Article Text

Statistics from Altmetric.com
Summary box
A majority of husbands do not separate from their wives with fistula following childbirth.
Factors associated with remaining married with fistula include whether the couple had children, fistula complexity and duration, date of fistula development, location, women’s age and husband’s education.
Women with fistula should be referred for treatment as soon as possible, before they spend time enduring the medical, psychological and social consequences of living with incontinence.
Living with obstetric fistula: learnings from nine African countries
Narratives can be useful. Stories draw us in, inspiring empathy and action. Such is the case with obstetric fistula, a maternal morbidity that occurs when women experience obstructed labour and are not able to access a timely caesarean section. Women with fistula are left continuously leaking urine, an embarrassing and difficult problem that typically can be resolved only by surgery. On top of the physical and emotional suffering caused by fistula, these women also experience the loss of their children because most of their babies do not survive during labour.1
Although obstetric fistula is completely preventable, humanity has created and continues to tolerate a reality in which not all women share similar access to high-quality healthcare. Obstetric fistula remains a challenge in rural settings in sub-Saharan Africa and South Asia where pregnant women do not have sufficient access to quality emergency obstetric care. Estimating fistula prevalence is challenging; perhaps one million women endure fistula, with 6000 new cases each year.2 The persisting burden of obstetric fistula reminds us of global health inequity, forcing us to see how health and social systems are failing to protect women and girls.
Women with fistula face significant physical and social constraints. They endure the shame of smelling of urine, often without appropriate materials to manage their incontinence. Many live with interrelated physical and medical problems affecting their daily activities. The pain and stigma caused by fistula push affected women to avoid public gatherings and social events.3 Furthermore, women with fistula are more likely than others to experience domestic violence.4 Sexual intercourse can be painful or not possible.5 6 It is a difficult reality for women and those who love them.
Dramatic stories seemingly encapsulate the misery of living with obstetric fistula: women with fistula are shunned, abandoned and isolated. This most dramatic story is not true for all women with obstetric fistula, however. In a compelling TED Talk (Technology, Entertainment, Design), Adichie urges us to avoid the ‘danger of a single story’—narratives that become definitive, eliminating nuance and putting a wedge in our efforts to understand one another.7 Single stories are incomplete. They do not sufficiently reflect the diversity of experiences and perspectives that constitute reality.
We wondered why some couples remain married through the ordeal of fistula while others do not. BMJ Open published our paper exploring this question: ‘Factors associated with marital status of women with genital fistula after childbirth: a retrospective review in nine African countries.’8 It is a retrospective review that draws from a large, multicountry dataset of women who sought fistula repair surgery in nine African countries: Ethiopia, Kenya, Malawi, Rwanda, Somalia, South Sudan, Tanzania, Uganda and Zambia. TJIPR, MM and colleagues collected data from women who presented for fistula repair between 1994 and 2017 and had developed fistula between 1975 and 2017.
Are all women with fistula divorced? No. Around 57% of the women included in our review were living with their husbands at the time that they sought fistula repair. Given that we review events that happened in the past, our analysis cannot draw conclusions about causes. Instead, we look at associations: variables that affect the odds of remaining married with fistula. We identified the following factors associated with remaining married with fistula:
Whether the couple had children (figure 1): Many people remain married to raise children together. Others have similarly found that previous births are associated with remaining married with fistula.9 10 We considered this indicator in different ways, including the birth number (parity) at which the woman developed fistula and the number of living children that she had when she sought out fistula repair. We had assumed that women who stayed married would be more likely to have children than women who separated, but surprisingly, this was not necessarily the case. Around 10% of women with fistula had a child between fistula development and fistula repair, without a statistically significant difference between those who remained married and who did not.
Complexity of the problem: Women who had both urinary and faecal incontinence separated more than women with urinary incontinence alone. Women who had unsuccessful surgeries to repair the problem separated more than women who were seeking out treatment for the first time.
Duration of the problem: We anticipated a steady decline in marriage over time while living with fistula. Instead, an initial sharp drop was followed by a flat line (figure 2). We interpret this to mean that the husbands who will leave typically do so in the first year or two.11
Date of fistula development: We found that the likelihood of remaining married with fistula decreased over the time period that we considered, 1975–2017. This probably reflects something true for the general population, although it is difficult to know without reliable data from civil registration systems.
Husband’s education: The woman’s level of education did not have a statistically significant connection to her likelihood of remaining married, but husbands who attended any school at all were more likely to stick with their wives than men who had not been to school.
Age: Women 20–35 were less likely to be separated than the women who developed fistula as teenagers or older women.
Location: Some countries had more marital separation among women with fistula than others. Controlling for other variables, probabilities ranged from 51.8% of women with fistula remaining married in Uganda to 69.4% of women with fistula remaining married in Zambia (figure 3).
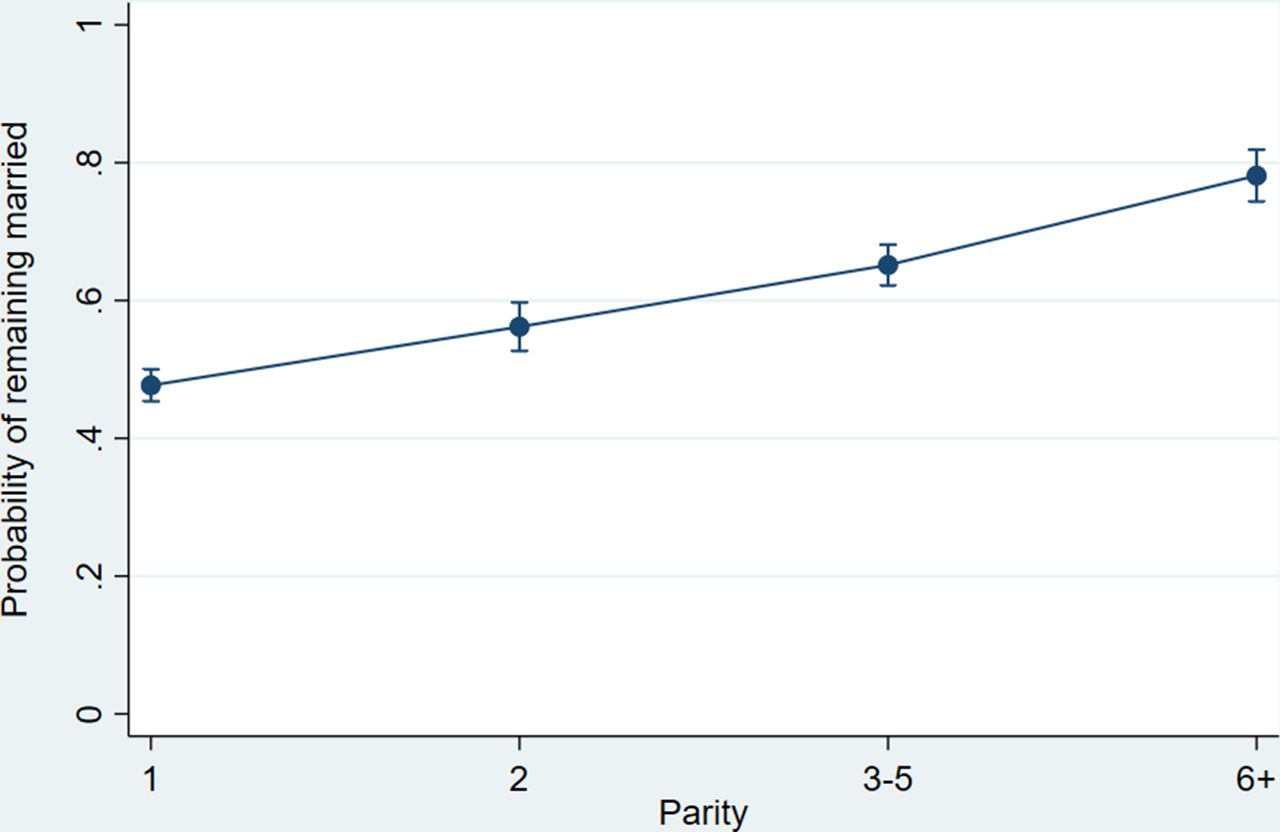
Predicted probability of remaining married with fistula by parity. Reproduced from Ngongo CJ et al.8

Predicted probability of remaining married with fistula by duration of incontinence. Reproduced from Ngongo CJ et al.8

{kind=link}
{kind=link}
{kind=link}
Predicted probability of remaining married with fistula by country. Reproduced from Ngongo CJ et al.8
Our analysis conveys that there is not a single story about life with fistula. We identified many factors associated with remaining married, even as we acknowledge that many reasons for continued marriage cannot be known. Every woman’s situation is unique.
Obstetric fistula has already been nearly eliminated in well-resourced settings. Quality emergency obstetric care must be made similarly available to women living in rural, low-resource settings. Until then, health providers must refer women who develop fistula for treatment as soon as possible, before they spend time enduring the medical, psychological and social consequences of living with incontinence.
Counselling can provide valuable, targeted support to both women with fistula and those who love them. While many husbands leave their wives with fistula, more than half stay married. Where appropriate, health providers and counsellors can seek to engage men as partners, encouraging husbands to support their wives on the journey back to health.
Data availability statement
Data generated and analysed during the current study are not publicly available during a period of analysis and dissemination but will be available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by AMREF Ethics and Scientific Review Committee P88/2013. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
RTI International funded this analysis through a professional development award. We appreciate travel support from the African Medical and Research Foundation (AMREF), EngenderHealth, the Fistula Foundation, the Freedom from Fistula Foundation, Gesellschaft für Technische Zusammenarbeit (GTZ; now GIZ), Johnson & Johnson, the Royal Netherlands Embassy of Tanzania, SOS East Africa, United Nations Population Fund (UNFPA), and Women and Health Alliance International (WAHA). The Fistula Foundation and the International Federation of Gynecology and Obstetrics (FIGO) paid the article processing charge. We thank the specialists and staff in the hospitals. Finally, we thank the women whose unforgettable experiences inform our conclusions.
Footnotes
Handling editor Seye Abimbola
Twitter @cngongo
Contributors Our commentary author list mirrors the authors on our paper published in BMJ Open (https://pubmed.ncbi.nlm.nih.gov/35613777/). CN and TJIPR formulated the study. TJIPR and MM collected the data. LL entered the data, with verification from TJIPR and curation by CN. CN analysed the data with statistical advice from DB and CB. CN wrote the paper. TJIPR, MM, LL, DB and CB reviewed and edited the paper. CN and TJIPR are guarantors, accepting full responsibility for the finished work.
Funding RTI International internal professional development award 0291013.201.102.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.