99 100 110–114 Sometimes these efforts also aimed to promote critical consciousness using Freirean principles as a way to empower participants.94 A few programmes sought to build community awareness and shift norms by facilitating community sharing from smaller groups that had been convened on a specific SRH issue, such as HIV or IPV prevention.41 45 98 115
Many programmes endeavoured to change community norms by training opinion leaders, community action teams, community activists or ambassadors; these efforts often focused on shifting gender norms at the community level.44 75 113 116–119 For example, based on an analysis using John Gaventa’s Powercube, a framework for analysing power that helps users to identify opportunities for mobilisation and change, the SASA programme trained ordinary community members as activists, who were then mentored to conduct various activities to engage men, women and institutions in the community.119 A few programmes included activities to assess impact within communities—as opposed to just changes in individual attitudes—such as by asking community members about the frequency and type of their communication relating to issues targeted by the programme,46 or creating measures to assess community-level changes.120 121
Several programmes aiming to shift power relations at the community level were implemented by grassroots organisations or other types of community-based organisations. They created and amplified demand for change by working to decrease the acceptability of domestic violence, claiming human rights for sex workers or agitating for better quality maternal healthcare.25 37 38 40 42–44 These efforts were generally part of a longer term, iterative strategy that entailed multilevel engagement in order to effect change at multiple levels. For example, Balestra and colleagues and Dasgupta and colleagues describe a programme wherein grassroots women set their own goals related to maternal health and other issues and then collected evidence to use in their advocacy vis-a-vis local health facilities, as well as district and state managers and policy-makers.37 40
Several programmes engaged the media to cover the project concerned and/or to be a channel for communicating information or ideas that were intended to effect a change in norms and power relations.108 122 A few projects intervening at the community level did not aim to shift community power relations per se, but rather to create enabling conditions for changes in power dynamics at the interpersonal level, such as by raising awareness among stakeholders about the links between harmful gender norms and IPV, or between young age of marriage and maternal morbidity and mortality, and attempting to galvanise their support for change.90 97 102 123 124
Public policy/governance
Seventeen of the programmes reviewed addressed the public policy/governance level; none focused exclusively on this level. Some programmes included advocacy activities aiming to foster governmental commitment to the given SRH issue, such as by ensuring the involvement of local or national government leaders or entities in programme awareness raising activities.25 75 95 102 110 125 Others sought to change the ways that public sector actors operate, such as schools or medical training institutions, by changing policies.102 126 Civil society organisations made claims on policy-makers at the local or national level, including trying to alter the ideologies underpinning governance decisions37 40 43 45 or trying to hold the governmental accountable for failing to fulfil the right to SRH.127 Some programmes run by NGOs built capacity and/or supported individuals or organisations to engage in policy-making, including through engagement in electoral politics.39 41 85 101–103
Lessons learned
The papers described lessons learnt regarding programmes seeking to alter power relations in order to improve SRH. While the focus of this paper is on what the programmes did rather than the impact they had, we report on some of the key lessons presented insofar as these shed light on fundamental issues such as the combination and types of activities that comprise a programme. Not all papers reported programme results. Of those that did, many simply presented results and noted that the programme—understood as an exposure—worked or did not work. These focused on the viability of the programme theory without necessarily invoking power.
We present power-related lessons in table 3, according to the key themes invoked by the papers’ authors, as well as their framing of the theme. For example, some described community resistance as a barrier and discussed how they overcame it; others simply asserted that a particular approach had helped to minimise community resistance.
Key themes and power-related lessons learnt from SRH literature
Discussion
Nature of existing evidence about power in SRH programmes
This paper adds value by summarising what the academic public health community has chosen to test and research in terms of power relations and SRH, and by raising questions about how this corresponds to the significant task of effecting change in power relations to improve the right to SRH. We elaborate further.
The 93 programmes reviewed reflect a diversity of priorities and approaches to addressing power. Most programmes intervened at multiple levels simultaneously, including some programmes that were described as ‘structural’. The structural programmes tended to be more explicit about their objective to shift power relations, noting that an explicit power framing channelled participants’ priorities towards both upstream and proximate drivers of SRH inequities (eg, see Abramsky et al116). Others addressed multiple levels using a more typical programme theory that sought to change individual behaviours and proximate drivers.
Almost all of the programmes tried to influence individual knowledge and behaviour, as well as some of the proximal structures shaping individual ability to exercise agency, such as gender relations of power in sexual encounters. The research designs used were skewed toward (quasi) experimental and quantitative preappraoches/postapproaches and measuring success in terms of individual knowledge and reported behaviour change, reflecting a prevalence of positivist evidence in addressing power in programmes.
The predominance of positivist biomedical framing and study approaches of the programmes reviewed in this study stands in contrast to the diverse and deep body of research—ranging from ethnography to political science—that analyse the ways that power shapes SRH policy, programmes and population health.5 128 This broader literature of descriptive cross-sectional studies typically draw on paradigms from the social sciences, such as interpretivist and constructivist framings, that can enrich biomedical research by foregrounding social relations and constellations of causes of change. Such framings are often germane to programmes that aim to shift power relations.129 130 By contrast, the use of traditional public health measurement approaches to assess structural change, as more typically used in the programmes reviewed in this study, entails many challenges, including how to account for complexity and context and how to create measures that detect changes in power relations.12 25 131–137 Programmes that seek to alter power relations might incorporate real-time learning and adaptation, and encounter uncertain trajectories of change, including pushback. Time frame and methodological limitations may undermine the effectiveness and assessment of a programme, and undercut effective scale-up or adaption and replication as the influence of social and political context is not elucidated.138 139 In brief, both the programmes implemented and the methods used to assess their impact likely do not correspond to the multilevel determinants of structure and agency.
On the other hand, there was a subset of articles that focused on bottom-up efforts to build agency and mobilise collective power, typically led by NGOs working at the national and subnational levels. Overall, their approach was grounded in a human rights or social movements paradigm, and the focus of research included how these programmes were part of a longer process of changing both structure and agency, rather than a time-bound effort to increase quantifiable indicators.25 37 39 40 43 101 140
It is notable that none of the programmes described focused on abortion, although one included postabortion care in their efforts to improve respectful maternity care.102
The right to SRH as a governmental obligation
Perhaps in part because they are empirical research on programmes to address specific health concerns and behaviours, the studies reviewed are somewhat removed from the larger question of how governments can address the power-related drivers of SRH inequities. The right to health approach is based on the assumption that the government is the ultimate duty bearer mandated to respect, protect and fulfil the right to SRH.141 With few exceptions, the programmes reviewed were pilots or localised efforts. To be sure, many of these efforts were intended to produce evidence that can be diffused and used by governmental and other actors developing national strategies and scaled-up programming, and these scaled up efforts may not be documented in peer-reviewed literature. Nonetheless, the extent to which pilot evidence is useable to policy-makers and actually informs governmental programmes remains an important priority for research, support and advocacy.139 142 143
Relatedly, none of the programmes explicitly address the provision of SRH care within the private sector—both for profit and non-profit private actors. The private sector is a major provider of SRH services in many settings144 often responsible for over half of the services provided in a country, so programmes aiming to affect power as a determinant of SRH at the organisational level should consider the role played by the private sector.
Sustainability and scale
Almost all of the programmes reviewed were led by NGOs, universities or research institutions, though they typically were implemented within the public sector. This raises questions about governmental commitment and capacity; potential for scale; and researcher commitment, ability, and incentives to study governmental efforts. In other words, there is likely both a research gap and an implementation gap. The research gaps reflects the fact that funders typically fund NGOs and universities to study programmes, including those implemented in the public sector. The implementation gap likely exists because governments are unwilling to directly confront the power dynamics that shape the right to SRH, and/or because many programmes are piloted by non-governmental actors and then not subsequently scaled up and taken over by governments. On the one hand, non-governmental actors may have greater expertise to both research and provide rights-based care, particularly to marginalised groups.145 On the other hand, in many settings, the government is the only actor with the capacity to implement health programmes at scale. As a body of work, research needs to consider these questions if researchers aim to produce evidence that can influence the right to SRH over the long term and at scale.
Limitations
Our review has several limitations. First, the peer-reviewed literature is not an unbiased representation of the universe of action to address the power-related determinants of SRH. This limitation holds for almost any review of academic literature describing programme approaches, but it has specific implications for our paper. As compared with external interventions, social movement efforts are likely under-represented in the peer-reviewed global health literature, particularly in a literature search that takes an interventionist frame. At the same time, social movement efforts and grassroots advocacy on SRH are deep and long-standing, and integral to a comprehensive assessment of efforts to address power dynamics as these shape the right to SRH. Social movement and grassroots NGO action may be most significant for especially contentious SRH issues, such as abortion. Stigma relating to abortion and other issues may also contribute to their under-representation in research and, thus, in peer-reviewed literature. It is also possible that programmes that describe themselves as being transformative may in some way reinforce power relations; our summation of the article would not have detected that. As an illustration, a programme that purportedly seeks to change gendered power relations in SRH might not refer patients to abortions, even in contexts where abortion is permitted. This nuance might not come through in a peer-reviewed paper, but it would mean that the programme’s impact on power relations is more partial or complex than we could learn from the paper itself. In essence, the gap between the literature and reality may be especially pertinent in the case of SRH.
Second, this analysis did not include programmes that may inadvertently affect power relations by perpetuating harmful power relations,22 146 or the ways that power pervades SRH agenda setting, and research and evaluation itself.26 147 148
Third, much of the work that would address power as a determinant of SRH might not be explicitly related to SRH or be sensitive to the search terms we used, which combine SRH, programmes/intervention and power. For example, efforts to improve morale and job security among healthcare workers could help to lessen rude treatment of clients seeking maternal healthcare but may not be labelled as an SRH intervention. An effort to hold the government accountable for failing to deliver quality maternal health services in a national court or to change the laws related to abortion, age of consent, or the regulation sex work would address power dynamics shaping the right to SRH but would likely not be detected using search terms related to programmes.
Fourth, this analysis focuses on LMICs. There is growing recognition that truly ‘global health’ should indeed be global and not focus exclusively on LMICs. Indeed, the power dynamics shaping SRH may be shaped and influenced at the global level, and, even if not, have many commonalities across countries at all income levels, such as accelerating wealth inequality.149 The silo between HICs and LMICs is eroding, as it can stifle innovation, solidarity and learning.150 The need to develop new, widely accepted review methodologies that can accommodate literature from all over the world—such as a stratified sampling approach—to reviewing papers is urgent.
Fifth, because we addressed such a broad topic here, we were unable to zoom in on granular issues that may be of great importance to theory development. For example, the papers revealed different theories and findings regarding the creation of peer groups to foster individual empowerment, as opposed to creating peer groups to serve as a source of social capital or a mechanism for collective mobilisation. As another example, some programmes addressed sex workers as an at-risk group that needs to be empowered with health information and prevention tools, while other programmes addressed sex workers as a group that needs health information and tools as well as avenues for rights claiming and obtaining remedies for police harassment. These approaches make different assumptions about how power dynamics shape the right to SRH.
Conclusion
Power and the right to SRH is a big topic. This paper looks at a significant slice of that topic—how programmes seeking to improve the right to SRH address power. Despite the limitations of our approach, we identified key trends and themes, including the prevailing focus on behaviour change strategies, and the related use of research approaches that are focused on detecting changes therein. At the same time, especially in the context of HIV and/or GBV, there are many programmes that seek to affect change on multiple levels and that use complicated study designs that harness epidemiological approaches to assess change at multiple levels. Further development of these approaches and increased programme and research attention to power relations at the community, organisational and policy/governance levels would complement the behaviouralist research. This should be done in a way that links research back to its purpose: producing a body of evidence that together can start to answer the question of how to shift power dynamics in favour of the right to SRH, and that is useful to decision-makers in SRH programme development.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Veena Sriram and Kerry Scott kindly offered thought partnership and feedback on possible methods for the review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @martaschaaf, @globalstopp
Contributors MS, VB and SMT developed the methodology and reviewed the same 10 manuscripts to ensure the reliability of the inclusion and exclusion criteria. MS extracted the data and wrote the first draft of the paper. VB and SMT made substantial comments on the first draft, including writing new text. AI, GS and IA offered substantive input and drafted some text, particularly regarding the framing of the paper and discussion. All authors read and approved the final manuscript.
Funding This manuscript was developed with support from the United Nations Development Program (UNDP)-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP Research), a cosponsored programme executed by the WHO.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.