Article Text

Statistics from Altmetric.com
Tuberculosis (TB) is one of the leading causes of death globally from a single infectious agent, despite being a preventable and curable disease.1 A significant concern is the large number of people estimated to have TB who are currently not diagnosed or reported, which further increased during the COVID-19 pandemic from approximately 3–4 million in 2020 and only showed a partial recovery in 2021.1
The first WHO-recommended rapid diagnostic (WRD), endorsed by WHO in 2010, revolutionised the diagnosis of TB. It was simple to perform, produced results in under 2 hours and could detect resistance to rifampicin, one of the most potent drugs to treat TB. Over the years, evidence has shown WRDs are highly accurate, reduce time to treatment initiation, impact patient-important outcomes and are cost-effective.2 In the past decade, WHO has endorsed several WRDs, including products suited to different contexts.2
The WHO End TB Strategy adopted by all countries calls for all people with TB to be diagnosed with a WRD as an initial test by 2025.3 However, in 2021, only 38% of people with TB were tested with a WRD as an initial test,1 while only 25% of all TB diagnostic testing sites had access to WRDs.4 Lack of access and insufficient use of WRDs contribute to the large gap in the detection of TB and drug resistance. Most people with TB still undergo a smear microscopy test as the initial TB test or do not receive any bacteriological diagnosis. Smear microscopy has several limitations, the most notable being very low sensitivity and inability to detect drug resistance. Furthermore, patient pathway analyses and work on diagnostic cascades highlight the importance of a holistic and decentralised approach to improve timely access to WRDs at the primary healthcare level, where over 80% of people with TB first seek care.5–7 The lack of access to WRDs needs to be rapidly addressed, and plans to switch to WRDs should be accelerated in all high-TB burden countries.
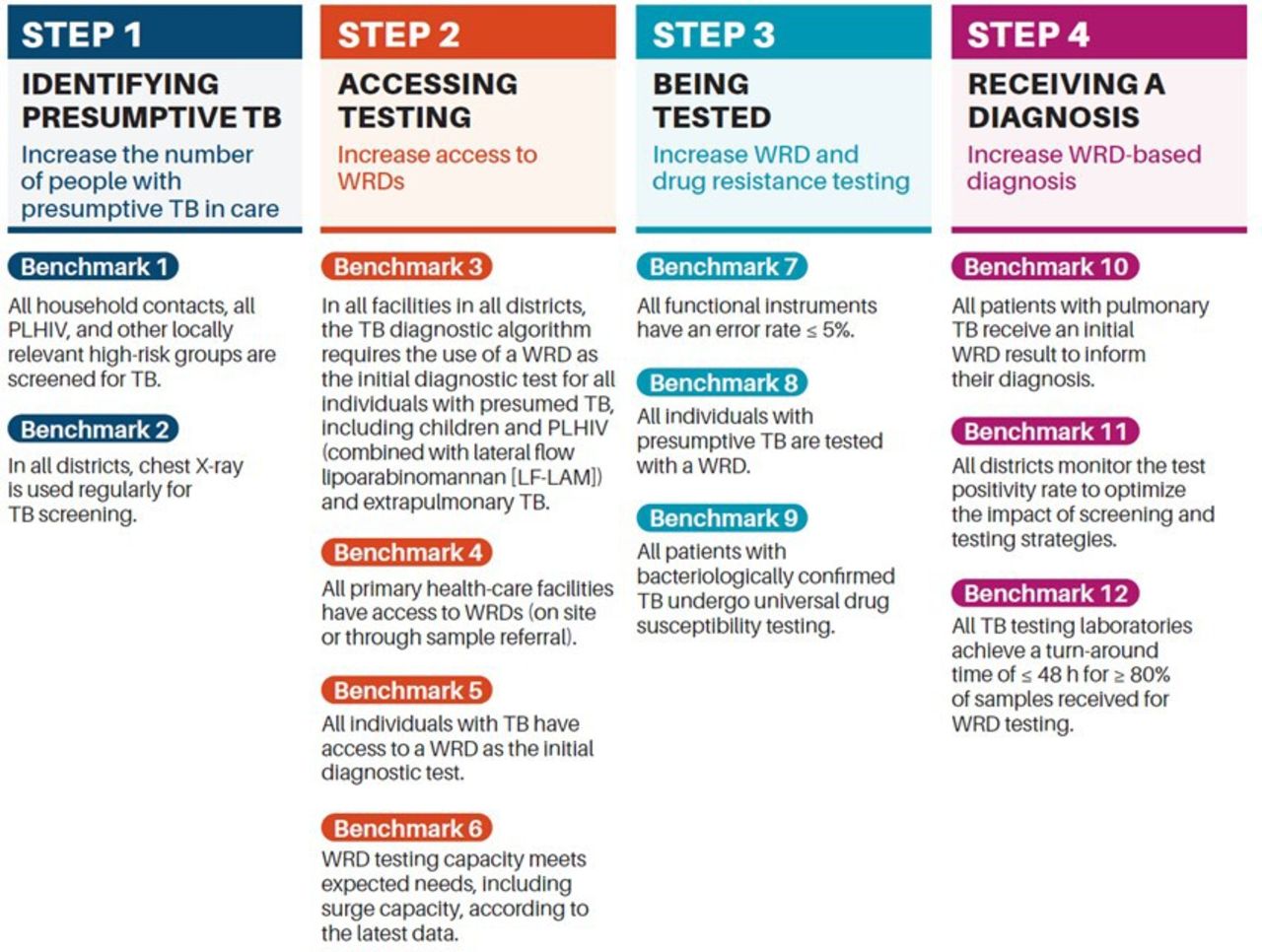
To facilitate the development of significant plans to scale up WRDs, the WHO, following extensive consultations, issued in April 2023 the WHO Standard: Universal Access to Rapid TB Diagnostics, with 12 benchmarks across four steps in a care cascade (figure 1) to achieve universal access to WRDs, increase bacteriologically confirmed TB and drug resistance detection, and reduce the time to diagnosis.4

{kind=link}
The WHO Standard: Universal Access to Rapid TB Diagnostics comprises 12 benchmarks to be completed by countries in the four steps of the diagnostic cascade: identifying presumptive TB, accessing testing, being tested and receiving a diagnosis. PLHIV, people living with HIV; TB, tuberculosis; WRD, WHO-recommended rapid diagnostic.
The benchmarks in the first step aim at identifying presumptive TB through the prioritisation of screening of high-risk groups and use of chest X-ray, which detects twice as many people with TB at early stages of the disease compared with symptom screening.8 The second step addresses access issues, including the availability of testing capacity and algorithms to deploy WRDs to reach the primary healthcare level and all individuals in need. The TB diagnostic algorithm requires using a WRD as the initial diagnostic test for all people with presumed TB. Additionally, all primary healthcare facilities must have access to WRDs, on-site or through sample referral.
The third step sets benchmarks for all individuals with presumptive TB to be tested with a WRD and undergo a drug susceptibility testing (DST), highlighting the importance of monitoring quality. Universal DST is defined as all people with bacteriologically confirmed TB to be tested as a minimum for resistance to rifampicin, all patients with rifampicin-resistant TB to be tested for resistance to fluoroquinolones, and all patients with resistance to rifampicin and fluoroquinolones for resistance to bedaquiline and linezolid. Recently, WHO endorsed shorter treatment regimens for all forms of TB, including TB infection, and drug-sensitive and drug-resistant TB. The diagnosis of all these forms of TB depends on the availability of rapid testing and universal access to DST. The last step sets benchmarks to achieve timely test results, promotes the use of data to optimise case detection and highlights the importance of addressing pulmonary TB, which contributes to disease transmission.
The WHO standard includes specific context-dependent benchmarks for the private health sector, as in some settings, more than a third of all people with TB are managed outside the national TB control programme.1 These benchmarks include screening at-risk populations (eg, healthcare workers and mine workers), ensuring availability of WRDs through public–private mix access models to reach all people with TB, and implementing a common diagnostic approach including universal DST and bacteriological confirmation of pulmonary TB.
The WHO standard presents a summary of evidence and experiences on barriers, enablers, solutions, approaches and implementation strategies to support the scale-up of WRDs. The findings of a systematic review and prospective qualitative study among stakeholders in high-burden countries are presented.4 They highlight the importance of combining high-quality, person-centred TB care with multicomponent strategies to address barriers at each health system level. Strong evidence was found on the importance of longitudinal stakeholder engagement to leverage innovative solutions such as optimised diagnostic networks and digital health technologies.
In addition, practical programme-derived solutions to overcome diagnostic access barriers are described. An example is a multicomponent strategy in Nigeria, where the instrument, standard operating procedure, solar panels and clinical training materials are all ‘packaged’ and shipped to each diagnostic site. Other helpful interventions identified include video-based refresher training to improve outreach, staff incentives to improve turnaround time, cross-use of WRD services between the public and private health sectors to improve access, and the use of short messaging services and other social media tools to enhance communication of test results and strengthen coordination in health programmes, respectively.
Many barriers have hampered the roll-out of WRDs, including a lack of political commitment, limited financial resources and technical challenges. The evidence synthesis shows that the technical barriers are not insurmountable. The enablers, solutions, approaches and strategies presented in the WHO standard can help overcome most technical challenges. The COVID-19 pandemic has shown that lack of political and financial commitments can also be overcome. These should no longer be considered barriers for a curable disease with high mortality.
Universal access to diagnosis is achievable and can be completed in record time, as seen from the massive efforts to scale up testing for COVID-19, with over 6 billion SARS-CoV-2 tests performed since the pandemic started.9 In just a single quarter (Q2, 2020) in the early period of the pandemic, the COVID-19 Diagnostic Consortium received orders from 44 countries for over 17 million molecular tests,10 exceeding the total number of WRDs procured annually by high TB burden countries after 10 years of scale-up. Investments in TB diagnostics are urgently needed and are very logical as diagnosing TB provides a superior cost:benefit ratio compared with many other diseases.11 Positive signs of increased commitment are emerging from some high-burden countries (eg, India),12 with others already showing the impact of renewed efforts (eg, Nigeria).1 The recent announcement of a 20% price reduction by one molecular diagnostic manufacturer,13 resetting the market space that has been slow to shift, will facilitate uptake and access.
While current WRDs will not fill all the gaps, they can at least narrow the margins and lay the foundations for emerging solutions. The next-generation urinary lateral-flow urine lipoarabinomannan technologies are promising, with a sensitivity expected to be better than the current smear microscopy, simple and fast enough for use during clinical encounters. Other technologies in development include a low-cost, battery-operated rapid nucleic acid amplification test that provides results within 30 min at an expected price well below the US$10 threshold and is suitable for sample types that are simpler to collect (eg, tongue swabs).
Up-front investment in better diagnostics will accelerate universal health coverage, resulting in better health for all and reducing the unacceptable mortality due to a curable and preventable disease such as TB. Strong political will and funding commitments in countries and by international agencies are necessary to ensure universal access to WRDs and universal DST.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors NI developed the first draft of the manuscript. MZ, C-MN and TK reviewed and provided further input.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.